
Abstract
Characteristic cardiac valve abnormalities and left ventricular hypertrophy are present in untreated patients with mucopolysaccharidosis type VI (MPS VI). Cardiac ultrasound was performed to investigate these findings in subjects during long-term enzyme replacement therapy (ERT) with recombinant human arylsulfatase B (rhASB, rhN-acetylgalactosamine 4-sulfatase, galsulfase, Naglazyme®). Studies were conducted in 54 subjects before ERT was begun and at specific intervals for up to 96 weeks of weekly infusions of rhASB at 1 mg/kg during phase 1/2, phase 2, and phase 3 trials of rhASB. At baseline, mitral and aortic valve obstruction was present and was significantly greater in those ≥12 years of age. Mild mitral and trace aortic regurgitation were present, the former being significantly greater in those <12 years. Left ventricular hypertrophy, with averaged z-scores ranging from 1.6–1.9 SD greater than normal, was present for ages both <12 and ≥12 years. After 96 weeks of ERT, ventricular septal hypertrophy regressed in those <12 years. For those ≥12 years, septal hypertrophy was unchanged, and aortic regurgitation increased statistically but not physiologically. Obstructive gradients across mitral and aortic valves remained unchanged. The results suggest that long-term ERT is effective in reducing intraventricular septal hypertrophy and preventing progression of cardiac valve abnormalities when administered to those <12 years of age.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Mucopolysaccharidosis type VI (MPS VI, Maroteaux-Lamy syndrome) is a lysosomal storage disease caused by functional absence of the enzyme N-acetylgalactosamine 4-sulfatase (arylsulfatase B or ASB; E.C. 3.1.6.12). Absence of this enzyme results in the accumulation of dermatan-sulfated glycosaminoglycans (GAGs) within lysosomes of various tissues including bones, cartilage, lungs, airways, and the cardiovascular system (Neufeld and Muenzer 2001). The progressive accumulation of these substances results in multi-organ system dysfunction such as joint contractures, short stature, dysostosis multiplex, decreased pulmonary function, cardiac abnormalities and, ultimately, shortened life span (Neufeld and Muenzer 2001). The severity of the clinical findings is variable but, in a recent survey of 121 MPS VI subjects, an accelerated clinical course was associated with urinary excretion of GAGs in excess of 200 μg/mg creatinine (Swiedler et al. 2005).
Evaluation of the heart in individuals with untreated MPS VI by cardiac ultrasound has been reported by several investigators (Lael et al. 2010; Dangel 1998; Wippermann et al. 1995; Azevedo et al. 2004; Scarpa et al. 2009; Fesslova et al. 2009). The characteristic cardiac abnormalities of MPS VI include ventricular hypertrophy and a progressive thickening of mitral and aortic valves resulting in valvular regurgitation, stenosis, or both. Until now the effects of enzyme replacement therapy (ERT) upon the heart in MPS VI have not been reported.
Previous phase 1, 2, and 3 studies have shown that treatment of individuals with MPS VI by ERT with recombinant human N-acetylgalactosamine 4-sulfatase (rhASB; galsulfase; Naglazyme®) is safe, rapidly reduces urinary GAG levels, and improves endurance as measured by 6- or 12-min walk and pulmonary function testing (Harmatz et al. 2004, 2005, 2006). Further analysis of pooled data from the clinical ERT trials and the survey study has demonstrated safety and significant long-term increases in endurance, pulmonary function, and growth when galsulfase is administered for 96 weeks or more (Harmatz et al. 2008, 2010; Decker et al. 2010). The purpose of this report is to analyze cardiac ultrasound data obtained during phase 1, 2, and 3 clinical ERT trials to determine the effects of 96 weeks of ERT upon the characteristic cardiac findings in individuals with MPS VI.
Methods
Previous reports have detailed the study design and outcomes of the phase I/2, 2, and 3 galsulfase trials in subjects with MPS VI (Harmatz et al. 2004, 2005, 2006, 2008, 2010); details of the clinical trials are outlined in Table 1. Cardiac ultrasound was performed as part of the clinical evaluation of subjects in the phase 1/2, 2, and 3 clinical trials at baseline, before ERT was begun, and at intervals of 24–48 weeks and 72–96 weeks after initiation of ERT (Table 2). An Institutional Review Board (IRB) or Ethics Committee (EC) at each participating clinical site approved each study. All adult patients and parent/guardians gave written consent; patients younger than 18 years old gave written assent according to local IRB regulations.
Archived ultrasound data, collected from subjects who had participated in phase 1/2, 2, or 3 clinical trials, were reviewed and tabulated for this study. The original echoes were obtained and analyzed at the individual sites; original echo tapes were unavailable for further review. Each archived measurement was reviewed for reliability by a single person (E.B.). Discrepancies were resolved by discussion with individual sites. The entire data set was then subjected to statistical evaluation. Height, weight, and urinary GAG content at study entry were analyzed for the 54 subjects who participated in phase 1/2, 2, or 3 galsulfase trials.
Cardiac ultrasound investigations were performed and interpreted by study protocol at the participating sites during each study point as indicated in Table 2. Measurements included M-mode determination of left ventricular chamber dimension in diastole (LVED) and systole (LVES), as well as diastolic left ventricular posterior wall (LVPWd) and intraventricular septal (IVSd) thicknesses. Body surface areas were calculated by the method of duBois for each subject, and z-scores were determined from the measured value for each chamber dimension and wall thickness at each evaluation (Dyar 2012). The individual z-scores from each subject for each parameter at each time point were summed and averaged to obtain the mean z-score displayed in the tables. By use of the z-score, chamber dimensions and wall thicknesses from subjects of differing body surface areas can be compared, and the changes within a particular subject tracked over time (Kampmann et al. 2000). With this system, a z-score of 0 represents the expected normal value for a given body surface area, a positive z-score is a standard deviation value greater than expected normal, and a negative z-score is a value less than expected normal. Left ventricular shortening fraction (SF) was calculated by standard methods (Lopez et al. 2010).
Doppler interrogation of flow acceleration across, and regurgitation from, all cardiac valves was measured by pulsed, continuous, and color flow Doppler methods. Peak systolic gradient was recorded across aortic valves; mean diastolic gradient was measured across mitral valves; and both were compared to normal values (Lopez et al. 2010; Hatle and Angelsen 1985; Baumgartner et al. 2009; Sohn and Kim 2001). Valvular regurgitation was assigned the following scores: 0 (none), 1 (trace), 2 (mild), 3 (moderate), and 4 (severe). Mitral and aortic valve gradients and regurgitation scores for the cohort were recorded at baseline, 48 and 96 weeks. Three subjects had undergone mitral valve repair or replacement (two before and one during the trials) or aortic valvuloplasty (one before the trials). For purposes of this review, peak systolic aortic gradient was the only variable analyzed after mitral valve replacement in these three subjects. Additional cardiac anomalies were noted when found.
Ultrasound reports were obtained and reviewed retrospectively. Data from the phase I/2 study and phase 3 study were analyzed for differences between combined reduced dose (0.2 mg/kg, phase 1/2 low-dose group) or delayed dose (phase 3, placebo group) and standard dose (1 mg/kg) treatment. Data were pooled from all three treatment trials (phase 1/2, phase 2, and phase 3) and then analyzed for baseline values and for differences between baseline and 24–48 and 72–96 weeks of treatment with galsulfase.
Data were analyzed using all available data and then re-analyzed using only those subjects for whom data were available at all three study points (baseline, weeks 48 and 96) of galsulfase treatment.
Statistical analysis
Initial analyses were based on analysis of variance models or Student’s t-test to assess differences in demographic variables at baseline between the various subgroups compared. Analysis of differences by gender and by age (<12 years versus ≥12 years) were made both at baseline and between weeks 24–48 and 72–96. Finally, the major hypotheses were evaluated using general linear models and performed for all subjects for whom data were available and again for subjects for whom data were available at all three study points of galsulfase treatment (Pettersen et al. 2008; Diggle et al. 2012). The models investigated differences over the three time points between and within each of the two treatment groups (reduced or delayed vs. standard dose). To estimate more efficient and unbiased regression parameters of data collected as repeated measures over time, the generalized estimating equation approach of Zeger and Liang was used (Diggle et al. 2012). This allowed specification of a working correlation matrix that accounts for the within-subject correlations. A significance level of 0.05 was used for all statistical tests. Data were analyzed using SAS version 9.2.
Results
Baseline studies
The mean age for the entire group was 11.8 ± 5.4 (range 6–29) years; 37 (68 %) were females and 17 (32 %) males. The mean urinary GAG of 341.4 ± 120.5 μg GAG/mg creatinine was elevated and concomitant mean age-adjusted stature (102.5 ± 13 cm) reduced (Table 3), suggesting more severe MPS VI disease in this group of individuals as has been previously reported by others (Swiedler et al. 2005). Height, weight, and body surface area differed by age (p = 0.008, 0.0008, and 0.001, respectively, data not shown); however, there was no difference in height, weight, or urinary GAG either by gender (p = 0.373, 0.373, and 0.235, respectively) or in GAG by age (p = 0.224).
Cardiac dimensions and function
Cardiac findings for the 54 subjects before the initiation of ERT are listed in Table 4. Males and females did not significantly differ in age (12.2 ± 6 vs. 11.7 ± 5.2 years, p = 0.742) or in any measured cardiac parameter (data not shown), thus both genders were grouped together for all subsequent analyses. The mean z-score of left ventricular end-diastolic dimension (LVED) was within 1 SD of normal at baseline for all participants, regardless of age. By contrast, the mean z-score of LVES was 1.2 SD smaller than normal in those ≥12 years of age, a finding that just reached statistical significance (p = 0.039) when compared to those <12 years. Despite this finding, SF was within normal limits for all participants, regardless of age. The mean z-scores for left ventricular wall thicknesses (LVPWd, IVSd) were increased to 1.4 –1.9 SD greater than normal at baseline for all participants regardless of age (p = 0.858 and 0.229, respectively) in keeping with the infiltrative nature of the lysosomal storage diseases.
Cardiac valves
Before ERT, the mean mitral valve gradient of 7.28 ± 5.68 mmHg was higher than normal (<5 mmHg) (Lopez et al. 2010; Hatle and Angelsen 1985; Baumgartner et al. 2009; Sohn and Kim 2001), indicating obstruction to flow (mitral stenosis) prior to institution of galsulfase therapy. The mitral gradient was significantly greater for subjects ≥12 vs. <12 years (9.69 ± 6.46 vs. 5.15 ± 3.98 mmHg, respectively, p = 0.022) (Table 4). Two of the three mitral valve replacements were performed in those >12 years of age. For the entire cohort, the mitral valve was mildly regurgitant at baseline (score 1.35 ± 1.05). In contrast to mitral stenosis, mitral regurgitation was significantly less in older subjects (mitral regurgitation score 1.00 ± 0.93 vs. 1.58 ± 1.01 for subjects ≥12 vs. <12 years, p = 0.044).
The aortic valve was less affected than the mitral before ERT. The peak systolic gradient across the aortic valve for the entire group of 13.72 ± 10.78 mmHg was at the upper limit of childhood normal values (11–13 mmHg) (Lopez et al. 2010; Hatle and Angelsen 1985; Baumgartner et al. 2009; Sohn and Kim 2001). As with the mitral valve, the aortic gradient was significantly greater in older participants (18.77 ± 13.68 vs. 9.24 ± 3.90 mmHg, p = 0.015). Aortic valvuloplasty was performed in one subject >12 years of age before the initiation of therapy. Aortic regurgitation was barely perceptible at baseline (aortic regurgitation score of 0.53 ± 0.87 equivalent to trace regurgitation) and did not differ between older and younger subjects (p = 0.104 for age ≥12 vs. <12 years).
Other cardiac anomalies
Other cardiac anomalies were rare in this group of subjects, but included one subject with partial anomalous pulmonary venous return, sinus venosus atrial septal defect, and pulmonary stenosis, who had undergone pulmonary valvotomy.
Studies after galsulfase treatment
Cardiac dimensions and function
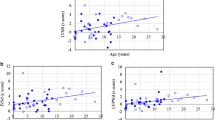
Data from the entire cohort are presented in Table 5, while data from subjects in whom all three time points were available (before ERT, weeks 24–48, and weeks 72–96) are presented in Table 6. After 96 weeks of enzyme, the mean z-score for LVED remained unchanged (p = 0.150, p = 0.146, respectively) and normal (Table 5, Table 6) for both groups. The mean z-score for left ventricular systolic dimension (LVES) increased significantly (p = 0.034) during therapy for the entire cohort but not for those in whom all three time points were available (p = 0.053), but this change did not adversely affect cardiac function since the SF remained normal for both groups throughout the study (p = 0.208, p = 0.135, respectively). For both the entire cohort and for those in whom all three time points were available, the mean z-score for left ventricular posterior wall thickness (LVPWd) remained increased and did not change (p = 0.551, p = 0.510, respectively) after 96 weeks of enzyme, but the mean z-score for IVSd decreased significantly (p < 0.0001and p < 0.0001, respectively) during this period. One subject was lost to follow-up after baseline studies. Analysis of data with and without his inclusion did not alter results. Prior to combining data from the two groups, we had examined all data as a function of time, comparing standard vs. reduced or delayed enzyme. We observed a significant time versus group interaction (p = 0.0396) for IVSd (Table 5, footnote 1, Figure A).
Because there was no statistical difference in wall thickness between the entire cohort and those in whom all three measurement points were available, we analyzed the data for those <12 years of age vs. those ≥12 years of age from the entire cohort. Treatment with galsulfase appeared to have more effect when administered to those <12 years of age (Table 7). For those subjects <12 years of age, the mean z-score for IVSd reflected significantly less hypertrophy (p < 0.0001) while for those ≥12 years it did not change (p = 0.318).
Cardiac valves
After 96 weeks of enzyme, neither mitral valve obstruction (MMV) nor mitral valve regurgitation (MRS) changed in either the entire cohort or in those in whom all three measurement points were available (MMV: p = 0.552, p = 0.971, respectively, and MRS: p = 0.459, p = 0.402, respectively, Tables 5 and 6). Aortic valve obstruction remained unchanged for both the entire cohort and for those in whom all three time points were available (p = 0.150, p = 0.516, respectively) during the studies, but aortic regurgitation increased significantly (p = 0.004, p = −0.008, respectively) while still remaining within the “trace to mild” category. As discussed above, prior to combining data from the two groups, we examined the pattern over time for each group (standard vs. reduced or delayed) to learn if it was similar for the two groups. We observed a significant time versus group interaction (p = 0.019) for aortic regurgitation (Table 5, footnote 2, Figure B) although again we could not identify any reasonable explanation as to why this would be the case.
When the entire cohort was analyzed by age <12 vs. ≥12 years, neither mitral nor aortic valve stenosis changed after 96 weeks of therapy. Mitral regurgitation did not increase in either age group (Table 7) after 96 weeks of treatment, but aortic valve regurgitation score increased in those ≥12 years of age (p = 0.015).
Discussion
The cardiovascular system is progressively and unambiguously affected in individuals with MPS VI. Left ventricular hypertrophy, as well as anatomic and functional abnormalities of the mitral and aortic valves, have previously been well described by others (Lael et al. 2010; Dangel 1998; Wippermann et al. 1995; Azevedo et al. 2004; Scarpa et al. 2009; Fesslova et al. 2009). Our data obtained prior to the initiation of ERT from a large number of severely affected subjects with MPS VI support these observations but, more importantly, describe the cardiac effects of long-term treatment with galsulfase ERT.
Prior to ERT, left ventricular hypertrophy and mitral valve stenosis were the most prominent cardiac features found by this study. Left ventricular hypertrophy was severe, with mean z-scores approaching 2 SD greater than normal, and was found in subjects of all ages. The mean gradient across the mitral valve was elevated at baseline and increased significantly when those <12 years of age were compared to those ≥12. Mitral valve replacement, performed in three subjects before, or during, these studies confirmed the severity of this finding. By contrast, mitral valve regurgitation, usually a more common finding in most MPS VI pediatric reports (Lael et al. 2010; Dangel 1998; Wippermann et al. 1995; Azevedo et al. 2004; Scarpa et al. 2009; Fesslova et al. 2009) was only mild in our subjects. The presence of mitral stenosis, rather than regurgitation, has been found in older individuals with MPS VI (Diggle et al. 2012; Marwick et al. 1992; Tan et al. 1992) and is consistent with the older age of the subjects in this study.
Aortic valve obstruction at baseline was significantly greater in those 12 years of age or older but, when compared to mitral obstruction, was milder. Only one subject underwent aortic valvuloplasty prior to initiation of enzyme treatment. Only trace aortic regurgitation was present at baseline, a finding considered not physiologically significant.
Long-term enzyme replacement therapy with galsulfase was associated with maintenance of normal left ventricular function in all subjects in this study and regression of left ventricular septal hypertrophy in those who initiated treatment before 12 years of age. This remained true when we evaluated the entire cohort as well as when we analyzed only those in whom all three measurement points were available. During the course of this study, cardiac valve stenosis neither worsened nor improved, regardless of age. Aortic valve regurgitation increased significantly—but not physiologically—after 96 weeks of enzyme replacement in subjects ≥12 years of age. Although this finding had little physiologic consequence to these individuals, it may imply that cardiac valve pathology, once begun, may not be reversible. This progression of aortic regurgitation in the ≥12 years of age group is most likely due to underlying disease. It is difficult to assess causal relationship with ERT treatment given that the treatment group was followed for 96 weeks, placebo for 24 weeks, and echocardiography was not assessed after 24 weeks of treatment or placebo.
Valve obstruction is identified by the measurement of increased Doppler flow velocities across cardiac valves. With a normal cardiac output, the maximum normal Doppler velocity across the mitral valve is 1.3 m/s or 6.7 mmHg in children (Hatle and Angelsen 1985). The mean mitral gradient, a more accurate measure of obstruction, is obtained by averaging the instantaneous mitral flow velocities throughout diastole, resulting in a lower value. Mean mitral valve gradients <5 mmHg are consistent with mild mitral obstruction in adults; no values have been established for children (Baumgartner et al. 2009). The maximum normal Doppler velocities across the aortic valve in adults and children are 1.7–1.8 m/s, respectively, corresponding to peak aortic gradients of 11–13 mmHg (Hatle and Angelsen 1985). At baseline the mean mitral and aortic valve gradients in our subjects exceeded normal values and were greater in older subjects, consistent with the progressive nature of MPS VI.
The lack of response of the cardiac valves to ERT is similar to that reported in a small series of MPS VI patients who underwent hematopoietic stem cell transplantation (HSCT) and were studied an average of 5 (range 1.8–9) years after the procedure (Herskhovitz et al. 1999). The relatively avascular nature of cardiac valve tissue (Dow and Harper 1932) may, in part, explain the lack of improvement in valve morphology and function with either HSCT or ERT. Irreversible valve damage accruing over years may also explain the lack of response in older children and young adults (such as the subjects of this study) to any type of intervention. In support of early intervention, galsulfase, given from 8 weeks of life, has been shown to prevent cardiac abnormalities altogether (McGill et al. 2010).
Although this study had a large number of subjects with MPS VI who were studied over a lengthy time period, there are limitations to the study. The placebo group was followed for only the first 24 weeks of the phase 3 study. If follow-up had been extended for a longer time period, other differences between the placebo and treated groups may have been identified. The second limitation of this study is that ultrasounds were performed and analyzed at local sites. The concept of a central echocardiographic facility to provide reliable and reproducible data for multicenter pediatric cardiac studies emerged during the course of these trials (Lipschultz et al. 2001). Cardiac ultrasound in subjects with MPS can be difficult due to abnormalities of the thorax, poor lung expansion from hepatomegaly and restrictive lung disease, and inability to extend the neck. Comparison of M-mode measurements made in the field versus the central location in two different pediatric studies (Lipschultz et al. 2001; Dai et al. 1999) suggests that repeated measurements from the field may be more reliable than a single measurement. Thus although inter-institutional differences may have affected the absolute values obtained in this study, it is likely that trends (repeated values from the same sites) were less affected.
Summary
Left ventricular hypertrophy and significant mitral valve obstruction are reported in 54 individuals with MPS VI ranging from 6 to 29 years of age undergoing treatment trials with galsulfase. Long-term enzyme replacement with galsulfase was associated with stable left ventricular function in all subjects and regression of intraventricular septal hypertrophy when enzyme therapy began before the age of 12 years. Despite long-term enzyme therapy, cardiac valve stenosis remained unchanged in all subjects. Aortic regurgitation increased statistically, but not physiologically, only in those who began enzyme at 12 or more years of age. The evidence presented suggests that the underlying pathological changes due to GAG accumulation, especially in the valves, may be poorly reversible and that early initiation of galsulfase therapy may be beneficial.
References
Azevedo ACMM, Schwartz IV, Kalakun L, Brustolin S, Burin MG, Beheregaray APC, Leistner S, Giugliani C, Rosa M, Barrios P, Marinho D, Esteves P, Valadares E, Boy R, Horovitz D, Mabe P, de Silva LCA, de Souza ICN, Ribeiro M, Martins AM, Palhares D, Kim CA, Giugliani R (2004) Clinical and biochemical study of 28 patients with mucopolysaccharidosis type VI. Clin Genet 66:208–213
Baumgartner H, Hung J, Bermejo J, Chambers JB, Evangelista A, Griffin BP, Iung B, Otto CM, Pellikka PA, Quinones M (2009) Echocardiographic assessment of valve stenosis: EAE/ASE recommendations for clinical practice. J Am Soc Echocardiogr 22:1–23
Dai S, Ayres NA, Harrist RB, Bricker JT, Labarthe DR (1999) Validity of echocardiographic measurement in an epidemiological study: Project HeartBeat! Hypertension 34:236–241
Dangel JH (1998) Cardiovascular changes in children with mucopolysaccharide storage disease and related disorders—clinical and echocardiographic findings in 64 patients. Eur J Pediatr 157:534–538
Decker C, Yu ZF, Giugliani R, Schwartz IV, Guffon N, Teles EL, Miranda MC, Wraith JE, Beck M, Arash L, Scarpa M, Ketteridge D, Hopwood JJ, Plecko B, Steiner R, Whitley CB, Kaplan P, Swiedler SJ, Conrad S, Harmatz P (2010) Enzyme replacement therapy for mucopolysaccharidosis VI: growth and pubertal development in patients treated with recombinant human N-acetylgalactosamine 4-sulfatase. J Pediatr Rehabil Med 3(2):89–100
Diggle PJ, Heagerty P, Liang KY, Zeger SL (2002) Analysis of longitudinal data, 2nd ed. Oxford University Press, New York
Dow DR, Harper WF (1932) The vascularity of the valves of the human heart. J Anat 66(Pt 4):610–617
Dyar D (2012) Parameter(z). Pediatric and fetal echo z-score calculators.http://parameterz.blogspot.com/
Fesslova V, Corti P, Sersale G, Rovelli A, Russo P, Mannarino S, Butera G, Parini R (2009) The natural course and the impact of therapies of cardiac involvement in the mucopolysaccharidoses. Cardiol Young 19:170–178
Hachida M, Nonoyama M, Bonkohara Y, Hanyama N, Koyanagi H (1996) Combined aortic and mitral valve replacement in an adult with mucopolysaccharidosis (Maroteaux-Lamy syndrome). Heart Vessel 11:215–217
Harmatz P, Whitley CB, Waber L, Pais R, Steiner R, Plecko B, Kaplan P, Simon J, Butensky E, Hopwood JJ (2004) Enzyme replacement therapy in mucopolysaccharidosis VI (Maroteaux-Lamy syndrome). J Pediatr 144:574–580
Harmatz P, Ketteridge D, Giugliani R, Guffon N, Teles EL, Sa Miranda MC, Yu Z-F, Swiedler SJ, Hopwood JJ, and for the MPS VI Study Group (2005) Direct comparison of measures of endurance, mobility, and joint function during enzyme-replacement therapy of mucopolysaccharidosis VI (Maroteaux-Lamy syndrome): results after 48 weeks in a phase 2 open-label clinical study of recombinant human N-acetylgalactosamine 4-sulfatase. Pediatrics 115:e681–e689
Harmatz P, Giugliani R, Schwartz, Guffon N, Teles EL, Sa Miranda MC, Wraith JE, Beck M, Arash L, Scarpa M, Yu Z-F, Wittes J, Berger KI, Newman MS, Iowe AM, Kakkis E, Swiedler SJ, for the MPS VI Phase 3 Study Group (2006) Enzyme replacement therapy for mucopolysaccharidosis VI: a phase 3, randomized, double-blind, placebo-controlled, multinational study of recombinant human N-acetylgalactosamine 4-sulfatase (recombinant human arylsulfatase B or rhASB) and follow-on, open-label extension study. J Pediatr 148:533–539
Harmatz P, Giugliani R, Schwartz IDV, Guffon N, Teles EL, Sa Miranda MC, Wraith JE, Beck M, Aash L, Scarpa M, Ketteridge D, Hopwood JJ, Plecko B, Steiner R, Whitley CB, Kaplan P, Yu Z-F, Swiedler SJ, Decker C, for the MPS VI Study Group (2008) Long-term follow-up of endurance and safety outcomes during enzyme replacement therapy for mucopolysaccharidosis VI: final results of three clinical studies of recombinant human N-acetylgalactosamine 4-sulfatase. Mol Gen Metab 94:469–475
Harmatz P, Yu Z-F, Giugliani R, Schwartz IVD, Guffon N, Teles EL, Sa Miranda MC, Wraith JE, Beck M, Arash L, Scarpa M, Ketteridge D, Hopwood JJ, Plecko B, Steiner R, Whitley CB, Kaplan P, Swiedler SJ, Hardy K, Berger KI, Decker C (2010) Enzyme replacement therapy for mucopolysaccharidosis VI: evaluation of long-term pulmonary function in patients treated with recombinant human N-acetylgalactosamine 4-sulfatase. J Inherit Metab Dis 33:51–60
Hatle L, Angelsen B (1985) In: Doppler ultrasound in cardiology. Physical principles and clinical applications, 2nd ed. Philadelphia: Lea-Febiger, p 93
Herskhovitz E, Young E, Rainer J, Hall CM, Lidchi V, Chong K, Vellodi A (1999) Bone marrow transplantation for Maroteaux-Lamy syndrome (MPS VI): long-term follow-up. J Inher Metab Dis 22:50–62
Kampmann C, Wiethoff CM, Wenzel A, Stolz G, Betancour M, Wippermann C-F, Huth R-G, Habermehl P, Knuf M, Emschermann T, Stopfkuchen H (2000) Normal values of M mode echocardiographic measurements of more than 2000 healthy infants and children in central Europe. Heart 83:667–672
Lael GN, de Paula AC, Leone C, Kim CA (2010) Echocardiographic study of paediatric patients with mucopolysaccharidosis. Cardiol Young 20:254–261
Lipschultz SE, Easley KA, Orav EJ, Kaplan S, Starc S, Bricker JT, Lai WW, Moodie DS, Sopko G, Schluchter MD, Colan SD (2001) Reliability of multicenter pediatric echocardiographic measurements of left ventricular structure and function: the prospective P2C2 HIV study. Circulation 104:310–316
Lopez L, Colan SD, Frommelt PC, Ensing GL, Kendall K, Younoszai AK, Lai WW, Geva T (2010) Recommendations for quantification methods during the performance of a pediatric echocardiogram: a report from the Pediatric Measurements Writing Group of the American Society of Echocardiography Pediatric and Congenital Heart Disease Council. J Am Soc Echocardiog 23:465–495
Marwick TH, Bastian B, Hughes CF, Bailey BP (1992) Mitral stenosis in the Maroteaux-Lamy syndrome: a treatable cause of dyspnoea. Postgrad Med J 68:287–288
McGill JJ, Inwood AC, Coman DJ, Lipke ML, de Lore D, Swiedler SJ, Hopwood JJ (2010) Enzyme replacement therapy for mucopolysaccharidosis Vi from 8 weeks of age—a sibling control study. Clin Genet 77:492–498
Neufeld EF, Muenzer J (2001) The mucopolysaccharidoses. In: Scriver CR, Beaudet AL, Valle D, Sly WS (eds) The metabolic basis of inherited diseases, 8th ed. Mc Graw-Hill, New York, pp 3421–3452
Pettersen MD, Du W, Skeens ME, Humes RA (2008) Regression equations for calculation of z scores of cardiac structures in a large cohort of healthy infants, children, and adolescents: an echocardiographic study. J Am Soc Echocardiogr 21:922–934
Scarpa M, Barone R, Fiumara A, Astarita L, Parenti G, Rampazzo A, Sala S, Sorge G, Parini R (2009) Mucopolysaccharidosis VI: the Italian experience. Eur J Pediatr 168:1203–1206
Sohn S, Kim HS (2001) Doppler aortic flow velocity measurement in healthy children. J Korean Med Sci 16:140–144
Swiedler SJ, Beck M, Balbouj M, Giugliani R, Schwartz I, Harmatz P, Wraith JE, Roberts J, Ketteridge D, Hopwood JJ, Guffon N, Sa Miranda MC, Teles EL, Berger KI, Pisca-Nichols C (2005) Threshold effect of urinary glycosaminoglycans and the walk test as indicators of disease progression in a survey of subjects with mucopolysaccharidosis VI (Maroteaux-Lamy Syndrome). Am J Med Gen 134A:144–150
Tan CTT, Schaff HV, Fletcher AM Jr, Edwards WD, Karnes PS (1992) Valvular heart disease in four patients with Maroteaux-Lamy syndrome. Circulation 85:188–195
Wippermann C-F, Beck M, Schranz D, Huth R, Michel-Behnke I, Jungst B-K (1995) Mitral and aortic regurgitation in 84 patients with mucopolysaccharidoses. Eur J Pediatr 154:98–101
Acknowledgments
We acknowledge the participation of study patients and their families and the expert assistance of all study site coordinators and study site personnel. This study was an investigator-initiated study sponsored by BioMarin Pharmaceutical Inc., and supported, in part, with funds provided by the National Center for Research Resources, 5 M01 RR-01271 (Dr. Harmatz), 5 M01 RR-00400 (Dr. Whitley), M01 RR-00334 (Dr. Steiner), and UL1-RR-024134 (Dr. Kaplan). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Research Resources or the National Institutes of Health. The support of the European Consortium for Lysosomal Diseases (EUCLYD, 7th Framework program, European Union) is acknowledged (Dr. Beck).
BioMarin reviewed the manuscript to insure the accuracy of all statements regarding enzyme replacement therapy with galsulfase. All authors participated in the galsulfase clinical trials, collection of data, development and writing of the manuscript and are fully responsible for its content.
*The MPS VI Study Group co-investigators are John Waterson, MD, PhD and Elio Gizzi, MD, Children’s Hospital & Research Center Oakland, Oakland, CA; Yasmina Amraoui, MD, Children’s Hospital, University of Mainz, Germany; Bonito Victor, MD, Unidade de Doenças Metabólicas, Departamento Pediatria, Hospital de Sao João, Porto, Portugal; Javier Arroyo, MD, Hospital San Pedro de Alcantara, Hospital de día de Pediatría, Caceres, Spain; D.N. Bennett-Jones, MD, Consultant General and Renal Physician, Whitehaven, UK; Philippe Bernard, MD, Centre Hospitalier d’Arras, Arras, France; Prof. Billette de Villemeur, Hôpital Trousseau, Paris, France; Raquel Boy, MD, Hospital Universitário Pedro Ernesto, Rio de Janeiro, Brazil; Eduardo Coopman, MD, Hospital del Cobre De. Salvador, Calama, Chile; Prof. Rudolf Korinthenberg, Universitätsklinikum Freiburg, Zentrum für Kinderheilkunde und Jugendmedizin, Klinik II Neuropädiatrie und Muskelerkrankungen, Freiburg, Germany; Michel Kretz, MD, Hôpital Civil de Colmar, Le Parc Centre de la Mère et de l’Enfant, Colmar, France; Shuan-Pei Lin, MD, MacKay Memorial Hospital, Department of Genetics, Taipei, Taiwan; Ana Maria Martins, MD, UNIFESP, Instituto de Oncologia Pediátrica, GRAACC/UNIFESP, Departamento de Pediatria, São Paulo, Brazil; Anne O’Meara, MD, Our Lady’s Hospital for Sick Children, Dublin, Ireland; Gregory Pastores, MD, PhD, NYU Medical Center, Rusk Institute, New York, NY; Lorenzo Pavone, MD, Rita Barone, MD, Agata Fiumara, MD, and Prof. Giovanni Sorge, Department of Pediatrics, University of Catania, Catania, Italy; Silvio Pozzi, MD, Ospedale Vito Fazzi, UO Pediatria, Lecce, Italy; Uwe Preiss, MD, Universitätsklinik und Poliklinik fűr Kinder, Halle, Germany; Emerson Santana Santos, MD, Fundação Universidade de Ciências da Saúde de Alagoas Governador, Departamento de Pediatria, Maceió, Brazil; Isabel Cristina Neves de Souza, MD, and Luiz Carlos Santana da Silva, PhD, Universidade Federal do Pará, Centro de Ciências Biológicas, Hospital Universitário João de Barros Barreto, Belém, Brazil; Eugênia Ribeiro Valadares, MD, PhD, Hospital das Clínicas, Faculdade de Medicina da Universidade Federal de Minas Gerais-UFMG, Avenida Professor Alfredo Balena, Belo Horizonte-Minas Gerais, Brazil; Laura Keppen, MD, Department of Pediatrics, University of South Dakota School of Medicine, Sioux Falls, SD; David Sillence, MD, Children’s Hospital, Westmead, Australia; Lionel Lubitz, MD, Royal Children’s Hospital, Melbourne, Australia; William Frischman, MD, The Townsville Hospital, Townsville, Australia; Julie Simon, RN, Children’s Hospital & Research Center Oakland, Oakland, CA; Claudia Lee, MPH, Children’s Hospital & Research Center Oakland, Oakland, CA; Stephanie Oates, RN, Metabolic Unit, SA Pathology at Women’s and Children’s Hospital Adelaide, North Adelaide, Australia; Lewis Waber, MD, PhD, Pediatric Genetics and Metabolism, University of Texas Southwest Medical Center, Dallas, TX; Ray Pais, MD, Pediatric Hematology/Oncology, East Tennessee Children’s Hospital, Knoxville, TN; Laila Arash, MD, Children's Hospital, University of Mainz, Germany; Robert Steiner MD, Departments of Pediatrics and Molecular and Medical Genetics, Oregon Health & Science University, Portland, OR; Chester B Whitley, PhD, MD, University of Minnesota Medical School, Minneapolis, MN; Paige Kaplan, MD, Children’s Hospital of Philadelphia, Philadelphia, PA; Barbara Plecko, MD, Univ. Klinik für Kinder und Jugendheilkunde, Graz, Austria.
Conflict of interest
Drs. Harmatz, Beck, and Giugliani have provided consulting support to BioMarin Pharmaceutical Inc., Novato, CA. Drs. Harmatz, Beck, Scarpa, and Braunlin reported receiving a speaker’s honorarium and travel support from BioMarin. Drs. Harmatz and Scarpa have received research grants from BioMarin. BioMarin is a supporter of the Lysosomal Disease Network’s WORLD Symposium organized by Dr. Whitley. Drs. Decker and Imperiale are employees of BioMarin Pharmaceutical Inc.; both are stockholders. Andrea Schatz is an employee of BioMarin.
Open Access
This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Communicated by: Gregory M. Pastores
*The MPS VI Study Group co-investigators (see Acknowledgment section)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 2.0 International License (https://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Braunlin, E., Rosenfeld, H., Kampmann, C. et al. Enzyme replacement therapy for mucopolysaccharidosis VI: long-term cardiac effects of galsulfase (Naglazyme®) therapy. J Inherit Metab Dis 36, 385–394 (2013). https://doi.org/10.1007/s10545-012-9481-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10545-012-9481-2