
Abstract
There is a growing trend towards the production of “hospital report-cards” in which hospitals with higher than acceptable mortality rates are identified. Several commentators have advocated for the use of Bayesian hierarchical models in provider profiling. These methods are frequently based upon the posterior probability that a hospital’s mortality rate exceeds a specific benchmark. However, the minimum probability level required for classifying a hospital as having higher than acceptable mortality has never been formally justified. We developed Bayes Rules for determining optimal probability levels so as to minimize mean posterior costs associated with false classifications under specific loss functions. Using Monte Carlo simulation methods we then determined the ability of posterior tail probabilities of unacceptable performance to accurately identify hospitals with higher than acceptable mortality.

Similar content being viewed by others

References
Alter, D.A., Naylor, C.D., Austin, P.C., Tu, J.V.: Long-term MI outcomes at hospitals with or without on-site revascularization. J. Am. Med. Assoc. 285, 2101–2108 (2001).
Austin, P.C.: A comparison of Bayesian methods for profiling hospital performance. Med. Decis. Making 22, 163–172 (2002).
Austin, P.C.: The reliability and validity of Bayesian methods for hospital profiling: a Monte Carlo assessment. J. Stat. Plan. Infer. 128, 109–122 (2005).
Austin, P.C., Anderson, G.M.: Optimal statistical decisions for hospital report cards. Med. Decis. Making 25, 11–19 (2005).
Austin, P.C., Alter, D.A., Tu, J.V.: The accuracy of fixed and random effects models in calculating risk-adjusted mortality rates: a Monte Carlo assessment. Med. Decis. Making 23, 526–539 (2003).
Berger, J.O.: Statistical Decision Theory and Bayesian Analysis. Springer-Verlag, New York, NY (1980).
Burgess, J.F. Jr., Christiansen, C.L., Michalak, S.E., Morris, C.N.: Medical profiling: improving standards and risk adjustments using hierarchical models. J. Health Econ. 19, 291–309 (2000).
Christiansen, C.L., Morris, C.N.: Improving the statistical approach to health care provider profiling. Ann. Intern. Med. 127, 764–768 (1997).
DeGroot, M.H.: Optimal Statistical Decisions. McGraw-Hill, New York (1970).
Geweke, J.: Evaluating the accuracy of sampling-based approaches to calculating posterior moments. In: Bernardo, J.M., Berger, J.O., Dawid, A.P., Smith, A.F. (eds.) Bayesian Statistics 4, pp. 169–193. Clarendon Press, Oxford (1994).
Gilks, W.R., Thomas, A., Spiegelhalter, D.J.: A language and program for complex Bayesian modelling. Statistician 43, 169–178 (1994).
Gilks, W.R., Richardson, S., Spiegelhalter, D.J.: Introducing Markov chain Monte Carlo. In: Gilks, W.R., Richardson, S., Spiegelhalter, D.J. (eds.) Markov Chain Monte Carlo in Practice, pp. 1–19. Chapman & Hall, London (1996).
Goldstein, H.: Statistical information and the measurement of educational outcomes. J. R. Stat. Soc. A 155, 313–315 (1992).
Goldstein, H., Spiegelhalter, D.J.: League tables and their limitations: statistical issues in comparisons of institutional performance. J. R. Stat. Soc. A 159, 385–443 (1996).
Goldstein, H., Rasbash, J., Yang, M., Woodhouse, G., Pan, H., Nuttal, D., Thomas, S.: A multilevel analysis of school examination results. Oxford Rev. Educ. 19, 425–433 (1993).
Hofer, T.P., Hayward, R.A.: Identifying poor-quality hospitals. Can hospital mortality rates detect quality problems for medical diagnoses? Med. Care 34, 737–753 (1996).
Jacobs, F.M.: Cardiac Surgery in New Jersey in 2002: A Consumer Report. New Jersey Department of Health and Senior Services, Trenton (2005).
Localio, A.R., Hamory, B.H., Cocks Fisher, A., TenHave, T.R.: The public release of hospital and physician mortality data in Pennsylvania. A Case Study. Med. Care 35, 272–286 (1997).
Luft, H.S., Romano, P.S., Remy, L.L., Rainwater, J.: Annual Report of the California Hospital Outcomes Project. California Office of Statewide Health Planning and Development, Sacramento (1993).
Massachusetts Data Analysis Center: Adult Coronary Artery Bypass Graft Surgery in the Commonwealth of Massachusetts, January 1–December 31, 2002. Department of Health Care Policy, Harvard Medical School, Boston (2004).
McGlynn, E.A.: Introduction and overview of the conceptual framework for a national quality measurement and reporting system. Med. Care 41, I-1–I-7 (2003).
MRC Biostatistics Unit: BUGS Version 0.510. Cambridge, United Kingdom (1995).
Naylor, C.D., Rothwell, D.M., Tu, J.V., Austin, P.C., The Cardiac Care Network Steering Committee: Outcomes of coronary artery bypass graft surgery in Ontario. In: Naylor, C.D., Slaugher, P.M. (eds.) Cardiovascular Health Services in Ontario: An ICES Atlas, pp. 189–197. Institute for Clinical Evaluative Sciences, Toronto, Canada (1999).
New York State Department of Health: Coronary Artery Bypass Graft Surgery in New York State 1989–1991. New York State Department of Health, Albany, New York (1992).
Normand, S.L., Glickman, M.E., Gatsonis, C.A.: Statistical methods for profiling providers of medical care: issues and applications. J. Am. Stat. Assoc. 92, 803–814 (1997).
Pennsylvania Health Care Cost Containment Council: A Consumer Guide to Coronary Artery Bypass Graft Surgery, vol. 4. Pennsylvania Health Care Cost Containment Council, Harrisburg (1995).
Pennsylvania Health Care Cost Containment Council: Focus on Heart Attack in Pennsylvania. Research Methods and Results. Pennsylvania Health Care Cost Containment Council, Harrisburg (1996).
Raudenbush, S.W., Bryk, A.S.: Hierarchical Linear Models: Applications and Data Analysis Methods, 2nd ed. Sage Publications, Thousand Oaks (2002).
Scottish Office: Clinical Outcome Indicators, 1994. Clinical Resource and Audit Group, Edinburgh (1995).
Spiegelhalter, D.J., Aylin, P., Best, N.G., Evans, S.J.W., Murray, G.D.: Commissioned analysis of surgical performance using routine data: lessons from the Bristol inquiry. J. R. Stat. Soc. A 165, 191–231 (2002).
Thomas, J.W., Hofer, T.P.: Accuracy of risk-adjusted mortality rates as a measure of hospital quality of care. Med. Care 37, 83–92 (1999).
Thomas, N., Longford, N.T., Rolph, J.E.: Empirical Bayes methods for estimating hospital-specific mortality rates. Stat. Med. 13, 889–903 (1994).
Tu, J.V., Pashos, C.L., Naylor, C.D., Chen, E., Normand, S.L., Newhouse, J.P., McNeil, B.J.: Use of cardiac procedures and outcomes in elderly patients with myocardial infarction in the United States and Canada. New Engl. J. Med. 336, 1500–1505 (1997).
Tu, J.V., Austin, P., Naylor, C.D., Iron, K., Zhang, H.: Acute myocardial infarction outcomes in Ontario. In: Naylor, C.D., Slaugher, P.M. (eds.) Cardiovascular Health Services in Ontario: An ICES Atlas, pp. 83–110. Institute for Clinical Evaluative Sciences, Toronto (1999a).
Tu, J.V., Naylor, C.D., Austin, P.: Temporal changes in the outcomes of acute myocardial infarction in Ontario, 1992–96. Can. Med. Assoc. J. 161, 1257–1261 (1999b).
Tu, J.V., Austin, P.C., Walld, R., Roos, L., Agras, J., McDonald, K.M.: Development and validation of the ontario acute myocardial mortality prediction rules. J. Am. College Cardiol. 37, 992–997 (2001a).
Tu, J.V., Austin, P.C., Chan, B.T.B.: Relationship between annual volume of patients treated by admitting physician and mortality after acute myocardial infarction. J. Am. Med. Assoc. 285, 3116–3122 (2001b).
Wennberg, D.E., Birkmeyer, J.D. (eds).: The Dartmouth Atlas of Cardiovascular Health Care. Centre for Evaluative Clinical Sciences, Dartmouth (1999).
Zhou, X.-H., Obuchowski, N.A., McClish, D.K.: Statistical Methods in Diagnostic Medicine. John Wiley & Sons, New York (2002).
Acknowledgements
The Institute for Clinical Evaluative Sciences (ICES) is supported in part by a grant from the Ontario Ministry of Health and Long Term Care. The opinions, results and conclusions are those of the author and no endorsement by the Ministry of Health and Long-Term Care or by the Institute for Clinical Evaluative Sciences is intended or should be inferred. Dr. Austin is supported in part by a New Investigator award from the Canadian Institutes of Health Research (Institute for Health Services and Policy Research). This research was supported in part by an operating grant from the Natural Sciences and Engineering Research Council (NSERC) of Canada. We would like to thank Dr. Geoffrey M. Anderson for useful discussions concerning the study.
Author information
Authors and Affiliations
Corresponding author
Appendix A. Schematic description of Monte Carlo simulations
Appendix A. Schematic description of Monte Carlo simulations
-
1.
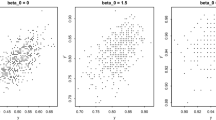
For each hospital, draw a random log-odds of mortality and a random slope from the following bivariate normal distribution:
$$ {\left( \begin{aligned} & \beta _{{0j}} \\ & \beta _{{1j}} \\ \end{aligned} \right)}\,\sim\,{\text{MVN}}{\left( {{\left( {\begin{array}{*{20}l} {{ - 2.063} \hfill} \\ {{0.913} \hfill} \\ \end{array} } \right)},{\left( {\begin{array}{*{20}c} {{0.081}} & {{0.022}} \\ {{0.022}} & {{0.023}} \\ \end{array} } \right)}} \right)},\quad j = 1, \ldots ,109. $$ -
2.
If exp (β0j /β 0) > 1.25 (where β0 = −2.063) then the jth hospital is defined to have higher than acceptable mortality (this is the gold standard). The analysis will then be repeated with thresholds of 1.3, 1.4 and 1.5.
-
3.
For each hospital, draw a hospital-specific mean illness severity score: \( \mu _{j}\,\sim\,N(0,{\text{SD}} = 0.159),\quad j = 1, \ldots ,110. \)
-
4.
For each patient at the jth hospital, randomly generate an illness severity score: \( X_{{ij}}\,\sim\,N(\mu _{j} ,{\text{SD}} = 0.989),\quad i = 1, \ldots ,n_{j} . \)
-
5.
For each patient, determine the patient-specific log-odds of death: \( \log {\left( {\frac{{p_{{ij}} }} {{1 - p_{{ij}} }}} \right)} = \beta _{{0j}} + \beta _{{1j}} X_{{ij}} . \)
-
6.
Randomly generate each patient’s vital status: \( Y_{{ij}}\,\sim\,{\text{Bernouilli}}(p_{{ij}} ). \)
-
7.
We have now randomly generated an illness severity score and an outcome for each patient at each of the 109 hospitals.
-
8.
We now fit a Bayesian hierarchical model to the randomly generated data.
-
9.
Using the simulated data, each hospital is classified as having either acceptable mortality or unacceptably high mortality.
-
10.
Sensitivity and specificity are determined.
-
11.
Steps 1 through 10 are repeated 100 times.
-
12.
The mean sensitivity and specificity is determined over the 100 simulations.
Rights and permissions
About this article
Cite this article
Austin, P.C., Brunner, L.J. Optimal Bayesian probability levels for hospital report cards. Health Serv Outcomes Res Method 8, 80–97 (2008). https://doi.org/10.1007/s10742-007-0025-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10742-007-0025-4