
Abstract
Purpose
Compare medical expenditures among adults with statin-associated adverse effects (SAAE) and high statin adherence (HSA) following myocardial infarction (MI).
Methods
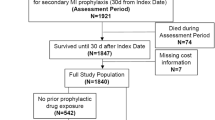
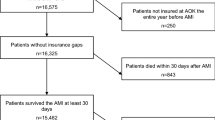
We analyzed expenditures in 2016 US dollars among Medicare beneficiaries with SAAE (n = 1741) and HSA (n = 55,567) who were ≥ 66 years of age and initiated moderate/high-intensity statins following an MI in 2007–2013. SAAE were identified through a claims-based algorithm, which included down-titrating statins and initiating ezetimibe, switching to ezetimibe monotherapy, having a rhabdomyolysis or antihyperlipidemic adverse event followed by statin down-titration or discontinuation, or switching between ≥ 3 statin types within 365 days following MI. HSA was defined by having a statin available to take for ≥ 80% of the days in the 365 days following MI.
Results
Expenditures among beneficiaries with SAAE and HSA were $40,776 (95% CI $38,329–$43,223) and $26,728 ($26,482–$26,974), respectively, in the 365 days following MI, and $34,238 ($31,396–$37,080) and $29,053 ($28,605–$29,500), respectively, for every year after the first 365 days. Multivariable-adjusted ratios comparing expenditures among beneficiaries with SAAE versus HSA in the first 365 days and after the first 365 days following MI were 1.51 (95% CI 1.43–1.59) and 1.23 (1.12–1.34), respectively. Inpatient and outpatient expenditures were higher among beneficiaries with SAAE versus HSA during and after the first 365 days following MI. Compared to beneficiaries with HSA, medication expenditures among those with SAAE were similar in the 365 days following MI, but higher afterwards. Other medical expenditures were higher among beneficiaries with SAAE versus HSA.
Conclusion
SAAE are associated with increased expenditures following MI compared with HSA.




Similar content being viewed by others

References
Stone NJ, Robinson JG, Lichtenstein AH, Bairey Merz CN, Blum CB, Eckel RH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129:S1–45.
Baigent C, Keech A, Kearney PM, et al. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet. 2005;366:1267–78.
Zhang H, Plutzky J, Skentzos S, Morrison F, Mar P, Shubina M, et al. Discontinuation of statins in routine care settings: a cohort study. Ann Intern Med. 2013;158:526–34.
Bruckert E, Hayem G, Dejager S, Yau C, Begaud B. Mild to moderate muscular symptoms with high-dosage statin therapy in hyperlipidemic patients--the PRIMO study. Cardiovasc Drugs Ther. 2005;19:403–14.
Wei MY, Ito MK, Cohen JD, Brinton EA, Jacobson TA. Predictors of statin adherence, switching, and discontinuation in the USAGE survey: understanding the use of statins in America and gaps in patient education. J Clin Lipidol. 2013;7:472–83.
Serban MC, Colantonio LD, Manthripragada AD, Monda KL, Bittner VA, Banach M, et al. Statin intolerance and risk of coronary heart events and all-cause mortality following myocardial infarction. J Am Coll Cardiol. 2017;69:1386–95.
Bitton A, Choudhry NK, Matlin OS, Swanton K, Shrank WH. The impact of medication adherence on coronary artery disease costs and outcomes: a systematic review. Am J Med. 2013;126:357 e7–357 e27.
Aubert RE, Yao J, Xia F, Garavaglia SB. Is there a relationship between early statin compliance and a reduction in healthcare utilization? Am J Manag Care. 2010;16:459–66.
Pittman DG, Chen W, Bowlin SJ, Foody JM. Adherence to statins, subsequent healthcare costs, and cardiovascular hospitalizations. Am J Cardiol. 2011;107:1662–6.
De Vera MA, Bhole V, Burns LC, Lacaille D. Impact of statin adherence on cardiovascular disease and mortality outcomes: a systematic review. Br J Clin Pharmacol. 2014;78:684–98.
Penning-van Beest FJ, Termorshuizen F, Goettsch WG, Klungel OH, Kastelein JJ, Herings RM. Adherence to evidence-based statin guidelines reduces the risk of hospitalizations for acute myocardial infarction by 40%: a cohort study. Eur Heart J. 2007;28:154–9.
Colantonio LD, Levitan EB, Yun H, Kilgore ML, Rhodes JD, Howard G, et al. Use of Medicare claims data for the identification of myocardial infarction: the Reasons for Geographic And Racial Differences in Stroke (REGARDS) study. Med Care. 2018;56:1051–9.
Colantonio LD, Kent ST, Huang L, Chen L, Monda KL, Serban MC, et al. Algorithms to identify statin intolerance in Medicare administrative claim data. Cardiovasc Drugs Ther. 2016;30:525–33.
Arca M, Pigna G. Treating statin-intolerant patients. Diabetes Metab Syndr Obes. 2011;4:155–66.
Rosenson RS, Baker SK, Jacobson TA, Kopecky SL, Parker BA, The National Lipid Association’s Muscle Safety Expert P. An assessment by the Statin Muscle Safety Task Force: 2014 update. J Clin Lipidol. 2014;8:S58–71.
Rosenson RS, Baker S, Banach M, Borow KM, Braun LT, Bruckert E, et al. Optimizing cholesterol treatment in patients with muscle complaints. J Am Coll Cardiol. 2017;70:1290–301.
Choudhry NK, Shrank WH, Levin RL, et al. Measuring concurrent adherence to multiple related medications. Am J Manag Care. 2009;15:457–64.
Karve S, Cleves MA, Helm M, Hudson TJ, West DS, Martin BC. Good and poor adherence: optimal cut-point for adherence measures using administrative claims data. Curr Med Res Opin. 2009;25:2303–10.
Smolina K, Wright FL, Rayner M, Goldacre MJ. Long-term survival and recurrence after acute myocardial infarction in England, 2004 to 2010. Circ Cardiovasc Qual Outcomes. 2012;5:532–40.
Mozaffarian D, Benjamin EJ, Go AS, et al. Heart Disease and Stroke Statistics-2016 update: a report from the American Heart Association. Circulation. 2016;133:e38–e360.
Romano PS, Roos LL, Jollis JG. Adapting a clinical comorbidity index for use with ICD-9-CM administrative data: differing perspectives. J Clin Epidemiol. 1993;46:1075–9 discussion 1081-90.
Muntner P, Yun H, Sharma P, Delzell E, Kent ST, Kilgore ML, et al. Ability of low antihypertensive medication adherence to predict statin discontinuation and low statin adherence in patients initiating treatment after a coronary event. Am J Cardiol. 2014;114:826–31.
Aaron KJ, Colantonio LD, Deng L, Judd SE, Locher JL, Safford MM, et al. Cardiovascular health and healthcare utilization and expenditures among Medicare beneficiaries: the REasons for Geographic And Racial Differences in Stroke (REGARDS) Study. J Am Heart Assoc. 2017;6:e005106.
Evans MA, Golomb BA. Statin-associated adverse cognitive effects: survey results from 171 patients. Pharmacotherapy. 2009;29:800–11.
Parker BA, Capizzi JA, Grimaldi AS, Clarkson PM, Cole SM, Keadle J, et al. Effect of statins on skeletal muscle function. Circulation. 2013;127:96–103.
Graham JH, Sanchez RJ, Saseen JJ, Mallya UG, Panaccio MP, Evans MA. Clinical and economic consequences of statin intolerance in the United States: results from an integrated health system. J Clin Lipidol. 2017;11:70–79 e1.
Harris LJ, Thapa R, Brown M, Pabbathi S, Childress RD, Heimberg M, et al. Clinical and laboratory phenotype of patients experiencing statin intolerance attributable to myalgia. J Clin Lipidol. 2011;5:299–307.
Keating AJ, Campbell KB, Guyton JR. Intermittent nondaily dosing strategies in patients with previous statin-induced myopathy. Ann Pharmacother. 2013;47:398–404.
Mampuya WM, Frid D, Rocco M, Huang J, Brennan DM, Hazen SL, et al. Treatment strategies in patients with statin intolerance: the Cleveland Clinic experience. Am Heart J. 2013;166:597–603.
Awad K, Mikhailidis DP, Toth PP, et al. Efficacy and safety of alternate-day versus daily dosing of statins: a systematic review and meta-analysis. Cardiovasc Drugs Ther. 2017;31:419–31.
Guyton JR, Bays HE, Grundy SM, Jacobson TA, The National Lipid Association Statin Intolerance Panel. An assessment by the Statin Intolerance Panel: 2014 update. J Clin Lipidol. 2014;8:S72–81.
Jacobson TA, Maki KC, Orringer CE, Jones PH, Kris-Etherton P, Sikand G, et al. National Lipid Association Recommendations for patient-centered management of dyslipidemia: part 2. J Clin Lipidol. 2015;9:S1–122 e1.
Lloyd-Jones DM, Morris PB, Ballantyne CM, et al. 2017 focused update of the 2016 ACC expert consensus decision pathway on the role of non-statin therapies for LDL-cholesterol lowering in the management of atherosclerotic cardiovascular disease risk: a report of the American College of Cardiology Task Force on expert consensus decision pathways. J Am Coll Cardiol. 2017;70:1785–822.
Ara R, Pandor A, Tumur I, Paisley S, Duenas A, Williams R, et al. Cost effectiveness of ezetimibe in patients with cardiovascular disease and statin intolerance or contraindications: a Markov model. Am J Cardiovasc Drugs. 2008;8:419–27.
Sabatine MS, Giugliano RP, Keech AC, Honarpour N, Wiviott SD, Murphy SA, et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med. 2017;376:1713–22.
Administration on Aging, Administration for Community Living, U.S. Department of Health and Human Services. A profile of older Americans: 2016. Washington, DC: U.S. Dept. of Health and Human Services, Administration on Aging; 2016. [Cited: October 10, 2017]; Available from: https://www.acl.gov/sites/default/files/Aging%20and%20Disability%20in%20America/2016-Profile.pdf
The Henry J. Kaiser Family Foundation. An overview of Medicare. Issue brief. Menlo Park: The Henry J. Kaiser Family Foundation, 2017. [Cited: August 4, 2018]; Available from: http://files.kff.org/attachment/issue-brief-an-overview-of-medicare
Colantonio LD, Kent ST, Kilgore ML, Delzell E, Curtis JR, Howard G, et al. Agreement between Medicare pharmacy claims, self-report, and medication inventory for assessing lipid-lowering medication use. Pharmacoepidemiol Drug Saf. 2016;25:827–35.
Funding
The design and conduct of the study, interpretation of the results, and preparation of the manuscript were supported through a research grant from Amgen, Inc. (Thousand Oaks, CA).
Author information
Authors and Affiliations
Contributions
The academic authors conducted all analyses, drafted the manuscript, and maintained the rights to publish this article.
Corresponding author
Ethics declarations
Conflict of Interest
KLM, DJH, and JFM are employed by and stockholders of Amgen. PM receives research support from Amgen. MEF and MLK receive research support from Amgen. RSR receives research support from Akcea, Amgen, AstraZeneca, Medicines Company, and Regeneron; is an Advisory Board member/consultant for C5, CVS Caremark, Regeneron, and Sanofi; receives honoraria from Akcea, Amgen, Kowa, and Pfizer; is a stockholder of MediMergent; and receives royalties from UpToDate. LDC, LD, and LC have no conflict of interest.
Ethical Approval
All procedures performed in the current student were conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The Institutional Review Board at the University of Alabama at Birmingham and Centers for Medicare and Medicaid Services approved the study.
Informed Consent
This is a retrospective cohort study and formal consent was not required.
Electronic Supplementary Material
ESM 1
(DOCX 83 kb)
Rights and permissions
About this article

Cite this article
Colantonio, L.D., Deng, L., Chen, L. et al. Medical Expenditures Among Medicare Beneficiaries with Statin-Associated Adverse Effects Following Myocardial Infarction. Cardiovasc Drugs Ther 32, 601–610 (2018). https://doi.org/10.1007/s10557-018-6840-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10557-018-6840-8