
Abstract
Background
Endoscopic variceal sequential ligation (EVSL) is currently endorsed in our hospital, as the preferred endoscopic treatment for prevention of variceal rebleeding and achieving adequate hemostasis. There is currently a lack of consensus surrounding EVSL-induced changes in esophageal motor function and abnormal reflux.
Aims
To explore alterations in esophageal motor function and risk of abnormal gastroesophageal reflux in liver cirrhosis patients with esophageal varices, after EVSL.
Methods
Twenty-one liver cirrhosis patients with esophageal varices were studied using manometry and 24-h pH monitoring 1 day prior to and 1 month following EVSL. The EVSL consisted of performing esophageal variceal ligation using a multi-band ligator, which was repeated every 4 weeks until the varices were eradicated.
Results
The amplitude and duration of peristaltic contraction waves and the percentage of abnormal esophageal contraction waveforms were unaltered in both the proximal (P > 0.05) and the distal (P > 0.05) esophagus after EVSL. However, the lower esophageal sphincter pressure was decreased following EVSL (16.1 ± 7.9 mmHg vs 21.1 ± 6.3 mmHg (P < 0.05)). Various quantitative parameters including percentage of total monitoring time with pH < 4.0, total number of reflux episodes, number of reflux episodes > 5 min, and DeMeester scores were not increased in post-EVSL patients. Abnormal reflux monitored by 24-h pH monitoring occurred in ten (47.6%) pre-EVSL patients and 11 (52.4%) post-EVSL patients.
Conclusions
Although EVSL affects esophageal motility by relatively decreasing LES pressure, it does not induce substantial motor abnormalities nor increase risk of abnormal gastroesophageal reflux disease in cirrhosis patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Liver cirrhosis is a chronic disease with significant prevalence worldwide, associated with high morbidity and mortality. Upper gastrointestinal (GI) bleeding following variceal rupture is a leading cause of death in liver cirrhosis patients with portal hypertension [1]. Traditional esophageal variceal ligation (EVL) introduced in 1986 is now advocated as a safe procedure for the treatment of esophageal variceal bleeding via mechanical blockade of variceal flow [2,3,4]. EVL has been accepted as the preferred endoscopic treatment for prevention of variceal rebleeding and achieving adequate hemostasis, with a lower rate of rebleeding, mortality, and complications than sclerotherapy [5]. However, EVL has been associated with a wide range of complications such as substernal pain, esophageal ulceration, stricture, perforation, and even death. Complications can occur in up to 40% of patients, while incidence of treatment-related death is 1% to 2% [6,7,8]. Currently, much controversy surrounds EVL-induced altered esophageal motor function such as changes in motility, described in some reports as transient and persistent in others [9, 10].
In our study, we performed endoscopic variceal sequential ligation (EVSL), which consists of performing esophageal variceal ligation every 4 weeks until variceal eradication for prophylaxis of variceal hemorrhage. EVSL has been advocated to be among the most efficient strategies available to control acute variceal hemorrhage and achieve adequate hemostasis, prevent rebleeding and decreasing mortality rates of patients with liver cirrhosis. The aim of our study was to investigate whether EVSL affects esophageal motility and causes abnormal gastroesophageal reflux.
Methods
This was a hospital-based clinical study conducted on patients with esophageal varices who underwent 24-h pH ambulatory recording and manometry of the esophagus before and after EVSL, in the Department of Gastroenterology of the Third Affiliated Hospital of Sun Yat-Sen University from January 2015 to January 2017. The Institute Research Committee and Institute Ethics Committee approved the study (Approved No. of ethic committee: [2014]2-145), and the study had been registered in Chinese Clinical Trial Registry (Registration number: ChiCTR-OOC-15005876).
Patients
Twenty-five patients with liver cirrhosis and esophageal varices were assessed for eligibility, and four patients were ineligible; one patient was found to have secondary liver carcinoma, and three patients did not complete the study. Twenty-one patients aged 18–75 years, with a previous history of variceal hemorrhage 1–12 months ago, who presented with no active bleeding on admission, were eligible for this study. All patients enrolled were nonsmokers and had no history of use within the preceding 2 weeks of acid-suppressant and motility drugs. The diagnosis of liver cirrhosis and esophageal varices was made on the basis of clinical history, physical examination, laboratory examination, ultrasound scan, and CT/MRI scan, and esophageal varices were evaluated by endoscopy. All patients, respectively, performed 24-h pH ambulatory recording and esophageal manometry 1 day prior to EVSL to obtain a baseline and 1 month following EVSL to observe the changes (Fig. 1).

Study design. Twenty-four liver cirrhosis patients with esophageal varices were assessed for eligibility; four patients were not eligible. Twenty-one patients were enrolled. The diagnosis of liver cirrhosis and esophageal varices was made on the basis of clinical history, physical examination, laboratory examination, ultrasound scan, and CT/MRI scan, and esophageal varices were evaluated by endoscopy. All patients performed 24-h pH ambulatory monitoring and esophageal manometry prior to and after EVSL. All the participants were inpatients at The Third Affiliated Hospital of Sun Yat-Sen University.
Exclusion Criteria
1. Patients with hepatic encephalopathy or other neuropsychiatric disorders; 2. Patients with Budd–Chiari syndrome or liver carcinoma; 3. Patients with unstable vital signs; 4. Patients with active gastrointestinal bleeding; 5. Patients with acute coronary syndrome, uncontrolled high blood pressure, or other severe cardiovascular diseases; 6. Patients with prior history of endoscopic treatment of esophageal varices; 7. Patients unable to complete the study.
Upper Gastrointestinal Endoscopy
In order to evaluate the severity of esophageal varices, all patients underwent standard upper gastrointestinal endoscopy and the varices were classified according to the Westaby classification system: Grade I: The esophageal varices collapse to inflation of the esophagus with air; Grade II: The esophageal varices are between grades I and III; Grade III: The esophageal varices are large enough to occlude the lumen [5, 6].
EVSL
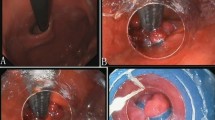
EVSL was performed with a multiple band ligator (Multi-Band Ligator SAEED SixShooter, Wilson-Cook Medical Co., Winston-Salem, USA). Ligation was first applied in the region of the gastroesophageal junction, with subsequent ligation applied at a distance interval of 2 cm in a helically cephalad direction; this procedure was then repeated to complete multiple ligations of individual channels at different levels, in the distal third of the esophagus. During each session, up to six bands were placed, and esophageal variceal ligation was repeated every 4 weeks until complete variceal obliteration [5] (Fig. 2a–f).

Procedure of the EVSL. a The esophageal varices were classified as Grade III prior to EVSL. b First session of EVSL. c, d The esophageal varices were alleviated after the initial session of EVSL. e Subsequent session of EVSL. f Successful eradication of esophageal varices after multiple sessions of EVSL
Esophageal Manometry
Esophageal manometry (EMN) was performed with an eight lumen, 4.5-mm-diameter polyvinyl catheter, locating the superior limit of the lower esophageal sphincter (LES) and using a low-compliance pneumohydraulic capillary infusion system (GAP-08A type, MedKinetic, China) for continuous perfusion with distilled water at a rate of 0.6 ml/min. In essence, the catheter was advanced through the nasal cavity down to the distal end of esophagus. Slow pull-through technique with catheter tractions with increments of 1.0 cm was used. The superior limit of the lower esophageal sphincter was designated as the place (in centimeters) immediately before the esophageal body pattern was recorded, usually where the tracing drops below the gastric baseline pressure. Manometric assessment of the esophagus was conducted in the supine position beginning at the LES. Both pressure at rest and relaxation of the LES during deglutition were measured. For assessment of the esophageal body, we used eight transducers. 5-mL wet swallows were given ten times on a 20- to 30-s interval. For assessment of the mid-esophagus part, the distal transducer was withdrawn an additional 1 cm and swallows given. The normative data were recorded by computerized software.
Twenty-Four-Hour pH Ambulatory Recording
Briefly, it was carried out with a portable digital system (HYW Type, Beijing Chang’an Henderson electronics co., LTD) composed of a catheter with an antimony electrode and an external reference electrode, placed 5 cm above superior limit of LES situated by manometry. The patient was asked to have a normal activity and have a normal diet without acidic fruits and soft drinks. Prior to the exam, proton pump inhibitors were discontinued at least 7 days, H2 blockers 72 h, and pro-kinetic agents 24 h, if in use. No antacids were used for duration of the examination. One reflux episode was arbitrarily defined as recording of an esophageal pH of less than 4 for at least 15 s. Abnormal reflux was defined as the period when the percentage of the total time of pH below 4 was greater than 4.5%, the frequency of long acid reflux episodes (esophageal pH less than 4 lasting more than 5 min) was greater than 50, and the DeMeester score was greater than 14.72.
Statistical Analysis
Statistical analysis was performed using SPSS 13.0 software. The quantitative data were compared using the Student’s t test for variables with a normal distribution, and the remaining data were expressed as median values. Comparisons of 24-h pH-metry and manometry parameters in pre- and post-EVSL patients were performed with the Wilcoxon’s signed test as the data were not expected to have a Gaussian distribution, P < 0.05 was considered to be significant.
Results
All 21 patients underwent manometry and 24-h ambulatory pH monitoring before and after EVSL, eighteen males and three females, aged 30–72 years; the mean age was 51.2 years and median age was 51 years. The etiology of cirrhosis was HBV in 15 patients, alcoholic induced in four patients, and of mixed (HBV and alcohol) etiology for the remaining two patients. Mean data changes from baseline, including liver function and coagulation function tests, are displayed in Table 1.
The esophageal varices of all patients were initially classified as Grade III on endoscopy. EVSL was performed on average 4.2 times and lasted 128 days from the initial band ligation session until variceal obliteration. Prior to EVSL, one patient complained of pyrosis and three of regurgitation. After EVSL, eight patients had chest pain within the first 48 h and one had dysphagia within 1 month, suggestive of altered esophageal motility. However, all these symptoms resolved rapidly, while no esophageal stricture was seen on follow-up endoscopy.
Twenty-Four-Hour pH Recording
The 24-h pH recordings show records of periods and percentage of the total monitoring time with pH below 4, the frequency of long acid reflux episodes (esophageal pH less than 4, lasting more than 5 min), and the DeMeester score, both before and after EVSL.
In this study, abnormal reflux was reported in ten (47.6%) pre-EVSL and 11 (52.4%) post-EVSL patients, with nine patients presenting with abnormal reflux pre- and post-EVSL. There was no significant statistical difference regarding the percentage of total monitoring time with pH < 4.0, total number of reflux episodes, number of reflux episodes > 5 min, and DeMeester scores between pre- and post-EVSL patients (Table 2).
Esophageal Manometry Findings
The lower esophageal sphincter pressure was significantly lower following EVSL compared to pre-EVSL (P < 0.05). However, there was no significant statistical difference in amplitude (P > 0.05) and duration (P > 0.05) of peristaltic contraction waves in both the proximal and the distal esophagus between pre- and post-EVSL patients (Table 3).
There were abnormal esophageal contraction waveforms both before EVSL and after EVSL on manometry; the percentage of abnormal waveforms both in the proximal and the distal esophagus was similar, with no statistically significant difference (P > 0.05). Motor dysfunction of the esophageal body was observed in six patients before EVSL and five after EVSL; however, the difference was not statistically significant (Table 4). Endoscopy performed on the patient who complained of dysphagia within 1 month after EVSL revealed no esophageal stricture, while esophageal manometry showed low-amplitude esophageal contractions and a high percentage of synchronized contractions waveforms.
Discussion
Our study showed that EVSL leads to changes in esophageal motility by decreasing the LES pressure; however, other parameters [11] such as amplitude and duration of peristaltic contraction were not significantly altered. The altered esophageal motility did not increase the number or duration of abnormal reflux episodes.
Although EVL-induced structural changes such as esophageal ulceration and stricture have been extensively reported, documentation of functional abnormalities of esophageal motility is scarce. Earlier studies have reported esophageal motility to be either diminished [12, 13] or unchanged [14]. Shortly after an EVL session (such as within 2 weeks), the acute local effects (edema, ulceration) may cause esophageal motility changes, which are often transient and reversible. Long-term changes in esophageal motility, usually associated with submucosal fibrosis in the esophageal wall, could not be observed in our study. Chen et al. reported a significantly shorter LES length in patients after EVL, while esophageal motility is barely altered [13]. Interestingly, we also found that the LES pressure was reduced after EVSL. We hence hypothesize that EVL actually normalizes LES pressure, which is usually elevated in liver cirrhosis patients with esophageal varices and does not induce abnormal esophageal motility. Twenty-four-hour ambulatory pH monitoring is regarded as the gold standard for diagnosis of GERD [15, 16]. In our study, no significant statistical difference was found regarding abnormal reflux in pre-EVSL and post-EVSL patients, as previous reported by Viazis et al. [17]. The esophageal pH of one patient with a prior history of mild gastroesophageal reflux was normalized following EVSL. Among two patients with new-onset abnormal reflux, one developed ascites due to hypoalbuminemia and was switched to Child–Pugh class C; the other patient initially with Child–Pugh class A liver function gained 7.5 kg with a BMI increase from 22.53 to 25.09; acid reflux was attributed to large volume ascites and obesity, respectively. Hence, we conclude that EVSL normalizes LES pressure, has little adverse impact on esophageal motility, and does not increase risk of gastroesophageal reflux. In our study, although abnormal reflux was recorded after EVSL, incidence of clinical symptoms was low, with one patient (4.7%) complaining of pyrosis and three patients (14.3%) of regurgitation.
The cause of the high prevalence of abnormal reflux in our study is yet unknown. Esophageal motor disorders and decreased amplitude of the peristaltic waves have been documented in cirrhotic patients with esophageal varices, compared to those without varices, including an asymptomatic control group [18]. However, since our study focused on pre- and post-EVSL patients, we could not assess the importance of this claim. Poor esophageal peristaltic wave progression and transient LES relaxation (TLESR) [19, 20] may account for changes documented in cirrhotic patients.
A shortcoming of our study includes use of conventional water-perfused manometry catheters, which precludes use of the Chicago Classification v3.0 of esophageal motility disorders. Another shortcoming was the small sample size of our study, despite the “minimally invasive” nature of both esophageal ambulatory 24-h pH monitoring and esophageal manometry found by most patients to be intimidating; we were hence unable to perform subgroup analysis of both cohorts. Further studies with greater sample size, comparing the frequency and severity of abnormal GER in cirrhotic patients with varying varix caliber and in those without varices, are essential for a better understanding.
References
Holster IL, Tjwa ET, Moelker A, et al. Covered transjugular intrahepatic portosystemic shunt versus endoscopic therapy + beta-blocker for prevention of variceal rebleeding. Hepatology. 2016;63:581–589.
Garbuzenko DV. Current approaches to the management of patients with liver cirrhosis who have acute esophageal variceal bleeding. Curr Med Res Opin. 2016;32:467–475.
de Franchis R, Baveno VIF. Expanding consensus in portal hypertension: report of the Baveno VI Consensus Workshop: stratifying risk and individualizing care for portal hypertension. J Hepatol. 2015;63:743–752.
Triantos C, Kalafateli M. Endoscopic treatment of esophageal varices in patients with liver cirrhosis. World J Gastroenterol. 2014;20:13015–13026.
Tripathi D, Stanley AJ, Hayes PC, et al. U.K. guidelines on the management of variceal haemorrhage in cirrhotic patients. Gut. 2015;64:1680–1704.
Van Stiegmann G, Goff JS. Endoscopic esophageal varix ligation: preliminary clinical experience. Gastrointest Endosc. 1988;34:113–117.
Dai C, Liu WX, Jiang M, Sun MJ. Endoscopic variceal ligation compared with endoscopic injection sclerotherapy for treatment of esophageal variceal hemorrhage: a meta-analysis. World J Gastroenterol. 2015;21:2534–2541.
Stiegmann GV, Goff JS, Michaletz-Onody PA, et al. Endoscopic sclerotherapy as compared with endoscopic ligation for bleeding esophageal varices. N Engl J Med. 1992;326:1527–1532.
Lo GH, Lin CW, Perng DS, et al. A retrospective comparative study of histoacryl injection and banding ligation in the treatment of acute type 1 gastric variceal hemorrhage. Scand J Gastroenterol. 2013;48:1198–1204.
Ghoshal UC, Saraswat VA, Aggarwal R, Misra A, Dhiman RK, Naik SR. Oesophageal motility and gastro-oesophageal reflux: effect of variceal eradication by endoscopic sclerotherapy. J Gastroenterol Hepatol. 1998;13:1033–1038.
Spechler SJ, Castell DO. Classification of oesophageal motility abnormalities. Gut. 2001;49:145–151.
Narawane NM, Bhatia SJ, Sheth MD, et al. Early changes in esophageal motility after endoscopic variceal sclerotherapy or ligation. Indian J Gastroenterol. 1999;18:11–14.
Chen SM, Lo GH, Lai KH, et al. Influence of endoscopic variceal ligation on oesophageal motility. J Gastroenterol Hepatol. 1999;14:231–235.
Berner JS, Gaing AA, Sharma R, Almenoff PL, Muhlfelder T, Korsten MA. Sequelae after esophageal variceal ligation and sclerotherapy: a prospective randomized study. Am J Gastroenterol. 1994;89:852–858.
Charbel S, Khandwala F, Vaezi MF. The role of esophageal pH monitoring in symptomatic patients on PPI therapy. Am J Gastroenterol. 2005;100:283–289.
Hirano I, Richter JE. Practice Parameters Committee of the American College of G: ACG practice guidelines: esophageal reflux testing. Am J Gastroenterol. 2007;102:668–685.
Viazis N, Armonis A, Vlachogiannakos J, et al. Effects of endoscopic variceal treatment on oesophageal function: a prospective, randomized study. Eur J Gastroenterol Hepatol. 2002;14:263–269.
Passaretti S, Mazzotti G, de Franchis R, Cipolla M, Testoni PA, Tittobello A. Esophageal motility in cirrhotics with and without esophageal varices. Scand J Gastroenterol. 1989;24:334–338.
Klauser AG, Schindlbeck NE, Muller-Lissner SA. Symptoms in gastro-oesophageal reflux disease. Lancet. 1990;335:205–208.
Mittal RK, McCallum RW. Characteristics and frequency of transient relaxations of the lower esophageal sphincter in patients with reflux esophagitis. Gastroenterology. 1988;95:593–599.
Funding
This study was funded by the National Natural Science Foundation for Young Scientists of China (81800458), the Science and Technology Developmental Special Foundation of Guangdong Province (2017B020226003), and the Science and Technology Planning Project of Guangdong Province Grant (2016A020216014).
Author information
Authors and Affiliations
Contributions
JT and BW developed the original concept and designed the study; JT, JZL, XLC, YWG, HT, XQW, FPZ, ZFW, and BW performed the study; JT supervised esophageal motility and 24-h pH monitoring; JT and BW analyzed the data and wrote the manuscript. All authors read and approved the final manuscript. All authors agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethics approval and consent to participate
The study protocol was approved by the Institute Research Committee and Institute Ethics Committee of Sun Yat-Sen University (Approved No. of ethic committee: [2014]2-145), and the study has been registered in Chinese Clinical Trial Registry (Registration number: ChiCTR-OOC-15005876). Signed informed consent was obtained from each patient for using materials and publication.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Tao, J., Li, J., Chen, X. et al. Endoscopic Variceal Sequential Ligation Does Not Increase Risk of Gastroesophageal Reflux Disease in Cirrhosis Patients. Dig Dis Sci 65, 329–335 (2020). https://doi.org/10.1007/s10620-019-05740-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-019-05740-1