
Abstract
Background
Ulcerative proctitis (UP) is a prevalent condition associated with increased morbidity and mortality. Topical mesalamine (5-aminosalicylic acid [5-ASA]) inhibits inflammatory processes in UP.
Methods
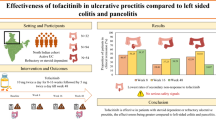
We evaluated effects of mesalamine 1-g suppository administered QHS compared with 500-mg suppository administered BID on UP activity (e.g., disease extension/mucosal appearance), remission, onset of response, safety and compliance in 97 patients with UP. A 6-week, randomized, multicenter, parallel-group, noninferiority study was conducted (and published) with Disease Activity Index (DAI) at week 6 as the primary efficacy variable and individual components of DAI at week 6 (i.e., stool frequency, rectal bleeding, mucosal appearance, global assessment) as secondary variables. Unreported outcomes were remission (DAI < 3 at weeks 3 and 6), disease extension, and complete response to treatment (DAI = 0; post-hoc, exploratory analysis).
Results
DAI values after 6 weeks were significantly reduced (±SD) from 6.6 ± 1.5 to 1.6 ± 2.3 (500-mg BID); and from 6.1 ± 1.5 to 1.3 ± 2.2 (1-g QHS). Mucosal appearance significantly improved from baseline after 3 and 6 weeks of treatment from 1.8 ± 0.5 to 0.8 ± 0.7 and 0.5 ± 0.7 (500-mg BID; P ≤ 0.0062) and from 1.7 ± 0.5 to 0.9 ± 0.5 and 0.4 ± 0.6 (1-g QHS; P ≤ 0.0001), respectively. Remission was comparable (78.3–86.1%); onset of response generally occurred within 3 weeks, and disease extension was reduced (>70%) after 6 weeks in both groups. Mesalamine was well tolerated. Compliance was >96%.
Conclusions
Mesalamine 500-mg BID and 1-g QHS suppositories are safe and effective for patients with UP. Most patients reported significant improvement within 3 weeks and UP remission and reduced disease extension after 6 weeks of treatment. Validity of QHS administration was confirmed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Ulcerative colitis (UC) is a chronic bowel disease defined by rectosigmoid mucosal inflammation and associated with immune system dysregulation [1–3]. Ulcerative proctitis (UP), a cryptogenic subset of UC, is differentiated by mucosal inflammation restricted to the rectum. Both UC and UP are symptomatically characterized by rectal bleeding, tenesmus, periodic diarrhea or constipation, and rectal pain [1]. Between 1 and 15 in 10,000 Americans have UC [1, 4], and up to 75% of newly diagnosed cases of UC may be UP [1]. Conversely, UP may progress to UC in up to 50% of affected patients [1].
The primary goals of managing UP include inducing and maintaining remission and healing the mucosa [3, 5]. Although oral formulations of 5-aminosalicylic acid (5-ASA), corticosteroids, and immunomodulators have been used successfully for disease management [6–8], data have demonstrated the effectiveness of topical formulations of these agents for the treatment of patients with UP [9–15]. Topical mesalamine (5-ASA delivered via suppository), which has been available for nearly two decades, inhibits prostanoid production, suppresses inflammatory cell action, and interferes with the transcriptional activation of genes encoding inflammatory mediators in the rectal mucosa in patients with UP [2, 6–13, 15, 16]. Further, preclinical studies have shown that topical mesalamine prevents the proliferation of colorectal cancer cells [17–19]. While most patients respond to BID dosing (i.e., one 500-mg mesalamine suppository in the morning and one at bedtime [QHS]), studies have shown that patients prefer taking a single 1-g mesalamine suppository QHS [10, 13].
These findings provided the basis for the selection of mesalamine doses (i.e., a 500-mg suppository BID or a 1-g suppository QHS) that were used in a 6-week, randomized multicenter study in patients with UP [20]. In that study, both mesalamine dosing regimens demonstrated comparable efficacy and safety, with similar compliance rates (only intent-to-treat [ITT] data were presented) [20]. The data reported herein are the results from additional analyses that were performed on the original population and confirm and expand upon those previously reported outcomes.
Materials and Methods
Study Design
A multicenter, randomized, parallel-group, noninferiority study was conducted to compare the efficacy and safety of a mesalamine 1-g suppository administered QHS and 500-mg suppositories administered BID (in the morning and QHS) in patients with active UP. The study protocol and amendments were reviewed and approved before submission to the appropriate institutions and regulatory agencies, and the trial was performed in accordance with the rules of Good Clinical Practice and was compliant with the Declaration of Helsinki.
Study Population
Eligible patients were male and non-pregnant non-lactating females, 18–70 years of age, with rectally confined UP confirmed by flexible sigmoidoscopy/colonoscopy (within 7 days of baseline measurements), and graded by a Disease Activity Index (DAI) value between 4 and 11 [21, 22]. Patients had mental and legal ability to provide written informed consent and could be smokers or non-smokers, but were not permitted to change their smoking habits during the 6-week study period. Patients were excluded if they had other digestive diseases (confirmed by histology and stool culture) that would interfere with DAI grading [23–25]. Patients were also excluded if they had UC that extended beyond the rectum (as determined by sigmoidoscopy/colonoscopy), if they chronically used oral 5-ASA (>4 g/day), any form of rectal 5-ASA, or any other medication for UP in the month preceding baseline measurements. The presence of clinically significant renal or hepatic impairment, urinary tract obstruction, coagulation disorders or use of anticoagulant drugs, other serious medical conditions, history of idiopathic pancreatitis, lack of use of reliable contraception (in women of child-bearing potential), and use of any experimental drug within 30 days of enrollment also excluded patients from the study.
Efficacy Evaluation
The primary objective of this study was to compare the clinical efficacy of two mesalamine suppository regimens in the treatment of patients with mild-to-moderate UP. The primary efficacy variable was DAI after 6 weeks of treatment. The DAI is a rating scale with four subscales: stool frequency, rectal bleeding, mucosal visualization at endoscopy, and disease global assessment [21]. Each subscale has four subdivisions of severity ranging from 0 (normal) to 3; the DAI score is the sum of all the subscales.
The secondary objectives of this study were to assess the remission rate (DAI < 3 at weeks 3 and 6), complete response to mesalamine after 3 and 6 weeks of treatment (DAI = 0), efficacy of the therapeutic regimens after 6 weeks of treatment versus baseline, effects of a concurrent maintenance dose of oral 5-ASA, the individual subscales of the DAI at week 6, and evaluation of safety and tolerability [23, 24]. Length of disease extension was recorded from endoscopy reports.
Efficacy and Safety Measures and Procedures
Patients were enrolled in the screening process after confirmation of willingness to participate and submission of informed consent. At the first visit, patients were instructed on how to complete the daily diary used to provide data for the DAI. A complete physical examination (excluding a genital/gynecologic examination, unless indicated) and endoscopy (with one rectal biopsy sample obtained from the most severely diseased area and one biopsy sample obtained from normal tissue above this area) were performed, medical history and demographic data were recorded, and routine hematologic, clinical chemistry, and pregnancy tests (if indicated), as well as urinalysis were completed (Fig. 1). Mucosal histology and/or stool cultures (demonstrating the absence of ova, parasites, pathogens or Clostridium difficile) confirmed patient admissibility. If a patient started medication on the basis of a positive diagnosis of UP and was later found negative by histology and/or culture, he or she was excluded from the ITT and efficacy analyses and was considered only for the safety analysis.

Investigational plan
A follow-up visit was performed after 3 weeks of treatment (i.e., between days 22 and 28). Endoscopy was performed and DAI was assessed by reviewing each patient’s diary and by questioning each patient about his or her symptoms over the previous 3 days (Fig. 1). Additional and continuing adverse events (AEs) and concomitant medications were recorded, and unused study medications were collected. New mesalamine and patient diaries were dispensed.
The third and final visit was performed after 6 weeks of treatment (i.e., between days 43 and 49) or as an end-of-treatment visit for patients who did not complete the trial (e.g., dropouts, randomized screening failures). Physical examination and the clinical laboratory tests (hematology, biochemistry, urinalysis, pregnancy tests) performed at the first visit were repeated. Another endoscopy was performed and the DAI value was recalculated by reviewing each patient’s diary, and patients were questioned about any symptoms experienced over the previous 3 days. AEs and concomitant medications were recorded, and unused study medications were retrieved (Fig. 1).
Compliance
Compliance was evaluated by suppository count at the second and last visits.
Statistical Analyses
Sample size calculations and justifications were based upon the ability to detect a difference of one DAI unit in the primary end point. After consideration of patient dropouts and withdrawals, it was calculated that 100 patients would be required for the study (with 50 patients randomized to each treatment; α = 0.05, power = 80%). Patients were randomly assigned to treatment groups in blocks of five. The study was open label.
The noninferiority of mesalamine 1 g QHS versus 500 mg BID was assessed through the following hypothesis: H01: U 1−U 2 ≥ 1.00 and H11: U 1−U 2 < 1.00. U 1 and U 2 represented the mean DAI value at week 6 in patients taking 1 g and 500 mg BID, respectively. A two-sided 90% confidence interval based on the comparison (U 1−U 2) was derived using the least square means from the ANCOVA model [26]. If the upper bound of this confidence interval was <1.00, it could be concluded that mesalamine 500 mg BID was at least as effective as mesalamine 1 g HS (i.e., non-inferiority).
Treatment by pooled site and baseline interaction terms were added separately. A significant interaction term (at 0.1 level) was included in the final model. Missing DAI data were estimated by the last-observation-carried-forward method for the ITT analysis.
All secondary efficacy parameters were evaluated in both the ITT and PP populations. The number and percentage of patients achieving remission (DAI < 3 at weeks 3 and 6) were presented descriptively within each treatment group, and the remission rate was tested using Fisher’s exact test. Complete response to the study drug (DAI = 0) was assessed after 6 weeks of therapy in each treatment group by comparing DAI changes at weeks 3 and 6 using a two-sided paired Student’s t test. The therapeutic response (DAI change at week 6) in patients receiving a maintenance dose of oral 5-ASA (≤4 g/day) compared with patients not receiving oral 5-ASA was assessed in both treatment groups using a Wilcoxon rank-sum test. The efficacy of the two mesalamine regimens was also assessed by comparing the DAI scores at baseline and week 6 using a two-sided paired Student’s t test and Pearson correlation (Spearman rank correlation if underlying assumptions were not met). The individual subscales of the DAI at week 6 were analyzed using an ANCOVA model and within-treatment comparisons. Length of disease extension was recorded a posteriori from individual endoscopy reports and analyzed in an exploratory manner. Only descriptive statistics were provided for safety parameters.
Results
Patient Disposition
Ninety-nine patients were recruited for this study, but two patients did not receive mesalamine, leaving 97 patients in the safety population (reported earlier [20]). Ten other patients did not meet inclusion or exclusion criteria, leaving 87 patients in the ITT population (Table 1). Eighty-three patients received the respective mesalamine treatment regimens and completed the study. Eighty-one patients were included in the PP analysis; 14 patients did not complete the 6-week study (Table 1).
Patient Demographics and Baseline Characteristics
Treatment groups did not differ significantly with respect to age or other baseline demographics between the ITT (reported earlier [20]) and PP populations (Table 2). A comparable percentage of patients in both treatment groups in the ITT and PP populations had a similar medical history and time since onset of UP (Table 2). There were no patients that were classified with active chronic colitis secondary to Crohn’s disease or active colitis that was inconsistent with inflammatory bowel disease (Table 2).
Primary Efficacy Evaluations
The use of mesalamine suppositories administered 500 mg BID or 1 g QHS reduced DAI values from baseline at week 3 and further reduced DAI values at week 6 in both the ITT (reported earlier [20]) and PP populations (Table 3). The between-group treatment differences in DAI values in weeks 3 and 6 were not statistically significant in the ITT or PP populations. As the upper bound of the confidence interval [−1.03; 0.69] was <1.00 unit, previously defined as clinical significance, it could be concluded that mesalamine 500 mg BID is as effective as 1 g QHS; these results were confirmed in both the ITT and PP populations.
Secondary Efficacy Evaluations
Treatment with mesalamine suppositories administered 500 mg BID and 1 g QHS improved individual components of the DAI after 3 weeks and furthered improved DAI values after 6 weeks. There was no difference between the mesalamine treatment groups in the ITT (reported earlier [20]) and PP populations with respect to stool frequency, rectal bleeding, endoscopic appearance, or global assessment (Table 4). Mucosal appearance was almost normal in both groups after 6 weeks of treatment in the ITT population. Further, there were no significant differences in remission rates after 3 weeks (~55%) or 6 weeks (~80%) of mesalamine therapy between treatment groups in both the ITT and PP populations (Table 4).
The time to onset of a clinical response, first assessed by comparing the mean DAI values at week 3 with values at baseline (Table 3), was statistically different (P < 0.0001 for the ITT and PP populations; data not shown) after 3 weeks of mesalamine therapy in both treatment groups, demonstrating that most patients responded within 3 weeks of the treatment initiation. Further, when comparing mean DAI values at weeks 3 and 6 (Table 3), data showed that the response to mesalamine was still increasing (P ≤ 0.0006 for both treatment groups in the ITT and PP populations; data not shown). There was no statistically significant difference in DAI values in either the mesalamine treatment group in the ITT or PP populations among patients who were or were not receiving oral 5-ASA maintenance therapy (data not shown).
Exploratory post-hoc analyses showed that the length of disease extension was reduced from 12.4 ± 5.4 cm (mean ± SD) at baseline to 3.5 ± 7.8 cm at week 6 in the mesalamine 500 mg BID group and from 10.5 ± 4.2 cm at baseline to 1.5 ± 3.2 cm at week 6 in the 1 g QHS group (Table 4). After 6 weeks of 500 mg BID therapy, 22 patients (41.5%) and 29 patients (54.7%) reported both complete response and resolved disease extension, respectively, compared with 15 patients (34%) and 25 patients (56.8%), respectively, in the 1 g QHS group.
Treatment Compliance
Compliance from first to last dose in both treatment groups in the ITT and PP populations was >96% (Table 4).
Safety Evaluation
Thirty patients (56.9%) in the mesalamine 500 mg BID group and 24 patients (54.5%) in the mesalamine 1 g QHS group reported treatment-emergent AEs (TEAEs) (Table 5). The most commonly reported TEAEs (reported earlier [20]) were in the gastrointestinal system (abdominal pain, flatulence, diarrhea, nausea) and the central nervous system (headache) (Table 5). Eight TEAEs classified as severe included abdominal pain (one patient in each treatment group), abdominal distension, frequent bowel movements, rectal hemorrhage, diarrhea, headache, and bronchospasm (all in the mesalamine 1 g QHS group). Three patients withdrew from the study because of treatment-limiting TEAEs (bronchospasm, increased headache intensity, worsening of clinical symptoms). No serious TEAEs were reported, and no deaths occurred during the study.
Discussion
While UP is associated with increased morbidity and mortality [1], few treatment guidelines have been published [3, 27]. Goals of therapy for UP call for mitigation of symptoms, including the reduction of rectal mucosal inflammation, prevention of flare-ups, and disease relapse [3]. One major reason for relapse is lack of treatment compliance [28]. Studies have shown that 47–86% of patients with UP will relapse if they remain untreated for 1 year [1].
Oral 5-ASA, corticosteroids, immunomodulators, biologic agents and antibiotics, alone or in combination, have been incorporated into UP treatment algorithms [1, 3], although new management strategies continue to emerge. Topical medications/suppositories containing 5-ASA [29], immunomodulators (e.g., tacrolimus) [11], and biologic agents (e.g., infliximab) [30] can prevent or mitigate the cascade of inflammatory events in the rectal mucosa, and reduce the morbidity and mortality associated with UP [3, 7]. Recommendations and strategies for the treatment of UP are shifting to incorporate these formulations [3, 6].
Guidelines have advocated the use of rectally administered mesalamine over topical steroids or oral 5-ASA for the treatment of patients with mild/moderate (and treatment-refractory) distal UC [3], and studies have shown that topical mesalamine is effective for symptomatic treatment [31], timely induction, and maintenance of remission in patients with UP [1, 7, 14, 22, 31, 32]. In one 4-week open-label trial, clinical remission was reported in 84% of patients (n = 50) treated with mesalamine suppositories QHS and in 80% of patients treated BID [10]. Data from a similar study in 251 patients with cryptogenic proctitis showed that mesalamine suppositories administered 500 mg BID or 1 g QHS were equally effective in mitigating the symptoms of UP [13]. The capacity of topical mesalamine to lower DAI values may be associated with its beneficial effects on rectal mucosal integrity, prostanoid production, and other mediators of mucosal inflammation [2, 17, 33–35]. Further, the onset of clinical response usually occurs within 3 weeks of treatment initiation. Remission rates documented in our study (~80%) are greater than those reported elsewhere (~70%) [29]. As in previously reported safety data [20], most of the TEAEs in this trial were gastrointestinal or central nervous system in nature, with no serious TEAEs associated with mesalamine treatment.
While topical pharmacotherapies, including mesalamine suppositories, can reduce disease activity in patients with UP [3], the way in which these agents are administered can compromise patients’ compliance and increase the overall costs of treatment (secondary to the costs of treating disease relapse and progression). In one multicenter study, 72 patients with UP who experienced ≥2 relapses within the past year or had achieved remission within the previous 3 months were given oral 5-ASA daily and either a 5-ASA enema or a placebo enema twice weekly for 1 year [36]. At the end of the study, patients treated with oral and rectal 5-ASA experienced significantly fewer relapses than did the placebo-treated controls (P = 0.036). Given the reduced overall need for medication to manage disease relapse, pharmacoeconomic analysis of the data showed a favorable cost-effectiveness ratio for the combination of oral and rectal 5-ASA [36]. Data from a similar study in 42 patients with UC who were treated with either oral 5-ASA and 5-ASA enemas or oral 5-ASA alone twice weekly for a median of 6 years showed a significant reduction in the number and incidence of relapses in the patients who received the combined oral and rectal 5-ASA treatment regimen (~40%; P < 0.034) [37]. Although administration drug costs were higher for rectal than for oral 5-ASA, the overall cost of relapse and hospitalization expenses decreased substantially (~50%) in the population studied [37]. Further, the pharmacologic treatment of patients with UP is associated with lower rates of morbidity and mortality than are the various surgical procedures currently being investigated [38].
The high rate of compliance reported by both mesalamine suppository treatment groups (>95%) in this study compares favorably with compliance levels reported in other studies [10, 13], and shows that patients are willing to self-administer suppositories to manage their UP. However, recent compliance data have shown that reducing the frequency of administration (i.e., from BID to QHS) significantly improves adherence to treatment [28]. The difficulty in retaining morning suppositories reported in a previous study [10] was overcome with QHS dosing.
A strength of this study was the use of the DAI, which has been validated in other clinical trials. The 6-week treatment duration of this study afforded an opportunity to extend the efficacy and safety assessment of mesalamine and provide some insight into the number of suppositories a patient may be willing to self-administer in a day. Limitations of the study include the relatively small sample size, the open-label design, the potentially compromised calculation of compliance via suppository count, the lack of a placebo run-in phase and/or a control group, and an accurate evaluation of the onset of response or the time to maximal response.
In conclusion, the results from this study confirm the efficacy and safety of mesalamine suppositories when administered at 500 mg BID or 1 g QHS for the treatment of patients with active mild-to-moderate UP. Most patients reported onset of response within 3 weeks and UP remission and reduced disease extension after 6 weeks of therapy, indicating that a 6-week treatment period should be recommended. The validity of a more convenient timing of suppository administration (QHS rather than BID) was also confirmed, and this once-daily dosing should increase compliance to mesalamine therapy and further improve clinical outcomes for patients with UP. Future studies are needed to quantify the benefits of extending treatment with mesalamine beyond 6 weeks and to examine remission in treatment-naïve, newly diagnosed patients with UP.
References
Regueiro MD. Diagnosis and treatment of ulcerative proctitis. J Clin Gastroenterol. 2004;38:733–740. doi:10.1097/01.mcg.0000139178.33502.a3.
Hanauer SB. Update on medical management of inflammatory bowel disease: ulcerative colitis. Rev Gastroenterol Disord. 2001;1:169–176.
Kornbluth A, Sachar DB. Ulcerative colitis practice guidelines in adults: American college of gastroenterology, practice parameters committee. Am J Gastroenterol. 2010;105:501–523. doi:10.1038/ajg.2009.727.
Herrinton LJ, Liu L, Lewis JD, Griffin PM, Allison J. Incidence and prevalence of inflammatory bowel disease in a Northern California managed care organization, 1996–2002. Am J Gastroenterol. 2008;103:1998–2006.
Ng SC, Kamm MA. Therapeutic strategies for the management of ulcerative colitis. Inflamm Bowel Dis. 2009;15:935–950. doi:10.1002/ibd.20797.
James SL, Irving PM, Gearry RB, Gibson PR. Management of distal ulcerative colitis: frequently asked questions analysis. Intern Med J. 2008;38:114–119. doi:10.1111/j.1445-5994.2007.01601.x.
Lakatos PL, Lakatos L. Ulcerative proctitis: a review of pharmacotherapy and management. Expert Opin Pharmacother. 2008;9:741–749. doi:10.1517/14656566.9.5.741.
Marteau P, Probert CS, Lindgren S, et al. Combined oral and enema treatment with Pentasa® (mesalazine) is superior to oral therapy alone in patients with extensive mild/moderate active ulcerative colitis: a randomised, double blind, placebo controlled study. Gut. 2005;54:960–965. doi:10.1136/gut.2004.060103.
Campieri M, Gionchetti P, Belluzzi A, et al. Topical treatment with 5-aminosalicylic in distal ulcerative colitis by using a new suppository preparation: a double-blind placebo controlled trial. Int J Colorectal Dis. 1990;5:79–81. doi:10.1007/BF00298473.
Gionchetti P, Rizzello F, Venturi A, et al. Comparison of mesalazine suppositories in proctitis and distal proctosigmoiditis. Aliment Pharmacol Ther. 1997;11:1053–1057. doi:10.1046/j.1365-2036.1997.00259.x.
Lawrance IC, Copeland TS. Rectal tacrolimus in the treatment of resistant ulcerative proctitis. Aliment Pharmacol Ther. 2008;28:1214–1220. doi:10.1111/j.1365-2036.2008.03841.x.
Lucidarme D, Marteau P, Foucault M, Vautrin B, Filoche B. Efficacy and tolerance of mesalazine suppositories versus hydrocortisone foam in proctitis. Aliment Pharmacol Ther. 1997;11:335–340. doi:10.1046/j.1365-2036.1997.126297000.x.
Marteau P, Florent C. Comparative, open, randomized trial of the efficacy and tolerance of slow-release 5-ASA suppositories once daily versus conventional 5-ASA suppositories twice daily in the treatment of active cryptogenic proctitis: French Pentasa Study Group. Am J Gastroenterol. 2000;95:166–170. doi:10.1111/j.1572-0241.2000.01679.x.
Marshall JK, Irvine EJ. Putting rectal 5-aminosalicylic acid in its place: the role in distal ulcerative colitis. Am J Gastroenterol. 2000;95:1628–1636.
van Hogezand RA, van Hees PA, van Gorp JP, et al. Double-blind comparison of 5-aminosalicylic acid and acetyl-5-aminosalicylic acid suppositories in patients with idiopathic proctitis. Aliment Pharmacol Ther. 1988;2:33–40.
Rubenstein JH, Waljee AK, Jeter JM, Velayos FS, Ladabaum U, Higgins PD. Cost effectiveness of ulcerative colitis surveillance in the setting of 5-aminosalicylates. Am J Gastroenterol. 2009;104:2222–2232. doi:10.1038/ajg.2009.264.
Kaiser GC, Yan F, Polk DB. Mesalamine blocks tumor necrosis factor growth inhibition and nuclear factor κB activation in mouse colonocytes. Gastroenterology. 1999;116:602–609. doi:10.1016/S0016-5085(99)70182-4.
Narisawa T, Fukaura Y. Prevention by intrarectal 5-aminosalicylic acid of N-methylnitrosourea-induced colon cancer in F344 rats. Dis Colon Rectum. 2003;46:900–903. doi:10.1007/s10350-004-6681-3.
Stolfi C, Sarra M, Caruso R, et al. Inhibition of colon carcinogenesis by 2-methoxy-5-amino-N-hydroxybenzamide, a novel derivative of mesalamine. Gastroenterology. 2010;138:221–230. doi:10.1053/j.gastro.2009.08.062.
Lamet M, Ptak T, Dallaire C, et al.; Mesalamine Study Group. Efficacy and safety of mesalamine 1 g HS versus 500 mg BID suppositories in mild to moderate ulcerative proctitis: a multicenter randomized study. Inflamm Bowel Dis. 2005;11:625–630. doi:10.1097/01.MIB.0000171277.70404.40.
Jørgensen LG, Fredholm L, Hyltoft Petersen P, Hey H, Munkholm P, Brandslund I. How accurate are clinical activity indices for scoring of disease activity in inflammatory bowel disease (IBD)? Clin Chem Lab Med. 2005;43:403–411. doi:10.1515/CCLM.2005.073.
Sutherland LR, Martin F, Greer S, et al. 5-Aminosalicylic acid enema in the treatment of distal ulcerative colitis, proctosigmoiditis, and proctitis. Gastroenterology. 1987;92:1894–1898.
Geboes K, Ridell R, Ost A, Jensfelt B, Persson T, Lofberg R. A reproducible grading scale for histological assessment of inflammation in ulcerative colitis. Gut. 2000;47:404–409. doi:10.1136/gut.47.3.404.
Riddell RH, Goldman H, Ransohoff DF, et al. Dysplasia in inflammatory bowel disease: standardized classification with provisional clinical applications. Hum Pathol. 1983;14:931–968. doi:10.1016/S0046-8177(83)80175-0.
Schlemper RJ, Riddell RH, Kato Y, et al. The Vienna classification of gastrointestinal epithelial neoplasia. Gut. 2000;47:251–255. doi:10.1136/gut.47.2.251.
D’Agostino RB Sr, Massaro JM, Sullivan LM. Non-inferiority trials: design concepts and issues—the encounters of academic consultants in statistics. Stat Med. 2003;22:169–186. doi:10.1002/sim.1425.
Regueiro M, Loftus EV Jr, Steinhart AH, Cohen RD. Inflammatory Bowel Disease Center. Clinical guidelines for the medical management of left-sided ulcerative colitis and ulcerative proctitis: summary statement. Inflamm Bowel Dis. 2006;12:972–978. doi:10.1097/01.mib.0000231496.92013.85.
Higgins PD, Rubin DT, Kaulback K, Schoenfield PS, Kane SV. Systematic review: impact of non-adherence to 5-aminosalicylic acid products on the frequency and cost of ulcerative colitis flares. Aliment Pharmacol Ther. 2009;29:247–257. doi:10.1111/j.1365-2036.2008.03865.x.
Cortot A, Maetz D, Degoutte E, et al. Mesalamine foam enema versus mesalamine liquid enema in active left-sided ulcerative colitis. Am J Gastroenterol. 2008;103:3106–3114. doi:10.1111/j.1572-0241.2008.02152.x.
Molnár T, Farkas K, Nagy F, Németh I, Wittmann T. Topically administered infliximab can work in ulcerative proctitis despite the ineffectiveness of intravenous induction therapy. Am J Gastroenterol. 2009;104:1857–1858.
Regueiro M, Loftus EV Jr, Steinhart AH, Cohen RD. Medical management of left-sided ulcerative colitis and ulcerative proctitis: critical evaluation of therapeutic trials. Inflamm Bowel Dis. 2006;12:979–994. doi:10.1097/01.mib.0000231495.92013.5e.
d’Albasio G, Paoluzi P, Campieri M, et al. Maintenance treatment of ulcerative proctitis with mesalazine suppositories: a double-blind placebo-controlled trial. Am J Gastroenterol. 1998;93:799–803.
Tokui K, Asai Y, Arakawa T, Matsumoto T, Nabeshima T. Comparative absorption of 5-aminosalicylic acid (5-ASA) after administration of a 5-ASA enema and salazosulfapyridine (SASP) after an SASP suppository in Japanese volunteers. Biol Pharm Bull. 2002;25:264–267. doi:10.1248/bpb.25.264.
Vree TB, Dammers E, Exler PS, Maes RA. Mono- and biphasic plasma concentration-time curves of mesalazine from a 500 mg suppository in healthy male volunteers controlled by the time of defecation before dosing. J Pharm Pharmacol. 2000;52:645–652. doi:10.1211/0022357001774471.
Vree TB, Dammers E, Exler PS, Maes RA. Liver and gut mucosa acetylation of mesalazine in healthy volunteers. Int J Clin Pharmacol Ther. 2000;38:514–522.
D’Albasio G, Pacini F, Camarri E, et al. Combined therapy with 5-aminosalicylic acid tablets and enemas for maintaining remission in ulcerative colitis: a randomized double-blind study. Am J Gastroenterol. 1997;92:1143–1147.
Piodi LP, Ulivieri FM, Cermesoni L, Cesana BM. Long-term intermittent treatment with low-dose 5-aminosalicylic enemas is efficacious for remission maintenance in ulcerative colitis. Scand J Gastroenterol. 2004;39:154–157. doi:10.1080/00365520310008133.
Bolin TD, Wong S, Crouch R, Engelman JL, Riordan SM. Appendicectomy as a therapy for ulcerative proctitis. Am J Gastroenterol. 2009;104:2476–2482. doi:10.1038/ajg.2009.388.
Acknowledgments
The authors wish to thank Jonathan M. Wert, MD, for editorial assistance in the development of this manuscript, which was supported by Axcan Pharma Inc.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Additional information
This study was conducted on behalf of the Mesalamine Study Group.
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Lamet, M. A Multicenter, Randomized Study to Evaluate the Efficacy and Safety of Mesalamine Suppositories 1 g at Bedtime and 500 mg Twice Daily in Patients with Active Mild-to-Moderate Ulcerative Proctitis. Dig Dis Sci 56, 513–522 (2011). https://doi.org/10.1007/s10620-010-1334-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-010-1334-y