
Abstract
Purpose
In order to minimize the risk of transmission of coronavirus disease 2019 (COVID-19), many clinic appointments were postponed to lower patient attendance. Actively calling patients to postpone appointments is a labour-intensive process. We were the first ophthalmic clinics in Hong Kong to use short message service (SMS) to dispatch messages simultaneously to a large number of patients to offer postponement of appointments. The aim of this study is to evaluate whether SMS is an effective method to reduce outpatient attendance during the COVID-19 pandemic.
Methods
This is an observational study reviewing data on SMS messages sent to all patients attending ophthalmology clinics of a tertiary eye centre in Hong Kong. All SMS were sent at least 5 days before the scheduled appointments. The text message included an enquiry hotline for postponement of appointments and offered drug refill. The study included data from February to April 2020. Two hundred patients were invited to take part in a questionnaire on satisfaction level and reason(s) for appointment rescheduling.
Results
During the study period, a total of 17,028 SMS were sent. The overall response rate was 23.6%. 14.3% postponed their appointments. This led to an overall 13.9% reduction of clinic attendance. The overall satisfaction was high (96%). The main reason for postponing appointment was worries about infection risk (93.1%).
Conclusion
SMS was an efficient and cost-effective flow-control method which was well accepted by patients and can reduce outpatient attendance. The time saved can potentially allow healthcare workers to conduct other infection control measures during the COVID-19 pandemic.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The coronavirus disease 2019 (COVID-19) is a highly infectious disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). COVID-19 quickly evolved as a global threat since the first reported case in December 2019. The World Health Organization (WHO) officially declared COVID-19 a pandemic on 11 March 2020 [1]. Since then, there has been continuing exponential growth in both newly confirmed COVID-19 cases and death toll. More than five million people in the world were infected and more than 350,000 succumbed, most of them being elderly [2]. Strict border control, mandatory quarantine policy and lockdown measures have been implemented in various parts of the world including Hong Kong, in order to contain the virus and mitigate the spreading of the infection. It is of paramount importance to step up infection control measures including various flow-control methods in public premises, especially in high-risk areas like hospitals or clinics.
Globally, we, as ophthalmologists, are facing an ageing population and a growing demand for ophthalmic service. Most ophthalmic patients are elderly and most ophthalmic clinics are extremely congested. It has been shown that even subclinical patients are capable of transmitting the virus [3]. As a result, both patients and healthcare workers working in ophthalmology may be more vulnerable to COVID-19 infection. We previously described the use of a three-level hierarchy approach as a framework to minimize transmission in ophthalmology: administrative control, environmental control and the use of personal protective equipment [4,5,6,7]. Administrative control is the most important as it involves the largest amount of people and prevents their exposure to infected cases. Various flow-control measures can reduce the number of outpatient attendance to prevent cross-infection in this vulnerable group of patients. Despite active solicitation of patients at the entrance of the clinic to reschedule their appointments, it would be more desirable if patients are informed of this option well before their scheduled appointments.
The use of short message service (SMS) in healthcare is not novel in ophthalmology. Previous studies have reported its effectiveness in reducing non-attendance for postoperative paediatric cataract patients [8], diabetic retinopathy patients [9] and patients in general ophthalmic clinics [10, 11]. On the contrary, it appears the effectiveness of SMS to reduce patient attendance has not been previously studied.
Informing a large number of outpatients to reschedule their appointments is often challenging and extremely labour-intensive. In view of this, our department took advantage of SMS to send information to patients via their mobile devices, at least 5 days before their scheduled appointments. The message provided an enquiry hotline number, so that patients could call to postpone their appointments. Besides, the message also offered the option of drug-refill without follow-up. We hereby report the results of this initiative.
Methods
This is an observational study based on the data collected over a 2-month period, from February to April 2020. Our two ophthalmic outpatient clinics are located in United Christian Hospital and Tseung Kwan O Hospital in Hong Kong. Together the two hospitals serve the eastern region of Kowloon peninsula of the Hong Kong Special Administrative Region, with a catchment population of over 1,155,000. The annual outpatient attendance was 140,352 in 2019–2020. 57% (79,847) of these attendants were aged 65 or above. On average, the daily total attendance of our two outpatient clinics is around 500. Target groups of patients were identified using the hospital electronic Out-patient Appointment System (OPAS) using the specific appointment codes. We included all patients who had general ophthalmology clinic appointments in the first week. This was subsequently extended to include patients with appointments for subspecialty clinics, investigations (visual field, refraction) and minor operations, due to escalation of the COVID-19 outbreak locally. On every Wednesday morning, SMS text messages were sent out by the hospital Information Technology (IT) Department to patients with clinic appointments in the following week. Content of the SMS included (1) option of rebooking and drug refill via telephone hotline and (2) persuasion of patients with fever, flu symptoms or recent travel history to avoid ophthalmic clinic attendance. Chinese version of the SMS was sent to patients with Chinese names and English version was sent to patients with names of foreign ethnicity.
The text message read:
EYE CLINIC: Due to COVID-19, you can consider drug refill or calling xxxxxxxx to reschedule. Please seek medical help if recent travel history + fever/flu symptoms.
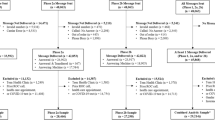
An ophthalmic nurse was responsible for answering the enquiry hotline and arranging appointment postponement. All cases were screened by ophthalmologists who would decide whether to accept the request for postponement, the duration of postponement and the need for drug-refill based on the clinical conditions at the most recent follow-up, as documented in the electronic record. The rescheduling was based on the following agreed protocol with one overarching principle: only patients with stable clinical conditions would be allowed to postpone their appointments. Patients with the following clinical conditions would need to keep their original appointment: (1) cases on systemic or topical steroids, (2) cases within two weeks postoperatively, (3) cases with uncontrolled intraocular pressure in the previous visits and (4) cases with conditions requiring frequent follow-ups. If the hotline was busy or if the patient called after office hours, calls were directed to a voicemail box and a nurse would subsequently return the calls (Fig. 1).

Workflow of using SMS for postponement of appointment. SMS short message service; IT information technology
To assess patients’ satisfaction to the SMS arrangement and their reasons for postponing their appointments, 200 patients were invited to take part in a questionnaire. Informed consent was obtained via the phone and patient privacy was respected (Fig. 2).

Questionnaire for patients who called the hotline on the SMS
Statistical analysis was performed using Microsoft Excel (Microsoft Corp., Redmond, WA, USA) and SPSS software version 26 (SPSS Inc., Chicago, IL, USA).
Results
During the 2-month period from February to April 2020, a total of 17,028 text messages were sent out successfully. The overall response rate was 23.6% (4011/17,028). Out of these 4011 patients, 60.8% (2439/4011) chose to postpone their appointments and 39.2% (1572/4011) chose to keep their original appointments. Overall, 14.3% (2439/17,028) of patients postponed their appointments, which led to a reduction of 13.9% of clinic attendance in the above period.
The weekly response rate was calculated. The peak of the weekly response rate (36.8%) coincided with the peak of the number of new COVID-19 cases (309) during the week of 22–28 March 2020. The Spearman’s rank correlation coefficient between the response rate and the number of new COVID-19 cases was 0.67, with p value of 0.07 (Fig. 3).

Correlation of response rate and number of new COVID-19 cases
Out of the 4011 patients who called the SMS hotline, 200 patients were selected, 100 from each clinic, to answer a questionnaire administered verbally over the phone by a nurse.
For the questionnaire results, the average age of the patients was 62. 49% were male and 51% were female. Out of the 200 responders, 192 (96%) were very satisfied or satisfied with the SMS arrangement (Fig. 4). Four patients (2%) reflected that the content of the SMS was unclear; they were unsure whether they needed to call back if they wished to keep their original appointments. 131 (65.5%) out of the 200 patients opted to reschedule their appointments. Out of those who postponed their appointments, 93.1% rescheduled as they were worried about infection risk, 2.3% had upper respiratory tract infection and 4.6% postponed for other reasons (Fig. 5).

Patients’ levels of satisfaction with the use of SMS for appointment arrangements

Patients’ reasons for postponing follow-up
The cost of sending a SMS was 0.06 US dollars (USD) per message. The total cost of sending SMS during the study period was USD $1,099. Instead of calling all 17,028 patients and asking them whether they wished to postpone their appointments, the nurse only needed to answer calls from 4011 patients. Assuming that it took three minutes on average for a phone call, the total time saved would be 651 h. Assuming a 44-h work week with 5-day work, this translates to 74 working days. The mean hourly salary of a registered nurse in the Hospital Authority in Hong Kong is approximately USD $30 [12] and labour cost of USD $19,530 was potentially saved over the 2-month period.
Discussion
Globally, healthcare workers are struck by the COVID-19 pandemic, leaving many unprepared. Because of the vulnerability of patients and healthcare workers in ophthalmology, healthcare workers globally have been working very hard to step up infection control measures. In countries with high surge of COVID-19 cases and their capacities of inpatient facilities compromised, even healthcare workers in ophthalmic fields may have to be deployed to help with the management of COVID-19 cases. In both scenarios, the overall manpower in ophthalmology may be very limited and labour-intensive calling of every case may not feasible.
Previous studies have reported the use of SMS for reducing non-attendance rate in ophthalmology clinics [8,9,10,11]. However, there appears to have no published study on using SMS to assist with reducing patient attendance during epidemics.
SMS messages have a number of merits, namely direct patient communication, instant delivery of messages and convenience. SMS is an efficient way to simultaneously dispatch a large number of messages [10], saving labour costs. Furthermore, with the global rise of scam calls in recent years, there is a tendency towards scepticism when receiving calls from unknown numbers, whereas patients who called the hotline were genuinely those who wished to postpone their appointments. The use of SMS may also be adopted during the recovery phase of clinical service when the current pandemic is over. It can allow patients to call the hotline to reschedule their missed appointment or make enquiries. SMS may also have a role in social distancing in busy ophthalmic outpatient clinics during the COVID-19 pandemic. Instead of waiting in a congested waiting room, it is possible that patients can wait in their own motor vehicles. SMS can be used to inform a patient when it is his or her turn to be attended by ophthalmologists to minimize the exposure of patients to infected cases.
Alternatively, the use of social media applications on mobile devices, such as WhatsApp or WeChat could be utilized to disseminate messages for free. In a recent study by Wan et al., they used the WeChat application to provide perioperative management during COVID-19 in China [13]. However, patients need to possess a smartphone with appropriate data plan and also install the application in order to receive messages. Our department did not utilize such apps as many ophthalmic patients are elderly and may not be using a smartphone or familiar with installation of messaging apps. To ensure all patients with a mobile phone (not necessarily a smartphone) will be able to receive messages, we used SMS instead of smartphone apps.
The study was conducted in April 2020 when the COVID-19 situation in Hong Kong was less severe compared with other parts of the world. We gave the option to patients to defer their appointments, and we did not actively postpone clinic appointments. From July 2020, Hong Kong had a new wave of COVID-19 cases, with the total number of infected cases tripled within a month (from around 1000 to over 3000). In response to this new wave of cases, our centre sent out SMS as in the original workflow. The overall response rate increased to 31.9% in July 2020. There appeared to be a correlation between the weekly response rate and weekly number of newly confirmed COVID-19 cases. Although this did not reach statistical significance, it appears to be in line with the results of our questionnaire, showing the majority of patients postponed their appointments due to fear of infection. Further studies to look into this psychological aspect of ophthalmic patients during COVID-19 may be warranted.
Limitations
The present study suffers all the shortcomings of any observational study. There was no control group that did not receive SMS. Thus it was not possible to perform detailed statistical analysis, such as calculating the “number needed to text” (NNT) to postpone one clinic appointment. The response rate to the SMS messages was affected by various factors, such as age, socio-economic status and incidence of new COVID-19 cases. The 200 patients who took part in the questionnaire were chosen without any randomization process. There may be participation bias, for example, very elderly patients may not be familiar with reading SMS and patients who were illiterate would not be able to respond. It was also possible that patients with Chinese names were only be able to read English and vice versa. Patients who did not provide a mobile phone number or provided an incorrect mobile phone number would not be able to receive the SMS messages. Due to cost issues, the number of characters was limited to 160 per text message and a minority of patients found the messages unclear. We also like to point out that the results of the present study may not be directly applicable to healthcare systems of other countries. Not only the stages of the COVID-19 pandemic may be different, there may also be differences in social, economic and cultural situations. Nevertheless, we believe our experience may allow global ophthalmologists to consider the use of SMS in the dissemination of information to a large number of patients during this pandemic.
Conclusion
The use of SMS during the COVID-19 pandemic led to a 13.9% reduction of outpatient appointments. SMS was an efficient and cost-effective flow-control method, which was well accepted by patients and can reduce outpatient attendance. The time saved can potentially allow healthcare workers to conduct other infection control measures during the COVID-19 pandemic.
Availability of data and material
Data and material can be provided upon request.
References
WHO Director-General's opening remarks at the media briefing on COVID-19 (2020) World Health Organization. https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020. Accessed 23 April 2020
COVID-19 coronavirus pandemic (2020). https://www.worldometers.info/coronavirus/. Accessed 29 May 2020
Bai Y, Yao L, Wei T, Tian F, Jin DY, Chen L, Wang M (2020) Presumed asymptomatic carrier transmission of COVID-19. JAMA 323(14):1406–1407. https://doi.org/10.1001/jama.2020.2565
Lai THT, Tang EWH, Chau SKY, Fung KSC, Li KKW (2020) Stepping up infection control measures in ophthalmology during the novel coronavirus outbreak: an experience from Hong Kong. Graefe’s Arch Clin Exp Ophthalmol 258(5):1049–1055. https://doi.org/10.1007/s00417-020-04641-8
Lai THT, Tang EWH, Fung KSC, Li KKW (2020) Reply to does hand hygiene reduce SARS-CoV-2 transmission? Graefe’s Arch Clin Exp Ophthalmol 258(5):1135–1135. https://doi.org/10.1007/s00417-020-04653-4
Lai THT, Tang EWH, Chau SKY, Li KKW (2020) Reply to ocular manifestation, eye protection, and COVID-19. Graefe’s Arch Clin Exp Ophthalmol 258(6):1341. https://doi.org/10.1007/s00417-020-04663-2
Wong DHT, Mak ST, Yip NKF, Li KKW (2020) Protective shields for ophthalmic equipment to minimise droplet transmission of COVID-19. Graefe’s Arch Clin Exp Ophthalmol 258(7):1571–1573. https://doi.org/10.1007/s00417-020-04683-y
Lin H, Chen W, Luo L, Congdon N, Zhang X, Zhong X, Liu Z, Chen W, Wu C, Zheng D, Deng D, Ye S, Lin Z, Zou X, Liu Y (2012) Effectiveness of a short message reminder in increasing compliance with pediatric cataract treatment: a randomized trial. Ophthalmology 119(12):2463–2470. https://doi.org/10.1016/j.ophtha.2012.06.046
Chen T, Zhu W, Tang B, Jin L, Fu H, Chen Y, Wang C, Zhang G, Wang J, Ye T, Xiao D, Vignarajan J, Xiao B, Kanagasingam Y, Congdon N (2018) A mobile phone informational reminder to improve eye care adherence among diabetic patients in rural China: a randomized controlled trial. Am J Ophthalmol 194:54–62. https://doi.org/10.1016/j.ajo.2018.07.006
Koshy E, Car J, Majeed A (2008) Effectiveness of mobile-phone short message service (SMS) reminders for ophthalmology outpatient appointments: observational study. BMC Ophthalmol 8:9. https://doi.org/10.1186/1471-2415-8-9
Brannan SO, Dewar C, Taggerty L, Clark S (2011) The effect of short messaging service text on non-attendance in a general ophthalmology clinic. Scott Med J 56(3):148–150. https://doi.org/10.1258/smj.2011.011112
Registered nurse (General)-(REF. NO.: KEC/C001/20) (2020). https://ha.taleo.net/careersection/ha_ext_cs/jobdetail.ftl?job=KEC/C001/20&tz=GMT%2B08%3A00&tzname=Asia%2FHong_Kong. Accessed 11 April 2020
Wang YH, Zhao LM, Liu ZY, Li XM (2020) Perioperative management by WeChat under the haze of COVID-19. Int J Ophthalmol 13(7):1161–1163. https://doi.org/10.18240/ijo.2020.07.22
Acknowledgements
The authors would like to dedicate this paper to all members of the Departments of Ophthalmology, the Information Technology Department and Specialist Outpatient Departments of United Christian Hospital and Tseung Kwan O Hospital. Special thanks to Mr. Kelvin Wong, Ms. Peggy Lam, Ms. Rachel Ng, Dr. Jeffrey Tse and Ms. Tebby Lee for their contributions to this project.
Funding
No funding was received.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by THTL. The first draft of the manuscript was written by THTL. EWHT and KKWL commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest or competing interests to declare.
Ethical approval
The study was performed in line with the principles of the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. The study protocol was approved by the research ethics committee of the Kowloon East Cluster of the Hospital Authority.
Informed consent
Informed consent was obtained from all participants included in the questionnaire study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Lai, T.H.T., Lee, M., Au, A.K.H. et al. The use of short message service (SMS) to reduce outpatient attendance in ophthalmic clinics during the coronavirus pandemic. Int Ophthalmol 41, 613–620 (2021). https://doi.org/10.1007/s10792-020-01616-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10792-020-01616-w