
Abstract
Background
Failure to reach 80% of maximal predicted heart rate (HR) during exercise may render a myocardial perfusion single photon emission computed tomography (SPECT) study non-diagnostic for ischemia detection. We sought to investigate the injection of atropine in patients who fail to achieve 80% of age-predicted HR during exercise performed for myocardial perfusion SPECT (MPS), defining its safety and efficacy to raise HR to adequate levels as well as its effect on MPS interpretation.
Methods and results
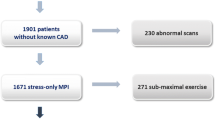
Between January 2002 and December 2004, we studied 3,150 consecutive patients (2,253 men and 897 women, mean age 55 ± 6 years) who were referred to a single office-based nuclear cardiology laboratory for MPS using SPECT imaging. One milligram of atropine was administered to patients that were unable to continue because of fatigue before reaching minimal HR, without an ischemic response (group A, n = 397). The scintigraphic results for group A were compared with those of patients who spontaneously achieved target HR (group B, n = 2,753). In group A, mean HR before atropine injection was 119.5 ± 13.6 beats per minute (bpm), and it increased up to 137.3 ± 13.5 bpm after drug administration, with an incremental of 17.8 ± 6.9 bpm (P < 0.0001). The mean percentage of age-related HR achieved in this group was 83.5 ± 8.1%. In 302 of this patients (76.1%) more than 80% of their aged-related HR (86.9 ± 5.1%) was attained. No major adverse effects occurred. When groups A and B were compared, baseline and peak HR, rate pressure product, and maximal metabolic equivalents achieved were higher in group B. There were no significant differences in the percentage of total positive perfusion studies between both groups: 210/397 patients (52.9%) in group A and 1,342/2,753 patients (48.7%) in group B (P = 0.39). Ischemia or ischemia plus scar was found in 112/397 patients (28.2%) in group A and in 923/2,753 patients (33.5%) of group B (P = 0.14).
Conclusion
Atropine added to exercise stress testing in patients who cannot achieve their 80% age-related HR is a safe, well-tolerated, and feasible method for MPS.
Similar content being viewed by others

References
Fletcher GF, Balady G, Froelicher VF, Hartley L, Haskell WL, Pollok ML (1995) Exercise standards. A statement for healthcare professionals from the American Heart Association. Circulation 91:580–615
Primeau M, Taillefer R, Essiambre R, Lambert R, Honos G (1991) Technetium 99 m Sestamibi myocardial perfusion imaging: comparison between treadmill, dipyridamole and trans-oesophageal atrial pacing “stress” tests in normal subjects. Eur J Nucl Med 18:247–251
Brown KA, Rowen M (1993) Impact of antianginal medications, peak heart rate and stress level on the prognostic value of a normal exercise myocardial perfusion imaging study. J Nucl Med 34:1467–1471
Verzijlbergen JF, Vermeersch PHMJ, Laarman G, Ascoop CAPL (1991) Inadequate exercise leads to suboptimal imaging. Thallium-201 myocardial perfusion imaging after dipyridamole combined with low-level exercise unmasks ischemia in symptomatic patients with non diagnostic thallium-201 scan who exercise submaximally. J Nucl Med 32:2071–2078
McLaughlin PR, Martin RP, Doherty P, et al (1977) Reproducibility of thallium-201 myocardial imaging. Circulation 55:497–503
Heller GV, Ahmed I, Tilkemeier PL, Barbour MM, Garber CE (1992) Influence of exercise intensity on the presence, distribution and size of thallium-201 defects. Am Heart J 123:909–916
Gibbons RJ, Balady GJ, Beasley JW, et al (1997) ACC/AHA guidelines for exercise testing. J Am Coll Cardiol 30:260–311
Iskandrian AS, Heo J, Kong B, Lyons E (1989) The effect of exercise level on the ability of thallium-201 tomographic imaging in detecting coronary artery disease: analysis of 461 patients. J Am Coll Cardiol 14:1477–1486
Gauri AJ, Raxwal VK, Roux L, et al (2001) Effects of chronotropic incompetence and beta-blocker use on the exercise treadmill test in men. Am Heart J 142:136–141
White MP (1999) Pharmacologic stress testing: understanding the options. J Nucl Cardiol 6:672–675
Roche F, Pichot V, Da Costa A, et al (2001) Chronotropic incompetence response to exercise in congestive heart failure, relationship with the cardiac autonomic status. Clin Physiol 21:335–342
Lauer MS, Okin PM, Larson MG, Evans JC, Levy D (1996) Impaired heart rate response to graded exercise: prognostic implications of chronotropic incompetence in the Framingham Heart Study. Circulation 93:1520–1526
Ellestad MH (1996) Chronotropic incompetence. The implications of heart rate response to exercise (compensatory parasympathetic hyperactivity?). Circulation 93:1485–1487
Sarullo FM, Schicchi R, Schirò M, Shillaci AM, Ascione A, Bonnì G, Americo L, Orlando G, Andolina S, Adamo M, Castello A (1996) Comparative evaluation of dobutamine–atropine stress echocardiography with exercise testing for detection of coronary artery disease [in Italian]. G Ital Cardiol 26:1279–1290
McNeill AJ, Fioretti PM, el-Said SM, et al (1992) Enhanced sensitivity for detection of coronary artery disease by addition of atropine to dobutamine stress echocardiography. Am J Cardiol 70:41–46
Secknus MA, Marwick TH (1997) Evolution of dobutamine echocardiography protocols and indications: safety and side effects in 3011 studies over 5 years. J Am Coll Cardiol 29:1234–1240
Geleijnse ML, Elhendy A, van Domburg RT, et al (1997) Cardiac imaging for risk stratification with dobutamine–atropine stress testing in patients with chest pain: echocardiography, perfusion scintigraphy, or both?. Circulation 96:137–147
Elhendy A, Valkema R, van Domburg RT, et al (1998) Safety of dobutamine–atropine stress myocardial perfusion scintigraphy. J Nucl Med 39:1662–1666
Elhendy A, van Domburg RT, Bax JJ, et al (1999) The functional significance of chronotropic incompetence during dobutamine stress test. Heart 81:398–403
Geleijnse ML, Elhendy A, Fioretti PM, Roelandt JRTC (2000) Dobutamine stress myocardial perfusion imaging. J Am Coll Cardiol 36:2017–2027
Elhendy A, van Domburg RT, Bax JJ, et al (2000) Safety, hemodynamic profile, and feasibility of dobutamine stress technetium myocardial perfusion single-photon emission CT imaging for evaluation of coronary artery disease in the elderly. Chest 117:649–656
Elhendy A, Geleijnse ML, van Domburg RT, et al (1997) Comparison of dobutamine stress echocardiography and technetium-99 m sestamibi single-photon emission tomography for the diagnosis of coronary artery disease in hypertensive patients with and without left ventricular hypertrophy. Eur J Nucl Med 25:69–78
Sarullo FM, Azzarello V, Sarullo A, Cirino G, Di Pasquale P (2002) Relationship between exercise-induced ST segmental depression and myocardial ischemia assessed by technetium-99 m tetrofosmin SPECT imaging in patients with inferior Q wave myocardial infarction. Int J Cardiovasc Imaging 18(3):195–201
Candell-Riera J, Santana-Boado C, Castell-Conesa J, et al (1997) Simultaneous dipyridamole/maximal subjective exercise with 99Tc-MIBI SPECT: improved diagnostic yield in coronary artery disease. J Am Coll Cardiol 29:531–536
Cosin-Sales J, Maceira AM, Garcia-Velloso MJ, Macìas A, Gimenez M, Garcìa-Bolao I, Coma-Canella I (2002) Safety and feasibility of atropine added to submaximal exercise stress testing with Tl-201 SPECT for the diagnosis of myocardial ischemia. J Nucl Cardiol 9:581–586
Ellestad MH, Wan MK (1975) Predictive implications of stress testing: follow-up of 2700 subjects after maximum treadmill stress testing. Circulation 51:363–369
Myers J, Prakash M, Froelicher V, Do D, Partington S, Atwood JE (2002) Exercise capacity and mortality among men referred for exercise testing. N Engl J Med 3546:793–801
Ledenheim ML, Pollock BH, Rozanshi A, et al (1986) Extent and severity of myocardial hypoperfusion as predictors of prognosis in patients with suspected coronary artery disease. J Am Coll Cardiol 7:464–471
Hachamovitch R, Berman DS, Kiat H, et al (1996) Exercise myocardial perfusion SPECT in patients without known coronary artery disease .Incremental prognostic value and use in risk stratification. Circulation 93:905–914
Schinkel AF, Elhendy A, van Domburg RT (2002) Prognostic value of dobutamine–atropine stress (99 m)Tc-tetrofosmin myocardial perfusion SPECT in patients with known or suspected coronary artery disease. J Nucl Med 43:767–772
Caner B, Karanfil A, Uysal U (1997) Effect of an additional atropine injection during dobutamine infusion for myocardial SPECT. Nucl Med Commun 18:567–573
David D, Lang RM, Borow KM (1988) Clinical utility of exercise, pacing, and pharmacologic stress testing for the noninvasive determination of myocardial contractility and reserve. Am Heart J 116:235–247
Katzung BG (2001) Basic and clinical pharmacology. McGraw-Hill, New York, p. 115
De Lorenzo A, Foerster J, Sciammarella MG, Suey C, Hayes SW, Friedman JD, Berman DS (2003) Use of atropine in patients with submaximal heart rate during exercise myocardial perfusion SPECT. J Nucl Cardiol 10:51–55
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sarullo, F.M., Ventimiglia, C., Taormina, A. et al. Safety and feasibility of atropine added in patients with sub-maximal heart rate during exercise myocardial perfusion SPECT. Int J Cardiovasc Imaging 23, 511–518 (2007). https://doi.org/10.1007/s10554-006-9169-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10554-006-9169-5