
Abstract
Clinical trials have shown that adjuvant Zoledronic acid (ZOL) reduces the development of bone metastases irrespective of ER status. However, post-menopausal patients show anti-tumour benefit with ZOL whereas pre-menopausal patients do not. Here we have developed in vivo models of spontaneous ER+ve breast cancer metastasis to bone and investigated the effects of ZOL and oestrogen on tumour cell dissemination and growth. ER+ve (MCF7, T47D) or ER−ve (MDA-MB-231) cells were administered by inter-mammary or inter-cardiac injection into female nude mice ± estradiol. Mice were administered saline or 100 μg/kg ZOL weekly. Tumour growth, dissemination of tumour cells in blood, bone and bone turnover were monitored by luciferase imaging, histology, flow cytometry, two-photon microscopy, micro-CT and TRAP/P1NP ELISA. Estradiol induced metastasis of ER+ve cells to bone in 80–100 % of animals whereas bone metastases from ER−ve cells were unaffected. Administration of ZOL had no effect on tumour growth in the fat pad but significantly inhibited dissemination of ER+ve tumour cells to bone and frequency of bone metastasis. Estradiol and ZOL increased bone volume via different mechanisms: Estradiol increased activity of bone forming osteoblasts whereas administration of ZOL to estradiol supplemented mice decreased osteoclast activity and returned osteoblast activity to levels comparable to that of saline treated mice. ER−ve cells require increased osteoclast activity to grow in bone whereas ER+ve cells do not. Zol does not affect ER+ve tumour growth in soft tissue, however, inhibition of bone turnover by ZOL reduced dissemination and growth of ER+ve breast cancer cells in bone.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Oestrogen receptor positive breast cancer accounts for approximately 70 % of primary breast malignancies. The development of targeted hormonal and biological therapies have resulted in significant increases in survival, however progression to metastasis remains a substantial clinical problem. Around 65–70 % of cancers that metastasise to bone are ER+ve and this condition remains incurable [1]. Due to the lack of clinically relevant models for ER+ve breast cancer bone metastasis the vast majority of pre-clinical studies have used hormone receptor negative cell lines to investigate breast cancer dissemination and growth in bone [reviewed in 2 and 3]. We have established in vivo models of spontaneous bone metastasis from ER+ve MCF7 and T47D cells grown in mouse mammary fat pads. These new models have enabled us, for the first time, to investigate some of the fundamental steps of bone metastasis following inoculation of cell lines into hind mammary fat pads, including growth at the primary site, tumour cell dissemination into the circulation and colonisation and growth in the bone microenvironment. We are now using these models to investigate the effects of bone targeted therapies on spontaneous bone metastasis of ER+ve xenografts.
There is increasing clinical and pre-clinical evidence supporting anti-tumour effects of the anti-resorptive agent zoledronic acid (ZOL) in hormone receptor negative breast cancer, but the effects on ER+ve breast cancers remain to be elucidated. Recent clinical trials suggest that menopausal status, rather than the hormone receptor status of the tumour, determines the anti-cancer efficiency of ZOL. The AZURE (Does Adjuvant zoledronic acid reduce Recurrence in stage II/III breast cancer?) trial [4] study investigated the use of adjuvant ZOL alongside chemotherapy in women with high risk of breast cancer recurrence. 3360 women were randomised to receive either placebo or intensive treatment with ZOL, in addition to standard therapy. Approximately 78 % of patients in each group had ER+ve tumours [5] and there was no correlation between hormone receptor status, disease free survival (DFS) or risk of death (ROD). In contrast, women who were postmenopausal for at least 5-years before entering the trial had a significantly increased disease free survival (25 %) and reduced risk of death from any cause (26 %) [6]. These data were confirmed in the ABCSG-12 trial that showed increased DFS in women more than age 40 who received ZOL. However the ABCSC-12 study also presented evidence indicating that adjuvant use of ZOL improves the outcome of pre-menopausal patients with ER+ve tumours [7], although patients in this trial received goserelin, a superantagonist of oestrogen, whereas participants in the AZURE study did not.
The differences in anti-tumour effects of ZOL between pre-menopausal and post-menopausal patients with bone metastasis are likely to be influenced by the regulation of bone turnover by oestrogens. Oestrogen has profound effects on bone by inhibiting osteoclastogenesis and promoting osteoclast apoptosis via direct actions on osteoclasts and their precursors [8–13]. In addition, oestrogens act on cells of the osteoblast lineage to prevent production of osteoclastigenic cytokines as well as inhibiting osteoclast apoptosis [10–13]. ZOL also exerts pro-apoptotic effects on osteoclasts through inhibition of key enzymes in the mevalonate pathway, ultimately preventing the release of bone derived factors that may stimulate tumour growth [14]. In contrast to oestrogen, administration of ZOL also reduces the number and activity of bone forming osteoblasts [15]. It is therefore possible that ZOL may be a more effective anti-tumour agent in a low oestrogen bone microenvironment due to its ability to inhibit the increased activity of osteoclasts observed under these conditions.
We have recently used a mouse model that mimics the pre- and post-menopausal bone microenvironment to establish the effects of anti-resorptive agents on ER−ve MDA-MB-231 breast tumour growth in bone. In this model, reduced circulating oestrogen caused by ovariectomy resulted in increased osteoclastic bone resorption that triggered the growth of dormant disseminated tumour cells to form overt tumours in bone. Administration of ZOL, or the specific osteoclast inhibitor OPG-Fc, prevented ovariectomy-induced stimulation of ER−ve tumour growth in bone, providing evidence that this process is driven by osteoclast mediated mechanisms [16, 17]. Interestingly, injection of ER+ve MCF7 cells into mice with high osteoclast activity did not induce tumour growth in bone [16]. We do not know if absence of tumour growth under these conditions was due to ER+ve tumour cells requiring oestrogen for growth and/or if different mechanisms are responsible for ER+ve and ER−ve breast cancer growth in bone.
In the current study we have investigated the effects of high levels of oestrogen on ER+ve tumour growth and spontaneous metastasis to bone, as well as on the ability of ER+ and ER−ve breast cancer cells to form tumours in bone. We have carried out detailed analysis of bone and tumour growth following administration of ZOL to mice supplemented with estradiol compared to control, to investigate the anti-tumour effects of ZOL in a high oestrogen environment. As expected, ER+ve breast cancer cells required addition of oestrogen to grow and metastasise to bone. Importantly, this study provides the first evidence that growth of ER+ve and ER−ve breast cancer cells in bone is stimulated by different mechanisms: ER+ve cells require active bone turnover but do not need increased osteoclasts activity, whereas ER−ve cells require stimulation of osteoclastic resorption of bone to grow in this environment. Furthermore, inhibition of bone turnover by ZOL reduced spontaneous metastasis of ER+ve breast cancer cells from the mammary fat pad to bone as well as dissemination and growth of ER+ve tumour cells in bone.
Materials and methods
Cell culture
Human breast cancer cells, MDA-MB-231-luc2 tdTomato (Calliper Life Sciences, Cheshire, UK), MCF7 and T47D (European Collection of Cell Cultures, Wiltshire, UK) were stably transfected with luc-2 using lentiviral transfection systems (Promega, Life sciences). Prior to in vivo inoculation cells were incubated for 15 min with 25 µM of 1,1′-Dioctadecyl-′,3′-Tetramethylindodicarbocyanine, 4-Chlorobenzenesulfonate (DiD) (Life Technologies, Paisley, UK). Tumour growth was monitored using an IVIS (luminol) system (Calliper Life Sciences). Human osteoblast-like HS5 cells were obtained from European Collection of Cell Cultures. All cell types were maintained in DMSO supplemented with 10 % FCS (Gibco, Paisley, UK).
Analysis of pro-metastatic parameters in vitro
All experiments were carried out in triplicate and repeated three times. Preliminary experiments were carried out to find optimum serum concentrations for obtaining cell growth at conditions 50 % of their maximum rate and this dose was used for cell proliferation experiments. Effects of PBS (control), 25, 50 or 100 μM ZOL on proliferation of HS5, MCF7 and T47D cells was performed in DMSO supplemented with 5 % FCS monitored every 24 h for 96 h by cell counting with a 1/400 mm2 haemocytometer (Hawksley, UK). Migration and invasion of MCF7 and T47D cells treated with ZOL/or towards HS5 cells treated with ZOL, PBS or 10 μg/ml mitomycin C (control) was assessed using 6 mm Transwell® plates with an 8.0 μm pore size (Costar, Corning Incorporated, USA) uncoated or coated with matrigel (Invitrogen). MCF7 or T47D cells were seeded into the inner chamber at a density of 5 × 105 per assay in DMSO supplemented with 2.5 % FCS and HS5 cells in DMSO supplemented with 2.5 % FCS treated with 15 μM ZOL, PBS or 10 μg/ml mitomycin C (control) added to the outer chamber. 24 after seeding cells were removed from the top surface of the membrane and cells that had invaded through the pores were stained with Haematoxylin and Eosin. Invasion was calculated as the percentage of cells that invaded through matrigel compared with cells that moved to the underside of uncoated plates Numbers of cells were counted using a DMRB microscope (Leitz, Germany) and OsteoMeasure XP v1.2.0.1 program (Osteometrics, USA).
In vivo studies
We used 12-week-old female BALB/c nude mice (Charles River, Kent, UK). Experiments were carried out in accordance with local guidelines and with Home Office approval under project licence 40/3462, University of Sheffield, UK.
For experiments investigating the effects of estradiol on ER+ve tumour growth and bone metastasis 17β estradiol pellets (Innovative Research of America) were implanted sub-cutaneously into 6 mice and 6 mice were sham operated (control). 3 days later, 5 × 105 MCF7 or T47D cells in 20 μL (50 % matrigel (BD Biosciences) 50 % PBS) were injected into the left and right hind fat pads. This experiment was repeated twice to ensure reproducibility of our model.
To investigate the effects of ZOL on primary tumour growth and bone metastasis, 5 × 105 T47D cells or MDA-MB-231 cells were injected into the left and right hind mammary fat pads 3 days after implantation of an estradiol pellet. 100 μg/kg ZOL [(1-hydroxy-2- (1H-imidazol-1-yl) ethylene) bisphosphonic acid] (Novartis Pharma AG, Basel, Switzerland) or PBS control was administered via intra-peritoneal injection (n = 8 mice/group). Primary tumour growth was measured twice per week using callipers (tumour volume = 4/3 πr3, where radius was calculated as (tumour length + width)/4), bone metastases were monitored by in vivo luciferase imaging and final tumour volume was measured on 2 non-serial histological samples taken from the right tibiae using a Leica RMRB upright microscope and OsteoMeasure software (Osteometrics, Inc. Dacatur, GA. USA.). 15 additional mice were used to study the effects of estradiol and ZOL on bone turnover. Estradiol pellets were implanted subcutaneously into 10 mice and 5 were non-estradiol control. 3-days after implantation of the pellet, 5 mice were injected once per week with 100 μg/kg ZOL the other 5 received PBS control for 4-weeks. Mice were sacrificed 24 h after their final injection with ZOL/PBS.
For investigating the effects of estradiol on dissemination and growth of ER−ve tumour cells in bone, 17β estradiol pellets were implanted sub-cutaneously into 8 mice and 8 mice were sham operated (control). 3 days following implantation of estradiol pellet/sham operation 5 × 105 MDA-MB-231 cells were injected into the left cardiac ventricle and bone metastases were monitored twice per week by luciferase imaging. Animals were sacrificed 4 weeks following injection of tumour cells.
All mice were culled by cardiac exsanguination and cervical dislocation. Whole blood was stored in heparin/10 % DMSO at −80 °C for subsequent analysis of circulating tumour cells. Serum was stored at −80 °C, primary tumours were fixed in 4 % paraformaldehyde and tibiae and femurs were fixed in 4 % PFA for μCT analysis before decalcification in 1 % PFA/0.5 % EDTA and processing for histology. Bones for two-photon analysis were stored in OCT at −80 °C.
Biochemical analysis
Serum concentrations of TRAP 5b and P1NP were measured using commercially available ELISA kits: MouseTRAP™ Assay (Immunodiagnostic systems) and Rat/Mouse P1NP competitive immunoassay kit (Immunodiagnostic Systems), respectively.
Microcomputed tomography imaging
Microcomputed tomography analysis was carried out using a Skyscan 1172 X-ray-computed microtomography scanner (Skyscan, Aartselar, Belgium) equipped with an X-ray tube (voltage, 49 kV; current, 200 μA) and a 0.5-mm aluminium filter. Pixel size was set to 5.86 μm and scanning initiated from the top of the proximal tibia as previously described [11].
Bone histology
Osteoclasts were detected by toluidine blue and tartrate-resistant acid phosphatase (TRAP) staining as previously described [12]. Osteoblasts were identified as mononuclear, cuboidal cells residing in chains along the bone surface. The number of osteoclasts/osteoblasts per millimetre of cortical-endosteal bone surface and trabecular bone surfaces and the proportion of bone surface occupied by osteoclasts/osteoblasts was determined using a Leica RMRB upright microscope and OsteoMeasure software (Osteometrics inc.) as previously described [16].
Two-photon microscopy
Tibiae were imaged using a multiphoton confocal microscope (LSM510 NLO upright; Zeiss, Cambridge, UK). DiD labelled cells were visualised using a 900 nm Chameleon laser, bone was detected using the 633 nm multiphoton laser (Coherent, Santa Clara, CA.) and images were reconstructed in LSM software version 4.2 (Zeiss). Velocity 3D image analysis software (Zeiss) was used to count the number of disseminated tumour cells in 2104 μm (X-axis) × 2525 μm (Y-axis) × 100 μm (Z-axis) of the left proximal tibia just below the growth plate.
Isolation of circulating tumour cells
Whole blood was analysed from each of the 8 mice per treatment group and parental MCF7 cells were used for staining controls using the protocol described in Holen et al. [18], with the exception that the primary antibody used was anti-human EpCAM antibody directly conjugated to Phycoerythrin (PE) (Clone 1B7; 1:50; eBioscience, Hatfield, UK). PE positive cells were plated directly into a 96-well tissue culture plate on a MoFlow High performance cell sorter (Beckman Coulter, Cambridge, UK). PE fluorescence was detected by a 555LP dichroic long pass and a 580/30 nm band pass filter. Acquisition and analysis of cells was performed using Summit 4.3 software. Following sorting, cells were cultured in RPMI medium supplemented with 10 % FCS.
Statistical analysis
Linear regression was calculated for ‘slope significance to non zero’ using R2 and Syx tests. For Kaplan–Meier survival charts, statistical analysis was by one tailed Mantel–Haenszel test and log rank test for trend. All other statistical analysis was by one way analysis of variance (ANOVA) followed by Newman-Keuls multiple comparison test. Data for in vivo experiments are shown as mean ± SD and for in vitro experiments as mean ± SEM. Statistical significance was defined as P ≤ 0.05 as calculated using Graphpad PRISM software. All P values are two-sided.
Results
ER+ve breast cancer cells metastasise to bone from the mammary fat pads
We first established two models of ER+ve breast cancer metastasis to bone by implanting MCF7 or T47D cells into the two hind mammary fat pads of 12-week old BALB/c nude mice (Fig. 1). In the absence of estradiol supplementation, tumours grew very slowly reaching only 126.00 ± 29.46 mm3 (MCF7) and 135.33 ± 25.50 mm3 (T47D) by day 56. Implantation of an estradiol pellet 3 days before injection of tumour cells resulted in significantly increased tumour growth from both cell lines, with tumour volumes reaching 194.00 ± 17.34 mm3 for MCF7 + estradiol compared with 61.66 ± 20.21 mm3 for MCF7 control at 42 days, and 196.67 ± 30.61 mm3 for T47D + estradiol compared with 101.33 ± 20.74 mm3 for T47D control at 49 days. All animals supplemented with estradiol were sacrificed before the pre-planned protocol end point (day 56) due to rapid loss of ≥10 % body mass (Fig. 1a, b). Luciferase imaging and histological analysis showed that neither MCF7 nor T47D cells metastasised to the long bones in the absence of estradiol supplementation. In marked contrast, in the presence of estradiol, bone metastases were detected in 85 % of mice bearing MCF7 tumours and 65 % of mice bearing T47D tumours (Fig. 1c). MCF7 and T47D cells specifically metastasised to the tibiae and femurs and no overt metastasis were detected elsewhere.

Estradiol stimulates ER+ve tumour growth in the mammary fat pad and bone metastasis in vivo. 12-week old female BALB/c nude mice (n = 6 per group) were injected with 5 × 105 MCF7 or T47D cells into the left and right hind mammary fat pads. Panels a, b show line graphs representing mean ± SD primary tumour growth (upper panel) and time to morbidity following tumour cell injection is represented by Kaplan Mayer plots (lower panel) for MCF7 and T47D cells, respectively. Panel c shows the percentage of mice that developed spontaneous bone metastases, photographic images and photomicrographs of Goldners’ stained cross sections of tibiae from representative mice with (T) and without (N) bone metastasis from the second experiment 42 days after injection of tumour cells into the hind mammary fat pads. *P < 0.05 compared with control
Estradiol does not stimulate growth of ER−ve breast cancer cells in bone
We have previously demonstrated that estradiol supplementation of BALB/c nude mice leads to significant increases in bone forming osteoblasts and bone volume, but does not affect numbers or activity of osteoclasts in tibiae or femurs, compared with control mice [16]. In these studies we established that increased bone turnover stimulates growth of ER−ve MDA-MB-231 breast cancer cells in bone through osteoclast-mediated mechanisms [16, 17]. We have now investigated whether stimulation of bone metastases from ER−ve MDA-MB-231 cells is specifically driven by osteoclast activity, or if increased activity of osteoblasts following estradiol changes to the bone microenvironment can also stimulate bone metastasis. Increasing osteoblast activity with estradiol has no effect on MDA-MB-231 tumour growth following orthotropic implantation into mammary fat pads [19]. Furthermore, inhibiting bone turnover with weekly administration of 100 μg/kg zoledronic acid (ZOL, Fig. 2a) did not alter MDA-MB-231 tumour growth in this site (Fig. 2b). MDA-MB-231 cells did not spontaneously metastasise from the mammary fat pads to bones in this model and therefore investigations into the effects of estradiol and ZOL on MDA-MB-231 tumour cell dissemination and bone metastases were carried out following tumour cell inoculation via intra-cardiac injection. Injection of MDA-MB-231 cells into the left cardiac ventricle 3-days following implantation of an estradiol pellet (Fig. 2a) had no effect on tumour growth in bone (Fig. 2c, d). Tumours grew in the bones of 3/8 control mice and 2/8 mice given estradiol supplementation (Fig. 2c). Two-photon analysis of the tibiae from these animals showed similar numbers of DiD-positive, non-proliferating, tumour cells in the marrow cavity of all mice (Fig. 2e). These data imply that oestrogen induced stimulation of osteoblast does not increase growth of ER−ve breast cancer cells in bone.

Estradiol ± zoledronic acid do not effect MDA-MB-231 tumour growth and bone metastases. 12-week old female BALB/c nude mice ± estradiol received weekly injection with 100 μg/kg zoledronic acid or saline (control) for 28 days. 3 days after commencement of estradiol or zoledronic acid/saline, 5 × 105 MDA-MB-231 cells were injected into the left cardiac ventricle or into the left and right hind mammary fat pads; n = 8 mice per group (panel a). Panel b shows the effects of zoledronic acid on growth of MDA-MB-231 cells in the mammary fat pads as tumour volume (mm3) ± SD. Panel c shows percentage of mice with tumours growing in their bones as measured on histological sections c and d shows luciferase images 28 days following intracardiac injection of ER−ve MDA-MB-231 cells. DiD labelled tumour cells in bone and representative multiphoton images of non-proliferating tumour cells (shown in red) disseminated in bone (shown in white) are shown in panel (e)
ZOL inhibits metastasis of T47D cells to bone from tumours in the mammary fat pad
Injection of T47D cells into the hind mammary fat pads of BALB/c nude mice reproducibly resulted in bone metastases and these mice remained healthier and lived longer than animals injected with MCF7 cells. We therefore used the T47D model to investigate the effects of ZOL on primary tumour growth and bone metastasis (Fig. 3a). Weekly administration of 100 μg/kg ZOL starting 3 days after injection of T47D cells into the two hind fat pads had no effect on primary tumour growth by day 34 (tumour volume 155.92 ± 142.86 mm3 in control versus 131.37 ± 117.32 mm3 in ZOL treated mice, Fig. 3b, c). Analysis of the hind limbs revealed that animals treated with ZOL had significantly reduced bone metastases compared with control (Fig. 3b, d, e). Bioluminescence and histological analysis showed that tumours were present in the hind limbs of 8/8 saline treated (control) mice and 2/8 mice treated weekly with 100 μg/kg ZOL (Fig. 3b, d), with a mean tumour bioluminescence per leg of 1.35 ± 0.54 p/s in control mice and 0.28 ± 0.44 p/s in ZOL treated mice (P < 0.001) (Fig. 3e). Histological analysis confirmed reduced tumour load in bones of mice treated with ZOL compared with control mice, with average tumour area measuring 2.50 ± 1.02 in control mice and 0.25 ± 0.35 in ZOL treated mice (P < 0.001) (Fig. 3f). There was no correlation between the volume of tumours in mammary fat pads and bone metastases (Fig. 3g). These data show that administration of ZOL decreased numbers of mice that develop bone metastases and reduced the size of these tumours in bone compared to control. This reduction in bone metastasis was not the result of ZOL affecting primary tumour volume.

Zoledronic acid inhibits bone metastasis from T47D cells. Estradiol pellets were implanted subcutaneously into 12-week old female BALB/c nude mice after 3 days 5 × 105 T47D cells were injected into the left and right mammary fat pads (i.m), mice were left for 3-days before receiving weekly administration of 100 μg/kg zoledronic acid or saline (control) for 28 days; n-8 mice per group (panel a). H&E stained scanned images of T47D tumours extracted from the right hind fat pad of mice treated weekly with saline or 100 μg/kg zoledronic acid and luciferase images for the right tibiae and femurs from the same animals are shown in panel (b). Panel c shows the mean tumour volume ± SD in the hind mammary fat pads and panel d shows the percentage of mice that developed bone metastases. Panels e and f show the mean tumour area per leg ± SD as identified by bioluminescence (photons per second) and following measurement on histological sections respectively. Panel g shows the correlation between mean size of tumour in the two mammary fat pads and mean size of bone metastases from the same animal *P < 0.05 compared with control
Effects of ZOL on ER+ve circulating and disseminated tumour cells
As ZOL reduced numbers of detectable bone metastases from T47D tumours, we investigated whether this effect was associated with alterations in numbers of tumour cells that were available to generate metastasis. Flow cytometric analysis of EpCAM positive cells isolated from whole blood of mice bearing T47D mammary tumours showed a trend towards fewer circulating tumour cells in ZOL treated mice (13.00 ± 6.66 per ml/mouse) compared with control (73.67 ± 40.42 per ml/mouse, P = 0.056) (Fig. 4a). We next used two-photon microscopy to detect DiD-labelled tumour cells that had and disseminated to bone from the mammary pad (Fig. 4b). We detected significantly higher numbers of DiD-labelled tumour cells in the marrow cavity of tibiae from control (saline) treated mice (4.64 ± 0.15 cells/mm2) compared with mice treated weekly with 100 μg/kg ZOL (3.87 ± 0.08 cells/mm2 P = 0.02). These data imply that ZOL may affect tumour cell shedding from the primary site, thereby limiting the number of tumour cells that are available to colonise bone and develop into secondary tumours.

Zoledronic acid inhibits dissemination of ER+ve tumour cells in bone. Estradiol pellets were implanted subcutaneously into 12-week old female BALB/c nude mice after 3 days 5 × 105 T47D cells were injected into the left and right mammary fat pads (i.m), mice were left for 3-days before receiving weekly administration of 100 μg/kg zoledronic acid or saline (control) for 28 days. N = 8 mice per group were analysed for tumour cell dissemination into blood and n = 4 mice per group were used for two-photon analysis of tumour cell dissemination into the tibiae. Panel a shows the effects of weekly administration of zoledronic acid on dissemination of T47D cells form mammary fat pad tumours into the blood. Flow cytometric histograms show the positive staining profiles and gating strategy. Mean numbers of circulating tumour cells ± SD were calculated from numbers of cells observed in R3. Panel b shows representative multiphoton images of non-proliferating DiD-labelled tumour cells (shown in red) that have been disseminated into the bone (shown in white) form the circulation. Mean numbers ± SD of DiD labelled tumour cells in the tibiae are shown in the histogram. *P < 0.05 compared with control
Effects of estradiol and ZOL on bone
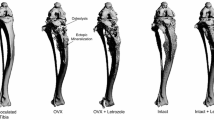
Estradiol and ZOL both have extensive effects on the bone environment. Estradiol appears to increase bone volume via inducing osteoclast apoptosis and prolonging the life of osteoblasts [8, 9], whereas ZOL has well documented properties as an anti-resorptive agent targeting osteoclasts [14]. In order to identify the effects of ZOL on bone turnover in a high oestrogen environment, we gave 12-week old female mice continuous estradiol supplementation with or without weekly administration of 100 μg/kg ZOL for 28-days. uCT analysis of tibiae revealed a significant increase in bone volume in mice receiving estradiol compared with control animals (BV/TV % = 18.94 ± 0.85 for control and 56.15 ± 5.24 for estradiol, P ≤ 0.001) which was further increased in mice receiving estradiol and ZOL to 78.81 ± 2.31 (P = 0.01 compared to estradiol alone and P ≤ 0.001 compared with control) (Fig. 5a, b). ELISA analysis showed no differences in serum TRAP levels between control (12.36 ± 2.76 U/L) and estradiol (9.96 ± 2.07 U/L) supplemented animals. In contrast, treating estradiol supplemented mice with ZOL resulted in a significant reduction in circulating concentrations of TRAP to 1.44 ± 0.88 U/L (P ≤ 0.001) (Fig. 5c). Supplementation with estradiol also stimulated osteoblast activity as evident by a significant increase in circulating concentrations of P1NP compared with control (P < 0.001). Administration of ZOL to estradiol supplemented mice reduced circulating P1NP concentrations to levels similar to that in control mice (control 2.93 ± 0.29 ng/ml; estradiol 4.25 ± 0.33; estradiol + ZOL 2.72 ± 0.48 ng/ml) (Fig. 5d). These data show that ZOL is more effective at reducing osteoclast activity than osteoblast activity in a high oestrogen environment.

Estradiol and zoledronic acid on bone have physiological effects on bone. Estradiol pellets were implanted into 10, 12-week old female BALB/c nude mice and 5 mice received saline control. 3 days later 5 estradiol-supplemented mice received 100 μg/kg zoledronic acid weekly and the remaining animals were administered saline (control, n = 5 per group). Representative μCT images of tibiae from mice receiving estradiol supplementation with or without weekly administration of 100 μg/kg zoledronic acid (a). Panel b shows effects of estradiol ± zoledronic acid on percentage of bone volume compared with total tissue volume ± SD. Serum concentrations of P1NP and TRAP are show in panels c and d, respectively. ***P < 0.001 compared with control, ^^^P < 0.001 compared with estradiol
Effects of bone cells ± ZOL on migration and invasion of ER+ve breast cancer cells
We next investigated whether cytostatic concentrations of ZOL affect tumour cell invasion and migration towards bone cells in vitro. Initial experiments identified 25 μM ZOL to be cytostatic and non-toxic in HS5 (osteoblastic), MCF7 and T47D cells over a 96 h time period (Fig. 6a, c), without affecting migration or invasion of matrigel by these tumour cells (data not shown). Treatment of HS5 cells with 25 μM ZOL inhibited the numbers of MCF7 and T47D cells that migrated towards these HS5 cells (P = 0.02 for MCF7 and P = 0.03 for T47D cells) and inhibited invasion of MCF7 and T47D cells through matrigel towards HS5 cells (P ≤ 0.01 for both MCF7 and T47D cells) over a 24 h time period (Fig. 6d–g). All data were compared with migration and invasion of MCF7 and T47D cells towards control (PBS) treated HS5 cells. To establish whether reduced migration and invasion was a result of ZOL decreasing the proliferation of HS5 cells we used mitomycin C as a control. Treatment of HS5 cells with mitomycin C had comparable affects on migration and invasion of MCF7 and T47D cells to that caused by treatment with ZOL (Fig. 6d–g). These in vitro data indicate that tumour cells have a preference to migrate towards bone cells that are actively proliferation. Therefore, it is possible that inhibition of bone turnover by ZOL may reduce ER+ve breast cancer cell homing to bone from the primary site in our in vivo models.

Effects of Zoledronic acid on ER+ve breast cancer cell migration and invasion towards bone cells in vitro. Panels a, b and c show the effects of 25, 50 and 100 μM zoledronic acid on proliferation of HS5 (bone) cells and MCF7 and T47D breast cancer cells respectively. Effects of 25 μM ZOL and mitomycin C on HS5 cell induced migration and invasion of MCF7 cells are shown in panels (d, f) and effects on T47D cells are shown in panels (e, g). *P < 0.05 compared with control, $P < 0.05 compared with 100 μM zoledronic acid and ^P < 0.05 compared with 100 and 50 μM zoledronic acid
Discussion
To date, only a small number of studies have been carried out investigating the effects of ZOL on ER+ve breast cancer and parameters associated with metastasis. These have focused on in vitro models of tumour apoptosis [20, 21] proliferation [22, 23], migration [24, 25] and invasion [25, 26] and until now there has been no data available from clinically relevant in vivo models representing metastasis of human breast cancer cells from the primary site to bone. For the current study we have used MCF7 and T47D cells to establish in vivo models of ER+ve breast cancer bone metastasis. Injection of either MCF7 or T47D cells into the two hind mammary fat pads of 12-week old BALB/c nude mice, 3 days after subcutaneous implantation of a slow release estradiol pellet, resulted in spontaneous overt metastasis detected exclusively in long bones of the hind limbs within 2–3 weeks. All animals supplemented with estradiol were sacrificed before control mice and before the pre-planned protocol endpoint due to loss of 10 % of body mass. Although the size primary tumours in estradiol supplemented animals were small (135 ± 25.5 mm3 for T47D and 126 ± 29.46 mm3 for T47D) and did not differ significantly from primary tumours in control mice estradiol supplemented animals had the additional burden of bone metastases. It is likely that this additional tumour burden contributed to accelerated loss of body mass seen in these animals. Mice bearing T47D tumours remained healthier for longer and therefore these models were used for subsequent in vivo experiments. Using these models, we have shown that administration of a clinically relevant dose of ZOL (100 μg/kg, equivalent to the 4 mg clinical dose) once per week reduces the number of tumour cells that disseminate into the bone environment and inhibits development of bone metastases. We did not detect overt metastasis by luciferase imaging in any other bony sites or soft tissue during the 56 day protocol. However, we did not perform two-photon analysis in tissues other than tibiae and femurs and therefore further experiments need to be carried out into accurately characterise the metastatic potential of MCF7 and T47D cells in these models.
Our present data suggest that the direct effects of ZOL on tumour cell proliferation in vitro and in soft tissue tumours in vivo are similar for both ER+ve and hormone receptor negative breast cancer cells. Numerous reports show direct anti-proliferative effects of adding 5–25 μM ZOL to the media of ER+ve MCF7 and T47D cells as well as hormone receptor negative MDA-MB-231 and MDA-MB-436 cells [reviewed in 27, 28]. In the current study we wanted to mimic the effects of ZOL in the bone environment. ZOL has high affinity of calcium in bone where it is preferentially incorporated into sites of active bone remodelling. In breast cancer patients, this results in millimolar concentrations of ZOL accumulating in bone following a single 4 mg infusion [29] and 60–65 % of this is retained by the skeleton [30]. As ZOL is directly incorporated into the skeleton, this compound has long lasting effects in this organ and it is estimated that the concentration of bisphosphonates in the resorption lacuna can be up to 10–1000 μM [31]. We therefore investigated the effects of 25–100 μM ZOL tumour cell proliferation, migration and invasion towards HS5 bone cells. In agreement, our current data show that exposure to 25 μM ZOL inhibits proliferation of MCF7 and T47D cells. There are no published data relating to the direct anti-tumour effects of ZOL on ER+ve soft tissue tumours, however, we and others have consistently shown that administration of clinically relevant doses of ZOL do not exert anti-tumour effects on ER−ve soft tissue tumours in vivo [32–35]. Similarly, the current study demonstrated an absence of anti-tumour activity against ER−ve MDA-MB-231 or ER+ve MCF7 mammary tumours following weekly administration of 100 μg/kg ZOL in vivo. It therefore seems likely that concentrations of ZOL that reach soft tissue tumours in vivo are not sufficient to affect tumour growth and any anti-metastatic effects are unlikely to be as a result of ZOL acting directly on the primary tumour.
ZOL is shown to inhibit migration and invasion of ER−ve breast cancer cells but has comparatively modest inhibitory effects on ER+ve cells in vitro [36–38]. In agreement with this, we found no effects of ZOL on migration or invasion of MCF7 or T47D cells in vitro (data not shown). However, addition of either the cytostatic compound mitomycin C, or 25 μM ZOL, to a transwell assay inhibited HS5 (bone cell) stimulated migration and invasion of MCF7 and T47D cells, suggesting that repressing proliferation of bone cells inhibits metastatic potential of ER+ve breast cancer cells. This hypothesis was supported by our in vivo studies, in which we found a trend towards decreased numbers of tumour cells being disseminated from primary T47D mammary tumours into the blood stream of mice treated with ZOL compared with control (saline) treated mice (P = 0.056). This was accompanied by a significant decrease in the numbers of DiD-labelled tumour cells in the tibiae of mice treated with estradiol and ZOL, compared with mice treated with estradiol alone. We can not decipher whether lower numbers of disseminated DiD-labelled tumour cells in bone are as a result of fewer available cells in the circulation that could colonise this site, or whether ZOL induced alterations to the bone microenvironment make bone less permissive for ER+ve tumour cell homing and/or colonisation. Interestingly, we have recently shown that a single dose of ZOL does cause substantial alterations to the areas of the tibia most commonly colonised by breast cancer cells in BALB/c nude mice [15]. Although this caused a re-distribution of ER−ve cancer cells in bone, the total number of tumour cells was unaffected. However, the model used by Haider et al. relies on tumour cells being injected directly into the circulation and therefore does not represent the effects of ZOL on tumour cell dissemination in bone from a primary site. It must be noted that extrapolation of numbers of tumour cells disseminated in bone by counting DiD labelled cells is likely to be an underestimate. DiD is a lipophilic membrane dye that is retained by non-proliferating cells and lost as tumour cells divide [16]. ZOL significantly inhibited formation of tumours in bone, therefore more tumour cells that have disseminated in bone will retain DID in the ZOL treated group at the 4 week time point measured, compared with control where proliferating tumour cells will gradually lose the dye and become undetectable. Whether tumours develop in bone from one or several disseminated tumour cells remains an unanswered question, making it difficult to judge the extent to which this affects our analysis. It is likely that ZOL induced reduction in numbers of tumour cells that disseminate in bone contribute to the reduced tumour burden observed in ZOL treated animals compared with control, however, this is probably not the only mechanism. We have previously shown that administration of ZOL or OPG-Fc prevents OVX-induced growth of dormant breast cancer cells to form overt tumours in bone, demonstrating that inhibition of activity of bone cells prevents proliferation of disseminated tumour cells in this environment [16, 17]. It is possible that some antitumour effects of ZOL remain unaccounted for in our model. We have used athymic nude mice that lack T-cells to allow the growth and metastasis of human cancer cell lines. There is accumulating evidence suggesting that ZOL has immunomodulatory properties that may contribute to the potential anti tumour effects of this compound [39–41]. Unfortunately, there is no immunocompetent model of ER+ve breast cancer metastasis to bone that will allow us to study this in more detail, further highlighting the need for the development of more clinically relevant in vivo models.
Castration-induced bone loss and PTH induced increase in osteoclasts and osteoblasts stimulate MDA-MB-231 tumour growth in bone [16, 17]. The compensatory mechanisms coupling activity of osteoclasts and osteoblasts makes it difficult to distinguish which cell type is involved in stimulation of tumourigenesis. In order for MCF7 or T47D cells to metastasise to bone it was necessary to increase the concentrations of circulating oestrogen in the mice by implanting a slow release estradiol pellet. Oestrogen has well defined activity in bone causing apoptosis in osteoclasts whilst prolonging the life of osteoblasts [8–13] and analysis of serum and bones from animals given estradiol supplementation revealed substantial increases in osteoblast activity but no significant alterations in osteoclast activity. This is in agreement with our previous data showing increased numbers of osteoblasts and no alterations in numbers of osteoclasts in bones from animals supplemented with estradiol [16]. We therefore investigated whether these oestrogen-mediated alterations in bone turnover were responsible for stimulating tumour growth in bone. Injection of hormone receptor negative MDA-MB-231 cells directly into the circulation of 12-week old mice supplemented with estradiol resulted in tumour cells disseminating in bone, but did not stimulate tumour formation, suggesting that MDA-MB-231 cells require osteoclast mediated bone resorption to proliferate in the bone environment of adult mice. In contrast, ER+ve cells readily form tumours in this estradiol high and osteoblast rich environment, but are not stimulated to proliferate in bone under conditions of increased bone resorption [16]. Administration of ZOL to mice supplemented with estradiol resulted in significant decrease in osteoclast activity and restored osteoblast activity to background (control) levels (Fig. 3c, d). It therefore appears that either ER+ve breast cancer cells require increased osteoblast activity to grow in bone, or they can grow in bone under normal conditions of bone resorption (requiring estradiol as a growth factor independent of the bone environment). Our data suggest that decreased bone turnover following ZOL prevents proliferation of disseminated ER+ve cells in bone, however, the mechanism behind this has yet to be fully established. Further studies are now required to decipher which cell types are important for ER+ve tumour growth in bone and why ZOL appears to have reduced capacity to inhibit osteoblast activity in a high oestrogen environment.
In conclusion, ZOL exerts indirect and direct effects that inhibit spontaneous bone metastasis from ER+ve mammary tumours. Administration of ZOL does not alter growth of ER+ve cells at the primary site but reduces tumour cell dissemination in bone. Once cells have disseminated in the bone environment the ZOL-mediated reduction in bone turnover prevents tumour cells from proliferating and forming overt metastases. The mechanism for stimulating tumour growth in bone appears to be different for hormone receptor negative and ER+ve breast cancer cells; hormone receptor negative cells require increased bone resorption to proliferate and form bone metastases whereas ER+ve cells do not. As both hormone receptor negative and ER+ve breast cancer cells require active bone resorption for tumours to grow in this environment, we hypothesise that ZOL inhibits tumour growth in bone form both types of breast cancer by inhibiting bone turnover. It is therefore likely that ZOL has more potent effects on tumour growth in patients who are 5-years or more post menopause as firstly these patients exhibit higher levels of bone turnover at baseline than pre-menopausal patients and therefore gain more benefit from anti-resorptive therapy [42] and secondly, ZOL appears to have increased ability to reduce bone turnover in a low oestrogen environment.
References
Zhang XH, Giuliano M, Trivedi MV, Schiff R, Osborne CK (2013) Metastasis dormancy in estrogen receptor-positive breast cancer. Clin Cancer Res 19(23):6389–6397
Kretschmann KL, Welm AL (2012) Metastasis dormancy in estrogen receptor-positive breast cancer. Cancer Metastasis Rev 31(3–4):579–583
Brown HK, Holen I (2009) Anti-tumour effects of bisphosphonates–what have we learned from in vivo models? Curr Cancer Drug Targets 9(7):807–823
Coleman R, Cameron D, Dodwell D, Bell R, Wilson C, Rathbone E et al (2014) AZURE investigators. Adjuvant zoledronic acid in patients with early breast cancer: final efficacy analysis of the AZURE (BIG 01/04) randomised open-label phase 3 trial. Lancet Oncol 15(9):997–1006
Coleman RE, Marshall H, Cameron D, Dodwell D, Burkinshaw R, Keane M et al (2011) Breast-cancer adjuvant therapy with zoledronic acid. N Engl J Med 365(15):1396–1405
Coleman R, de Boer R, Eidtmann H, Llombart A, Davidson N, Neven P et al (2013) Zoledronic acid (zoledronate) for postmenopausal women with early breast cancer receiving adjuvant letrozole (ZO-FAST study): final 60-month results. Ann Oncol 24(2):398–405
Gnant M, Mlineritsch B, Schippinger W, Luschin-Ebengreuth G, Pöstlberger S, Menzel C et al (2009) Endocrine therapy plus zoledronic acid in premenopausal breast cancer. N Engl J Med 360(7):679–691
Nakamura T, Imai Y, Matsumoto T, Sato S, Takeuchi K, Igarashi K et al (2007) Estrogen prevents bone loss via estrogen receptor alpha and induction of Fas ligand in osteoclasts. Cell 130(5):811–823
Novack DV (2007) Estrogen and bone: osteoclasts take center stage. Cell Metab 6(4):254–256
Tomkinson A, Reeve J, Shaw RW, Noble BS (1997) The death of osteocytes via apoptosis accompanies estrogen withdrawal in human bone. J Clin Endocrinol Metab 82(9):3128–3135
Kousteni S, Chen JR, Bellido T, Han L, Ali AA, O’Brien CA et al (2007) Reversal of bone loss in mice by nongenotropic signaling of sex steroids. Cell Metab 6(4):254–256
Kousteni S, Bellido T, Plotkin LI, O’Brien CA, Bodenner DL, Han L, Han K et al (2001) Nongenotropic, sex-nonspecific signaling through the estrogen or androgen receptors: dissociation from transcriptional activity. Cell 104(5):719–730
Almeida M, Han L, Martin-Millan M, Plotkin LI, Stewart SA, Roberson PK et al (2007) Skeletal involution by age-associated oxidative stress and its acceleration by loss of sex steroids. J Biol Chem 282(37):27285–27297
Benford HL, McGowan NW, Helfrich MH, Nuttall ME, Rogers MJ (2001) Visualization of bisphosphonate-induced caspase-3 activity in apoptotic osteoclasts in vitro. Bone 28(5):465–473
Haider MT, Holen I, Dear TN, Hunter K, Brown HK (2014) Modifying the osteoblastic niche with zoledronic acid in vivo-potential implications for breast cancer bone metastasis. Bone 66:240–250
Ottewell PD, Wang N, Brown HK, Reeves KJ, Fowles CA, Croucher PI et al (2014) Zoledronic acid has differential antitumor activity in the pre- and postmenopausal bone microenvironment in vivo. Clin Cancer Res 20(11):2922–2932
Ottewell PD, Wang N, Brown HK, Fowles CA, Croucher PI, Eaton CL, Holen I (2015) OPG-Fc inhibits ovariectomy-induced growth of disseminated breast cancer cells in bone. Int J Cancer. (Epub ahead of print)
Holen I, Whitworth J, Nutter F, Evans A, Brown HK, Lefley DV et al (2012) Loss of plakoglobin promotes decreased cell-cell contact, increased invasion, and breast cancer cell dissemination in vivo. Breast Cancer Res 14(3):R86
Fleming JM, Miller TC, Meyer MJ, Ginsburg E, Vonderhaar BK (2010) Local regulation of human breast xenograft models. J Cell Physiol 224(3):795–806
Senaratne SG, Pirianov G, Mansi JL, Arnett TR, Colston KW (2000) Bisphosphonates induce apoptosis in human breast cancer cell lines. Br J Cancer 82(8):1459–1468
Fromigue O, Lagneaux L, Body JJ (2000) Bisphosphonates induce breast cancer cell death in vitro. J Bone Miner Res 15(11):2211–2221
Mönkkönen H, Kuokkanen J, Holen I, Evans A, Lefley DV, Jauhiainen M et al (2008) Bisphosphonate-induced ATP analog formation and its effect on inhibition of cancer cell growth. Anticancer Drugs 19(4):391–399
Ibrahim T, Mercatali L, Sacanna E, Tesei A, Carloni S, Ulivi P et al (2012) Inhibition of breast cancer cell proliferation in repeated and non-repeated treatment with zoledronic acid. Cancer Cell Int 12(1):48
Muinelo-Romay L, Garcia D, Alonso-Alconada L, Vieito M, Carmona M, Martínez N et al (2013) Zoledronic acid as an antimetastatic agent for different human tumor cell lines. Anticancer Res 33(12):5295–5300
Insalaco L, Di Gaudio F, Terrasi M, Amodeo V, Caruso S, Corsini LR et al (2012) Analysis of molecular mechanisms and anti-tumoural effects of zoledronic acid in breast cancer cells. J Cell Mol Med 16(9):2186–2195
Rietkötter E, Menck K, Bleckmann A, Farhat K, Schaffrinski M, Schulz M et al (2013) Zoledronic acid inhibits macrophage/microglia-assisted breast cancer cell invasion. Oncotarget 4(9):1449–1460
Bosch-Barrera J, Merajver SD, Menéndez JA, Van Poznak C (2011) Direct antitumour activity of zoledronic acid: preclinical and clinical data. Clin Transl Oncol 13(3):148–155
Green JR, Guenther A (2011) The backbone of progress–preclinical studies and innovations with zoledronic acid. Crit Rev Oncol Hematol 77(Suppl 1):S3–S12
Steinman RA, Brufsky AM, Oesterreich S (2012) Zoledronic acid effectiveness against breast cancer metastases - a role for estrogen in the microenvironment? Breast Cancer Res 14(5):213
Chen T, Berenson J, Vescio R, Swift R, Gilchick A, Goodin S (2002) Pharmacokinetics and pharmacodynamics of zoledronic acid in cancer patients with bone metastases. J Clin Pharmacol 42(11):1228–1236
Rogers MJ, Watts DJ, Russell RGG (1997) Overview of bisphosphonates. Cancer 80(8):1652–1660
Daubiné F, Le Gall C, Gasser J, Green J, Clézardin P (2007) Antitumor effects of clinical dosing regimens of bisphosphonates in experimental breast cancer bone metastasis. J Natl Cancer Inst 99(4):322–330
Ottewell PD, Deux B, Mönkkönen H, Cross S, Coleman RE, Clezardin P, Holen I (2008) Differential effect of doxorubicin and zoledronic acid on intraosseous versus extraosseous breast tumor growth in vivo. Clin Cancer Res 14(14):4658–4666
Ottewell PD, Mönkkönen H, Jones M, Lefley DV, Coleman RE, Holen I (2008) Antitumor effects of doxorubicin followed by zoledronic acid in a mouse model of breast cancer. J Natl Cancer Inst 100(16):1167–1178
Ottewell PD, Lefley DV, Cross SS, Evans CA, Coleman RE, Holen I (2010) Sustained inhibition of tumor growth and prolonged survival following sequential administration of doxorubicin and zoledronic acid in a breast cancer model. Int J Cancer 126(2):522–532
Ottewell PD, Brown HK, Jones M, Rogers TL, Cross SS, Brown NJ et al (2012) Combination therapy inhibits development and progression of mammary tumours in immunocompetent mice. Breast Cancer Res Treat 133(2):523–536
Boissier S, Ferreras M, Peyruchaud O, Magnetto S, Ebetino FH, Colombel M et al (2000) Bisphosphonates inhibit breast and prostate carcinoma cell invasion, an early event in the formation of bone metastases. Cancer Res 60(11):2949–2954
Dedes PG, Gialeli Ch, Tsonis AI, Kanakis I, Theocharis AD, Kletsas D et al (2012) Expression of matrix macromolecules and functional properties of breast cancer cells are modulated by the bisphosphonate zoledronic acid. Biochim Biophys Acta 20(12):1926–1939
Miyagawa F, Tanaka Y, Yamashita S, Minato N (2001) Essential requirement of antigen presentation by monocyte lineage cells for the activation of primary human gamma delta T cells by aminobisphosphonate antigen. J Immunol 166:5508–5514
Dieli F, Gebbia N, Poccia F, Caccamo N, Montesano C, Fulfaro F et al (2003) Induction of gammadelta T-lymphocyte effector functions by bisphosphonate zoledronic acid in cancer patients in vivo. Blood 102:2310–2311
Gober HJ, Kistowska M, Angman L, Jeno P, Mori L, De Libero G (2003) Human T cell receptor gammadelta cells recognize endogenous mevalonate metabolites in tumor cells. J Exp Med 197:163–168
Khosla S (2010) Update on estrogens and the skeleton. J Clin Endocrinol Metab 95(8):3569–3577
Acknowledgments
The IVIS Lumina II system was purchased by an equipment grant from Yorkshire Cancer Research. Laboratory consumables were paid from by grants from Cancer Research UK and Weston Park Hospital Cancer Charity, UK.
Authors contributions
IH- study design and manuscript editing, MW– in vitro data acquisition and analysis and in vivo data analysis, FN- ER+ve in vivo data acquisition and analysis, AF- ER−ve in vivo data acquisition and analysis, AE- in vitro data acquisition and analysis, CE– study design and manuscript editing and PO- conceived the study, data analysis and manuscript preparation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Authors have no competing interests to declare.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Holen, I., Walker, M., Nutter, F. et al. Oestrogen receptor positive breast cancer metastasis to bone: inhibition by targeting the bone microenvironment in vivo. Clin Exp Metastasis 33, 211–224 (2016). https://doi.org/10.1007/s10585-015-9770-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10585-015-9770-x