
Abstract
Background and Study Aims
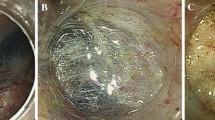
Varying degrees of fibrosis in colorectal endoscopic submucosal dissection (ESD) make the procedure difficult. Consensus on the predictive factors of fibrosis degree (mild or severe) has not been established. We conducted a study to identify the predictive factors and to examine the feasibility of ESD for fibrotic lesions.
Patients and Methods
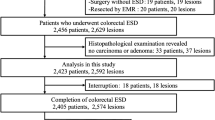
We included 518 patients who had undergone ESD for 558 lesions from April 2012–September 2018. Patients were classified into fibrosis or no-fibrosis groups, and logistic regression analysis was performed to identify predictive factors of fibrosis. Subgroup analyses were performed for fibrosis degree.
Results
The total incidence of fibrosis was 21.1% (mild: 14.1%; severe: 7.1%). Although the curative resection rate (free margin: invasion depth less than 1000 μm: no lymphatic invasion, vascular involvement) was lower in the fibrosis group compared with the control (80.7% vs. 97.6%), neither the en bloc resection rate (99.1% vs. 100%) nor incidence of perforation (0.9% vs. 0.2%) differed between the two groups. Multivariate analysis revealed that a cecal location, preoperative biopsy, straddling fold, laterally spreading tumor–non-granular-pseudo-depressed (LST-NG-PD) type were predictive of mild fibrosis. The presence of a straddling fold and a protruded lesion were independent predictive factors of severe fibrosis.
Conclusions
We identified the predictive factors of mild and severe fibrosis. It is preferable that a more experienced physician performs ESD for the lesions with F2 fibrosis.


Similar content being viewed by others

References
Torre LA, Bray F, Siegel RL, et al. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65:87–108.
Zauber AG, Winawer SJ, O’Brien MJ, et al. Colonoscopic polypectomy and long-term prevention of colorectal-cancer deaths. N Engl J Med. 2012;366:687–696.
Gorgun E, Benlice C, Abbas MA, et al. Experience in colon sparing surgery in North America: advanced endoscopic approaches for complex colorectal lesions. Surg Endosc. 2018;32:3114–3121.
Sauer M, Hildenbrand R, Oyama T, et al. Endoscopic submucosal dissection for flat or sessile colorectal neoplasia > 20 mm: a European single-center series of 182 cases. Endosc Int Open. 2016;4:E895–E900.
Chiba H, Ohata K, Ohno A, et al. Perforation with retroperitoneal emphysema after endoscopic submucosal dissection for a rectal carcinoid tumor. Endoscopy. 2010;42:E85–E86.
Arimoto J, Higurashi T, Chiba H, et al. Continued use of a single antiplatelet agent does not increase the risk of delayed bleeding after colorectal endoscopic submucosal dissection. Dig Dis Sci. 2018;63:218–227.
Arimoto J, Higurashi T, Kato S, et al. Risk factors for post-colorectal endoscopic submucosal dissection (ESD) coagulation syndrome: a multicenter, prospective, observational study. Endosc Int Open. 2018;6:E342–E349.
Chiba H, Ohata K, Tachikawa J, et al. Delayed bleeding after colorectal endoscopic submucosal dissection: When is emergency colonoscopy needed? Dig Dis Sci. 2018;64:880–887.
Makino T, Kanmura S, Sasaki F, et al. Preoperative classification of submucosal fibrosis in colorectal laterally spreading tumors by endoscopic ultrasonography. Endosc Int Open. 2015;3:E363–E367.
Imai K, Hotta K, Yamaguchi Y, et al. Preoperative indicators of failure of en bloc resection or perforation in colorectal endoscopic submucosal dissection: implications for lesion stratification by technical difficulties during stepwise training. Gastrointest Endosc. 2016;83:954–962.
Matsumoto A, Tanaka S, Oba S, et al. Outcome of endoscopic submucosal dissection for colorectal tumors accompanied by fibrosis. Scand J Gastroenterol. 2010;45:1329–1337.
Tamegai Y, Kisihara T, Fukunaga Y, et al. Endoscopic submucosal dissection for colorectal tumors accompanied by fibrosis in the submucosal layer. Gastroenterol Endosc. 2015;57:259–271.
Tanaka S, Kashida H, Saito Y, et al. JGES guidelines for colorectal endoscopic submucosal dissection/endoscopic mucosal resection. Dig Endosc. 2015;27:417–434.
Uraoka T, Saito Y, Matsuda T, et al. Endoscopic indications for endoscopic mucosal resection of laterally spreading tumours in the colorectum. Gut. 2006;55:1592–1597.
Hotta K, Yamaguchi Y, Saito Y, et al. Current opinions for endoscopic submucosal dissection for colorectal tumors from our experiences: indications, technical aspects and complications. Dig Endosc. 2012;24:110–116.
Watanabe T, Itabashi M, Shimada Y, et al. Japanese society for cancer of the colon and rectum (JSCCR) guidelines 2014 for treatment of colorectal cancer. Int J Clin Oncol. 2015;20:207–239.
Mizushima T, Kato M, Iwanaga I, et al. Technical difficulty according to location, and risk factors for perforation, in endoscopic submucosal dissection of colorectal tumors. Surg Endosc. 2015;29:133–139.
Kim ES, Cho KB, Park KS, et al. Factors predictive of perforation during endoscopic submucosal dissection for the treatment of colorectal tumors. Endoscopy. 2011;43:573–578.
Isomoto H, Nishiyama H, Yamaguchi N, et al. Clinicopathological factors associated with clinical outcomes of endoscopic submucosal dissection for colorectal epithelial neoplasms. Endoscopy. 2009;41:679–683.
Hotta K, Oyama T, Shinohara T, et al. Learning curve for endoscopic submucosal dissection of large colorectal tumors. Dig Endosc. 2010;22:302–306.
Seo M, Yang DH, Kim J, et al. Clinical outcomes of colorectal endoscopic submucosal dissection and risk factors associated with piecemeal resection. Turk J Gastroenterol. 2018;29:473–480.
Iacopini F, Saito Y, Bella A, et al. Colorectal endoscopic submucosal dissection: predictors and neoplasm-related gradients of difficulty. Endosc Int Open. 2017;5:E839–E846.
Pérez-Cuadrado-Robles E, Snauwaert C, Moreels TG, et al. Risk factors for conversion to snare resection during colorectal endoscopic submucosal dissection in an expert Western center. Endoscopy. 2019;51:152–160.
Suzuki T, Hara T, Kitagawa Y, et al. Feasibility of endoscopic submucosal dissection for cecal lesions. Scand J Gastroenterol. 2018;53:359–364.
Kim HG, Thosani N, Banerjee S, et al. Effect of prior biopsy sampling, tattoo placement, and snare sampling on endoscopic resection of large nonpedunculated colorectal lesions. Gastrointest Endosc. 2015;81:204–213.
Fukunaga S, Nagami Y, Shiba M, et al. Impact of preoperative biopsy sampling on severe submucosal fibrosis on endoscopic submucosal dissection for colorectal laterally spreading tumors: a propensity score analysis. Gastrointest Endosc. 2019;89:470–478.
Toyonaga T, Man-i M, Fujita T, et al. Retrospective study of technical aspects and complications of endoscopic submucosal dissection for laterally spreading tumors of the colorectum. Endoscopy. 2010;42:714–722.
Toyonaga T, Tanaka S, Man-I M, et al. Clinical significance of the muscle-retracting sign during colorectal endoscopic submucosal dissection. Endosc Int Open. 2015;3:E246–E251.
Chiba H, Ohata K, Takita M, et al. Double-tunnel method for treatment of colorectal lesions with severe fibrosis with endoscopic submucosal dissection. Endoscopy. 2018;50:E168–E169.
Fujihara S, Mori H, Kobara H, et al. The efficacy and safety of prophylactic closure for a large mucosal defect after colorectal endoscopic submucosal dissection. Oncol Rep. 2013;30:85–90.
Saito Y, Uraoka T, Yamaguchi Y, et al. A prospective, multicenter study of 1111 colorectal endoscopic submucosal dissections (with video). Gastrointest. Endosc. 2010;72:1217–1225.
Ohata K, Nonaka K, Minato Y, et al. Endoscopic submucosal dissection for large colorectal tumor in a Japanese general hospital. J Oncol. 2013;2013:218670.
Ohata K, Ito T, Chiba H, et al. Effective training system in colorectal endoscopic submucosal dissection. Dig Endosc. 2012;24:84–89.
Chiba H, Tachikawa J, Kurihara D, et al. Safety and efficacy of simultaneous colorectal ESD for large synchronous colorectal lesions. Endosc Int Open. 2017;5:E595–E602.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare they have no conflict of interest.
Ethical approval
The study was conducted in accordance with the principles laid down in the Declaration of Helsinki, and with the approval of the Institutional Review Board of our hospital (No.18-45).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Chiba, H., Tachikawa, J., Arimoto, J. et al. Predictive Factors of Mild and Severe Fibrosis in Colorectal Endoscopic Submucosal Dissection. Dig Dis Sci 65, 232–242 (2020). https://doi.org/10.1007/s10620-019-05735-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-019-05735-y