
Abstract
Introduction
Left ventricular assist devices (LVADs) are increasingly common in patients with advanced heart failure. GI bleeding (GIB) occurs in 20–30 % of these patients and can arise anywhere in the GI tract. Given the high rates of GIB in this population, our aim was to determine the diagnostic yield of repeated endoscopic evaluation in these patients.
Methods
We performed a retrospective review of all 257 patients who had LVADs placed between 2008 and 2013 at Duke University Hospital and identified all patients who underwent any endoscopic evaluation for GIB.
Results
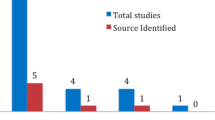
Of the 257 patients with LVADs placed, 78 (30 %) underwent at least one endoscopy for GIB. A source was identified in 36 % of cases, most commonly angioectasias (53.6 %). Treatment was performed in 67.9 % of patients and hemostasis was achieved in all. 64.1 % of the cohort underwent a second endoscopy for GIB. 42.9 % of these exams revealed a bleeding source. Endoscopic treatment was employed in 76.2 %. 38.5 % of the cohort underwent a third endoscopic exam for bleeding and a source was identified in 53.3 % with angioectasias remaining most common (56.3 %). By Fisher’s exact and Chi-square testing, only the presence of a bleeding source (p = 0.0034) and use of hemostatic therapy (p = 0.0127) on the index examination were significantly associated with re-bleeding.
Conclusions
GIB is common in patients with LVADs. The diagnostic and therapeutic yield of endoscopy is remains high with repeated interventions. Despite these high yields, a large portion of the cohort requires repeated interventions for recurrent bleeding.
Similar content being viewed by others


References
Kirklin JK, Naftel DC, Kormos RL, et al. Fifth INTERMACS annual report: risk factor analysis from more than 6,000 mechanical circulatory support patients. J Heart Lung Transplant. 2013;32:141–156.
Shrode CW, Draper KV, Huang RJ, et al. Significantly higher rates of gastrointestinal bleeding and thromboembolic events with left ventricular assist devices. Clin Gastroenterol Hepatol. 2014;12:1461–1467.
Stulak JM, Lee D, Haft JW, et al. Gastrointestinal bleeding and subsequent risk of thromboembolic events during support with a left ventricular assist device. J Heart Lung Transplant. 2014;33:60–64.
Singh G, Albeldawi M, Kalra SS, et al. Features of patients with gastrointestinal bleeding after implantation of ventricular assist devices. Clin Gastroenterol Hepatol. 2015;13:107.e1–114.e1.
Kushnir VM, Sharma S, Ewald GA, et al. Evaluation of GI bleeding after implantation of left ventricular assist device. Gastrointest Endosc. 2012;75:973–979.
Islam S, Cevik C, Madonna R, et al. Left ventricular assist devices and gastrointestinal bleeding: a narrative review of case reports and case series. Clin Cardiol. 2013;36:190–200.
Aggarwal A, Pant R, Kumar S, et al. Incidence and management of gastrointestinal bleeding with continuous flow assist devices. Ann Thorac Surg. 2012;93:1534–1540.
Raju GS, Gerson L, Das A, Lewis B, American Gastroenterological Association. American Gastroenterological Association (AGA) Institute medical position statement on obscure gastrointestinal bleeding. Gastroenterology. 2007;133:1694–1696.
Suarez J, Patel CB, Felker GM, et al. Mechanisms of bleeding and approach to patients with axial-flow left ventricular assist devices. Circ Heart Fail. 2011;4:779–784.
Meyer AL, Malehsa D, Bara C, et al. Acquired von Willebrand syndrome in patients with an axial flow left ventricular assist device. Circ Heart Fail. 2010;3:675–681.
Tsai HM, Sussman II, Nagel RL. Shear stress enhances the proteolysis of von Willebrand factor in normal plasma. Blood. 1994;83:2171–2179.
Crow S, Chen D, Milano C, et al. Acquired von Willebrand syndrome in continuous-flow ventricular assist device recipients. Ann Thorac Surg. 2010;90:1263–1269.
Letsou GV, Shah N, Gregoric ID, Myers TJ, Delgado R, Frazier OH. Gastrointestinal bleeding from arteriovenous malformations in patients supported by the Jarvik 2000 axial-flow left ventricular assist device. J Heart Lung Transplant. 2005;24:105–109.
Crow S, John R, Boyle A, et al. Gastrointestinal bleeding rates in recipients of nonpulsatile and pulsatile left ventricular assist devices. J Thorac Cardiovasc Surg. 2009;137:208–215.
Boyle AJ, Russell SD, Teuteberg JJ, et al. Low thromboembolism and pump thrombosis with the HeartMate II left ventricular assist device: analysis of outpatient anti-coagulation. J Heart Lung Transplant. 2009;28:881–887.
Menon AK, Götzenich A, Sassmannshausen H, et al. Low stroke rate and few thrombo-embolic events after HeartMate II implantation under mild anticoagulation. Eur J Cardiothorac Surg. 2012;42:319–323.
Najjar SS, Slaughter MS, Pagani FD, et al. An analysis of pump thrombus events in patients in the HeartWare ADVANCE bridge to transplant and continued access protocol trial. J Heart Lung Transplant. 2014;33:23–34.
Starling RC, Moazami N, Silvestry SC, et al. Unexpected abrupt increase in left ventricular assist device thrombosis. N Engl J Med. 2014;370:33–40.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
This work represents original research conducted within Duke University Health System research policies. Neither myself nor any of the authors listed above have any pertinent financial or professional conflicts of interest related to this study to disclose.
Rights and permissions
About this article

Cite this article
Dakik, H.K., McGhan, A.A., Chiu, ST. et al. The Diagnostic Yield of Repeated Endoscopic Evaluation in Patients with Gastrointestinal Bleeding and Left Ventricular Assist Devices. Dig Dis Sci 61, 1603–1610 (2016). https://doi.org/10.1007/s10620-015-4028-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-015-4028-7