
Abstract
Aims
The objective of this study was to develop and validate an easy-to-use risk score (APRS) to predict which patients with acute pancreatitis (AP) will need intensive care unit (ICU) treatment within 48 h post-hospitalization on the basis of the ubiquitously available clinical records.
Methods
Patients with acute pancreatitis were retrospectively included from three independent institutions (RM cohort, 5280; TJ cohort, 262; SN cohort, 196), with 56 candidate variables collected within 48 h post-hospitalization. The RM cohort was randomly divided into a training set (N = 4220) and a test set (N = 1060). The most predictive features were extracted by LASSO from the RM cohort and entered into multivariate analysis. APRS was constructed using the coefficients of the statistically significant variables weighted by the multivariable logistic regression model. The APRS was validated by RM, TJ, and SN cohorts. The C-statistic was employed to evaluate the APRS’s discrimination. DeLong test was used to compare area under the receiver operating characteristic curve (AUC) differences.
Results
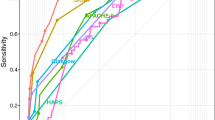
A total of 5738 patients with AP were enrolled. Eleven variables were selected by LASSO and entered into multivariate analysis. APRS was inferred using the above five factors (pleural effusion, ALT/AST, ALB/GLB, urea, and glucose) weighted by their regression coefficients in the multivariable logistic regression model. The C-statistics of APRS were 0.905 (95% CI 0.82–0.98) and 0.889 (95% CI 0.81–0.96) in RM and TJ validation. An online APRS web-based calculator was constructed to assist the clinician to earlier assess the clinical outcomes of patients with AP.
Conclusion
APRS could effectively stratify patients with AP into high and low risk of ICU admission within 48 h post-hospitalization, offering clinical value in directing management and personalize therapeutic selection for patients with AP.




Similar content being viewed by others


Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Lankisch PG, Apte M, Banks PA. Acute pancreatitis. Lancet 2015;386:85–96.
Argaiz ER, de Moraes AG. Acute pancreatitis. Lancet 2021;397:279–279.
Yadav D, Lowenfels AB. The epidemiology of pancreatitis and pancreatic cancer. Gastroenterology 2013;144:1252–1261.
Bumbasirevic V, Radenkovic D, Jankovic Z et al. Severe acute pancreatitis overall and early versus late mortality in intensive care units. Pancreas 2009;38:122–125.
Kaplan M, Ates I, Akpinar MY et al. Predictive value of C-reactive protein/albumin ratio in acute pancreatitis. Hepatobil Pancreat Dis Int 2017;16:424–430.
Zhang XX, Deng LH, Chen WW et al. Circulating microRNA 216 as a marker for the early identification of severe acute pancreatitis. Am J Med Sci 2017;353:178–186.
Silva-Vaz P, Abrantes AM, Castelo-Branco M, Gouveia A, Botelho MF, Tralhao JG. Multifactorial scores and biomarkers of prognosis of acute pancreatitis: applications to research and practice. Int J Mol Sci 2020;21:338.
Ranson JH, Rifkind KM, Roses DF, Fink SD, Eng K, Spencer FC. Prognostic signs and the role of operative management in acute pancreatitis. Surg Gynecol Obstet 1974;139:69–81.
Banks PA, Freeman ML. Practice Parameters Committee of the American College of G: practice guidelines in acute pancreatitis. Am J Gastroenterol 2006;101:2379–2400.
Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA et al. American-College of Chest Physicians Society of Critical Care Medicine Consensus Conference—definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Crit Care Med 1992;20:864–874.
Mounzer R, Langmead CJ, Wu BU, Evans AC, Bishehsari F, Muddana V et al. Comparison of existing clinical scoring systems to predict persistent organ failure in patients with acute pancreatitis. Gastroenterology 2012;142:1476–1482.
Park JY, Jeon TJ, Ha TH, Hwang JT, Sinn DH, Oh TH et al. Bedside index for severity in acute pancreatitis: comparison with other scoring systems in predicting severity and organ failure. Hepatobil Pancreat Dis Int 2013;12:645–650.
Papachristou GI, Muddana V, Yadav D, O'Connell M, Sanders MK, Slivka A, et al. Comparison of BISAP, Ranson's, APACHE-II, and CTSI scores in predicting organ failure, complications, and mortality in acute pancreatitis. Am J Gastroenterol 2010, 105:435–441; (quiz 442).
Tenner S, Baillie J, DeWitt J, Vege SS. American College of Gastroenterology guideline: management of acute pancreatitis. Am J Gastroenterol 2013;108:1400–1415.
Banks PA, Freeman ML, Amer PPC. Practice guidelines in acute pancreatitis. Am J Gastroenterol 2006;101:2379–2400.
Martinez J, Johnson CD, Sanchez-Paya J, de Madaria E, Robles-Diaz G, Perez-Mateo M. Obesity is a definitive risk factor of severity and mortality in acute pancreatitis: an updated meta-analysis. Pancreatology 2006;6:206–209.
Talamini G, Uomo G, Pezzilli R, Rabitti PG, Billi P, Bassi C et al. Serum creatinine and chest radiographs in the early assessment of acute pancreatitis. Am J Surg 1999;177:7–14.
Wu BU, Johannes RS, Sun XW, Conwell DL, Banks PA. Early changes in blood urea nitrogen predict mortality in acute pancreatitis. Gastroenterology 2009;137:129–135.
Pando E, Alberti P, Mata R, Gomez MJ, Vidal L, Cirera A, et al: Early changes in Blood Urea Nitrogen (BUN) can predict mortality in acute pancreatitis: comparative study between BISAP score, APACHE-II, and other laboratory markers-a prospective observational study. Can J Gastroenterol Hepatol 2021.
Lankisch PG, Weber-Dany B, Maisonneuve P, Lowenfels AB. High serum creatinine in acute pancreatitis: a marker for pancreatic necrosis? Am J Gastroenterol 2010;105:1196–1200.
Guidelines for intensive care unit admission, discharge, and triage. Task Force of the American College of Critical Care Medicine, Society of Critical Care Medicine. Crit Care Med 1999, 27:633–638.
Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG et al. Classification of acute pancreatitis-2012: revision of the Atlanta classification and definitions by international consensus. Gut 2013;62:102–111.
Riley RD, Ensor J, Snell KIE, Harrell FE, Martin GP, Reitsma JB, et al. Calculating the sample size required for developing a clinical prediction model. Bmj-Br Med J 2020, 368.
Sauerbrei W, Royston P, Binder H. Selection of important variables and determination of functional form for continuous predictors in multivariable model building. Stat Med 2007;26:5512–5528.
Jalali A, Alvarez-Iglesias A, Roshan D, Newell J. Visualising statistical models using dynamic nomograms. PLoS ONE 2019;14:e0225253.
Harrell FE, Califf RM, Pryor DB, Lee KL, Rosati RA. Evaluating the yield of medical tests. JAMA 1982;247:2543–2546.
Royston P. A remark on algorithm AS-181—the W-test for normality. Appl Stat 1995;44:547–551.
Boxhoorn L, Voermans RP, Bouwense SA, Bruno MJ, Verdonk RC, Boermeester MA et al. Acute pancreatitis. Lancet 2020;396:726–734.
Wu BU, Johannes RS, Sun X, Tabak Y, Conwell DL, Banks PA. The early prediction of mortality in acute pancreatitis: a large population-based study. Gut 2008;57:1698–1703.
Gajendran M, Prakash B, Perisetti A, Umapathy C, Gupta V, Collins L et al. Predictors and outcomes of acute respiratory failure in hospitalised patients with acute pancreatitis. Frontline Gastroenterol 2021;12:478–486.
Zhang YP, Liu C, Ye L, Yu N, Ye YN, Sun WR et al. Early prediction of persistent organ failure by serum angiopoietin-2 in patients with acute pancreatitis. Dig Dis Sci 2016;61:3584–3591.
Park JM, Shin SP, Cho SK, Lee JH, Kim JW, Kang CD et al. Triglyceride and glucose (TyG) index is an effective biomarker to identify severe acute pancreatitis. Pancreatology 2020;20:1587–1591.
Capparelli MA, D’alessandro PD, Questa HA, Ayarzabal VH, Bailez MM, Barrenechea ME. Development of a risk score for choledocholithiasis in pediatric patients. Pediatr Surg Int 2021;37:1393–1399.
Acknowledgments
Special thanks to S.W. and C.J. for their assistance with statistical analysis. Special thanks to L.X.F. and L.Y. for their expert technical assistance with radiological findings.
Funding
This work was funded by the National Natural Science Foundation of China (81901817, 62171230, U1809205, 61771249, 91959207, 81871352 and 92159301); Innovation Seed Funding of Wuhan University (TFZZ2018020); Hubei Provincial Key Laboratory Project (2021KYC0036).
Author information
Authors and Affiliations
Contributions
M.Y.J. and L.S. had the idea for and designed the study. L.Y. and X.Y.W. contributed to writing the paper. X.Y.W., S.W., Y.L., and P.X.H. contributed to data collection. L.Y. contributed to the statistical analysis. All authors contributed to data acquisition, data analysis, or data interpretation, and reviewed and approved the final version.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Yuan, L., Shen, L., Ji, M. et al. A New Risk Score to Predict Intensive Care Unit Admission for Patients with Acute Pancreatitis 48 Hours After Admission: Multicenter Study. Dig Dis Sci 68, 2069–2079 (2023). https://doi.org/10.1007/s10620-022-07768-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-022-07768-2