
Abstract
Background
Patients with typical reflux symptoms (heartburn/regurgitation) persisting despite proton pump inhibitor (PPI) therapy are not uncommon. Impedance-pH monitoring detects gastroesophageal reflux at all pH levels and may establish if ongoing symptoms on PPI therapy are associated with acid/nonacid reflux. Laparoscopic fundoplication is a therapeutic option in such patients but reflux parameters on PPI therapy and after intervention and their relationship with symptom persistence/remission have been scarcely studied.
Aims
The aim of this study was to assess reflux parameters and their relationship with symptoms before and after laparoscopic fundoplication, on and off PPI therapy, respectively, in patients with PPI-unresponsive heartburn/regurgitation and with a positive symptom-reflux association and/or abnormal reflux parameters detected on PPI therapy.
Methods
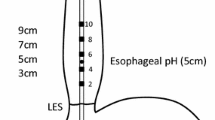
Impedance-pH monitoring was performed on high-dose PPI therapy and 3 months after laparoscopic fundoplication, off PPI therapy, in 40 patients with PPI-unresponsive heartburn/regurgitation. Symptoms were scored by a validated questionnaire.
Results
Esophageal acid exposure time as well as the number of total and proximal reflux events and of acid and weakly acidic refluxes decreased significantly after surgery: normal values were found in 100, 77, 95, 92 and 65% of cases, respectively. Weakly alkaline refluxes increased significantly postoperatively but neither before nor after intervention were associated with symptoms. All patients reported total/subtotal remission of heartburn/regurgitation 3 months after surgery.
Conclusions
Laparoscopic fundoplication improves acid and weakly acidic reflux parameters when compared with PPI therapy. This improvement justifies the very high post-surgical symptom remission rate that we observed. Prolonged follow-up is warranted but our findings strongly support the surgical option in PPI failures.



Similar content being viewed by others

Abbreviations
- GERD:
-
Gastroesophageal reflux disease
- PPI:
-
Proton pump inhibitor
- LES:
-
Lower esophageal sphincter
- DEA:
-
Distal esophageal amplitude
- GAET:
-
Gastric acid exposure time
- EAET:
-
Esophageal acid exposure time
- SAP:
-
Symptom association probability
- SI:
-
Symptom index
References
DeVault KR, Castell DO. Updated guidelines for the diagnosis and treatment of gastroesophageal reflux disease. Am J Gastroenterol. 2005;100:190–200.
Fass R, Shapiro M, Dekel R, Sewell J. Systematic review: Proton-pump inhibitor failure in gastro-oesophageal reflux disease—where next? Aliment Pharmacol Ther. 2005;22:79–94.
Fass R, Sifrim D. Management of heartburn not responding to proton pump inhibitors. Gut. 2009;58:295–309.
Sifrim D, Holloway R, Silny J, et al. Acid, nonacid, and gas reflux in patients with gastroesophageal reflux disease during ambulatory 24-hour pH-impedance recordings. Gastroenterology. 2001;120:1588–1598.
Vela M, Camacho-Lobato L, Srinivasan R, Tutuian R, Katz PO, Castell DO. Simultaneous intraesophageal impedance and pH measurement of acid and nonacid gastroesophageal reflux: Effect of omeprazole. Gastroenterology. 2001;120:1599–1606.
Hirano I, Richter JE, The Practice Parameters Committee of the American College of Gastroenterology. ACG practice guidelines: Esophageal reflux testing. Am J Gastroenterol. 2007;102:668–685.
Zerbib F, Bruley Des Varannes S, Roman S, et al. Normal values and day-to-day variability of 24-h ambulatory oesophageal impedance-pH monitoring in a Belgian–French cohort of healthy subjects. Aliment Pharmacol Ther. 2005;22:1011–1021.
Mainie I, Tutuian R, Shay S, et al. Acid and non-acid reflux in patients with persistent symptoms despite acid suppressive therapy: A multicentre study using combined ambulatory impedance-pH monitoring. Gut. 2006;55:1398–1402.
Zerbib F, Roman S, Ropert A, et al. Esophageal pH-impedance monitoring and symptom analysis in GERD: A study in patients off and on therapy. Am J Gastroenterol. 2006;101:1956–1963.
Bredenoord AG, Tutuian R, Smout AJPM, Castell DO. Technology review: Esophageal impedance monitoring. Am J Gastroenterol. 2006;101:1–8.
Castell DO. Reflux testing in the 21st century: Is there a role for pH only? Clin Gastroenterol Hepatol. 2008;6:840–841.
Pandolfino JE, Vela MF. Esophageal reflux monitoring. Gastrointest Endosc. 2009;69:917–930.
Frazzoni M, Grisendi A, Lanzani A, Melotti G, De Micheli E. Laparoscopic fundoplication versus lansoprazole for gastro-oesophageal reflux disease. A pH-metric comparison. Dig Liver Dis. 2002;34:99–104.
Frazzoni M, Lonardo A, Grisendi A, et al. Are routine duodenal and antral biopsies useful in the management of “functional” dyspepsia? A diagnostic and therapeutic study. J Clin Gastroenterol. 1993;17:101–108.
Sifrim D, Castell D, Dent J, Kahrilas PJ. Gastro-oesophageal reflux monitoring: Review and consensus report on detection and definitions of acid, non-acid, and gas reflux. Gut. 2004;53:1024–1031.
Kahrilas PJ, Shaheen NJ, Vaezi MF. American Gastroenterological Association Institute technical review on the management of gastroesophageal reflux disease. Gastroenterology. 2008;135:1392–1413.
Mainie I, Tutuian R, Agrawal A, Adams D, Castell DO. Combined multichannel intraluminal impedance-pH monitoring to select patients with persistent gastro-oesophageal reflux for laparoscopic Nissen fundoplication. Br J Surg. 2006;93:1483–1487.
Broeders JA, Draaisma WA, Bredenoord AJ, et al. Oesophageal acid hypersensitivity is not a contraindication to Nissen fundoplication. Br J Surg. 2009;96:1023–1030.
Hemmink GJM, Bredenoord AJ, Weusten BLAM, Monkelbaan JF, Timmer R, Smout AJPM. Esophageal pH-impedance monitoring in patients with therapy-resistant reflux symptoms: “on” or “off” proton pump inhibitor? Am J Gastroenterol. 2008;103:2446–2453.
Frazzoni M, Savarino E, Manno M, et al. Reflux patterns in patients with short segment Barrett’s oesophagus: A study using impedance-pH monitoring off and on proton pump inhibitor therapy. Aliment Pharmacol Ther. 2009;30:508–515.
Bredenoord AJ, Draaisma WA, Weusten BLAM, Gooszen HG, Smout AJPM. Mechanisms of acid, weakly acidic and gas reflux after anti-reflux surgery. Gut. 2008;57:161–166.
Zerbib F, Duriez A, Roman S, Capedont M, Mion F. Determinants of gastro-oesophageal reflux perception in patients with persistent symptoms despite proton pump inhibitors. Gut. 2008;57:156–160.
Tutuian R, Vela MF, Hill EG, Mainie I, Agrawal A, Castell DO. Characteristic of symptomatic acid reflux episodes on acid suppressive therapy. Am J Gastroenterol. 2008;103:1090–1096.
Scheffer RCH, Samsom M, Hebbard GS, Gooszen HG. Effects of partial (Belsey Mark IV) and complete (Nissen) fundoplication on proximal gastric function and esophagogastric junction dynamics. Am J Gastroenterol. 2006;101:479–487.
Roberts NB. Review article: Human pepsins—their multiplicity, function and role in reflux disease. Aliment Pharmacol Ther. 2006;24(Suppl. 2):2–9.
Bredenoord AJ, Weusten BLAM, Curvers WL, Timmer R, Smout AJPM. Determinants of perception of heartburn and regurgitation. Gut. 2006;55:313–318.
Vakil N, van Zanten SV, Kahrilas P, Dent J, Jones R, The Global Consensus Group. The Montreal definition and classification of gastroesophageal reflux disease: A global evidence-based consensus. Am J Gastroenterol. 2006;101:1900–1920.
Agrawal A, Roberts J, Sharma N, Tutuian R, Vela M, Castell DO. Symptoms with acid and nonacid reflux may be produced by different mechanisms. Dis Esophagus. 2009;22:467–470.
Aanen MC, Bredenoord AJ, Numans ME, Samson M, Smout AJPM. Reproducibility of symptom association analysis in ambulatory reflux monitoring. Am J Gastroenterol. 2008;103:2200–2208.
Pritchett JM, Aslam M, Slaughter JC, Ness RM, Garrett CG, Vaezi MF. Efficacy of esophageal impedance/pH monitoring in patients with refractory gastroesophageal reflux disease, on and off therapy. Clin Gastroenterol Hepatol. 2009;7:743–748.
Spechler JS. Surgery for gastroesophageal reflux disease: Esophageal impedance to progress? Clin Gastroenterol Hepatol. 2009;7:1264–1265.
Shay S, Tutuian R, Sifrim D, et al. Twenty-four hour ambulatory simultaneous impedance and pH-monitoring: A multicenter report of normal values from 60 healthy volunteers. Am J Gastroenterol. 2004;99:1037–1043.
Zentilin P, Iiritano E, Dulbecco P, et al. Normal values of 24-h ambulatory intraluminal impedance combined with pH-metry in subjects eating a Mediterranean diet. Dig Liver Dis. 2006;38:226–232.
Hila A, Agrawal A, Castell DO. Combined multichannel intraluminal impedance and pH esophageal testing compared to pH alone for diagnosing both acid and weakly acidic gastroesophageal reflux. Clin Gastroenterol Hepatol. 2007;5:172–177.
Campos GM, Peters JH, DeMeester TR, et al. Multivariate analysis of factors predicting outcome after laparoscopic Nissen fundoplication. J Gastrointest Surg. 1999;3:292–300.
Jackson PG, Gleiber MA, Askari R, Evans SR. Predictors of outcome in 100 consecutive laparoscopic antireflux procedures. Am J Surg. 2001;181:231–235.
Vakil N. Review article: The role of surgery in gastro-oesophageal reflux disease. Aliment Pharmacol Ther. 2007;25:1365–1372.
Roman S, Poncet G, Serray I, Zerbib F, Boulez J, Mion F. Characterization of reflux events after fundoplication using combined impedance-pH recording. Br J Surg. 2007;94:48–52.
Draaisma WA, Rijnhart-de Jong HG, Broeders IAMJ, Smout AJPM, Furnee EJB, Gooszen HG. Five-year subjective and objective results of laparoscopic and conventional Nissen fundoplication: A randomized trial. Ann Surg. 2006;244:34–41.
Competing interests
The authors have no competing interests to declare.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Frazzoni, M., Conigliaro, R. & Melotti, G. Reflux Parameters as Modified by Laparoscopic Fundoplication in 40 Patients with Heartburn/Regurgitation Persisting Despite PPI Therapy: A Study Using Impedance-pH Monitoring. Dig Dis Sci 56, 1099–1106 (2011). https://doi.org/10.1007/s10620-010-1381-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-010-1381-4