
Abstract
Purpose
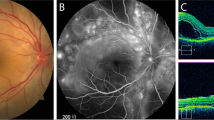
To identify prognostic factors for final visual outcome, development of complications, and recurrent inflammation in patients with Vogt-Koyanagi-Harada (VKH) disease.
Methods
All patients diagnosed with acute uveitis associated with VKH disease at the King Khaled Eye Specialist Hospital and King Abdulaziz University Hospital between January 1999 and February 2004 were reviewed. Data collected included age, gender, initial and final visual acuities, clinical findings at presentation, interval between onset of disease and starting treatment, treatment received, complications, number of recurrences, extraocular manifestations, and duration of follow-up period.
Results
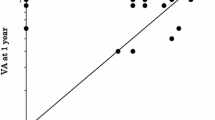
Sixty-eight patients were identified. There were 51 (75%) females and 17 (25%) males with a mean age of 25.04 ± 10.28 years (range 7–55 years). The mean follow-up period was 34.4 ± 20.1 months (range 8–62 months). The following factors were significantly associated with final visual acuity of 20/20 by univariate analysis: good initial visual acuity of better than 20/200 (p = 0.0415), absence of posterior synechiae of the iris at presentation (p = 0.0106), use of systemic corticosteroids for longer than nine months (p = 0.0479), slow tapering of systemic corticosteroids (p = 0.0024), absence of complications (p < 0.001), and absence of extraocular manifestations (p = 0.0124). Logistic regression analysis identified the use of systemic corticosteroids for longer than nine months to be associated with final visual acuity of 20/20 [odds ratio = 3.4; 95% confidence interval (CI) = 1.14–10.1]. The following factors were significantly associated with the development of complications by univariate analysis: age older than 18 years (p = 0.0161), initial visual acuity of 20/200 or worse (p = 0.0011), and presence of posterior synechiae of the iris at presentation (p = 0.0453). Factors identified after logistic regression analyses were age older than 18 years (odds ratio = 3.3; 95% CI = 1.33–8.17), and presence of posterior synechiae of the iris at presentation (odds ratio = 3.42; 9% CI = 1.38–8.47). Initial visual acuity of better than 20/200 was significantly associated with a lower risk of developing complications (odds ratio = 0.283; 95% CI = 0.129–0.629). The following factors were significantly associated with recurrent inflammation of three times or more by univariate analysis: initial visual acuity of 20/200 or worse (p = 0.0179), anterior chamber reaction of more than 2+ at presentation (p < 0.001), rapid tapering of systemic corticosteroids (p < 0.001), and development of extraocular manifestations (p = 0.0277).
Conclusions
Clinical findings at presentation, duration and method of tapering of systemic corticosteroids, and development of extraocular manifestations are significantly associated with final visual acuity, development of ocular complications, and recurrent inflammation. The development of ocular complications was significantly associated with a worse final visual acuity.
Similar content being viewed by others

References
Moorthy RS, Inomata H, Rao NA (1995) Vogt-Koyanagi-Harada syndrome. Surv Ophthalmol 39:265–292
Kobayashi H, Kokubo T, Takahashi M, Sato K, Miyokawa N, Kimura S, Kinouchi R, Katagiri M (1998) Tyrosine epitope recognized by an HLA-DR-restricted T-cell line from a Vogt-Koyanagi-Harada disease patient. Immunogenetics 47:398–403
Yamaki K, Gocho K, Hayakawa K, Kondo I, Sakuragi S (2000) Tyrosinase family proteins are antigens specific to Vogt-Koyanagi-Harada disease. J Immunol 165:7323–7329
Yamaki K, Kondo I, Nakamura H, Miyando M, Konno S, Sakuragi S (2000) Ocular and extraocular inflammation induced by immunization of tyrosinase related protein 1 and 2 in Lewis Rats. Exp Eye Res 71:361–369
Gocho K, Kondo I, Yamaki K (2001) Identification of autoreactive T cells in Vogt-Koyanagi-Harada disease. Invest Ophthalmol Vis Sci 42:2004–2009
Imai Y, Sugita M, Nakamura S, Toriyama S, Ohno S (2001) Cytokine production and helper T cell subsets in Vogt-Koyanagi-Harada disease. Curr Eye Res 22:312–318
Abu El-Asrar AM, Struyf S, Descamps FJ, Al-Obeidan SA, Proost P, VanDamme J, Opdenakker G, Geboes K (2004) Chemokines and gelatinases in the aqueous humor of patients with active uveitis. Am J Ophthalmol 138:401–411
Read RW, Rechodouni A, Butani N, Johnston R, Labree LD, Smith RE, Rao NA (2001) Complications and prognostic factors in Vogt-Koyanagi-Harada disease. Am J Ophthalmol 131:599–606
Ohno S, Minakawa R, Matsuda H (1988) Clinical studies of Vogt-Koyanagi-Harada’s disease. Jpn J Ophthalmol 32:334–343
Ohno S, Char DH, Kimura SJ, O’Connor GR (1977) Vogt-Koyanagi-Harada syndrome. Am J Ophthalmol 83:735–740
Read RW, Holland GN, Rao NA, Tabbara KF, Ohno S, Arellanes-Garcia L, Pivetti-Pezzi P, Tessler HH, Usui M (2001) Revised diagnostic criteria for Vogt-Koyanagi-Harada disease: report of an international committee on nomenclature. Am J Ophthalmol 131:647–652
Forrester JV, Ben Ezra D, Nussenblatt RB, Tabbara KF, Timonen P (1994) Grading of intermediate and posterior uveitis. In: Tabbara KF, Nussenblatt RB (eds) Posterior uveitis: diagnosis and management. Butterworth-Heinemann, Boston, pp 5–18
Rubsamen PE, Gass DM (1991) Vogt-Koyanagi-Harada syndrome. Clinical course, therapy, and long-term visual outcome. Arch Ophthalmol 109:682–687
Moorthy RS, Rajeev B, Smith RE, Rao NA (1994) Incidence and management of cataracts in Vogt-Koyanagi-Harada syndrome. Am J Ophthalmol 118:197–204
Forster DI, Rao NA, Hill RA, Nguyen QH, Baerveldt G (1993) Incidence and management of glaucoma in Vogt-Koyanagi-Harada syndrome. Ophthalmology 100:613–618
Moorthy RS, Chong LP, Smith RE, Rao NA (1993) Subretinal neovascular membranes in Vogt-Koyanagi-Harada syndrome. Am J Ophthalmol 116:164–170
Kuo IC, Rechdouni A, Rao NA, Johnston RH, Morgolis TP, Cunningham ET Jr (2000) Subretinal fibrosis in patients with Vogt-Koyanagi-Harada disease. Ophthalmology 107:1721–1728
Sonoda S, Nakao K, Ohba N (1999) Extensive chorioretinal atrophy in Vogt-Koyanagi-Harada disease. Jpn J Ophthalmol 43:113–119
Hayasaka S, Okabe H, Takahashi J (1982) Systemic corticosteroid treatment in Vogt-Koyanagi-Harada disease. Graefe’s Arch Clin Exp Ophthalmol 218:9–13
Keino H, Goto H, Usui M (2002) Sunset glow fundus in Vogt-Koyanagi-Harada disease with or without chronic ocular inflammation. Graefe’s Arch Clin Exp Ophthalmol 240:878–882
Rathinam SR, Vijayalakshmi P, Namperumalsamy P, Nozik RA, Cunningham ET Jr (1998) Vogt-Koyanagi-Harada syndrome in children. Ocul Immunol Inflamm 6:155–161
Tabbara KF, Chavis PS, Freeman WR (1998) Vogt-Koyanagi-Harada syndrome in children compared to adults. Acta Ophthalmol Scand 76:723–726
Acknowledgements
The authors thank Ms. Connie B. Unisa-Marfil for secretarial work.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Al-Kharashi, A.S., Aldibhi, H., Al-Fraykh, H. et al. Prognostic factors in Vogt-Koyanagi-Harada disease. Int Ophthalmol 27, 201–210 (2007). https://doi.org/10.1007/s10792-007-9062-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10792-007-9062-9