
Abstract
Mucopolysaccharidosis type II (MPS II; Hunter syndrome) is an X-linked, recessive, lysosomal storage disorder caused by deficiency of iduronate-2-sulfatase. It has multisystemic involvement, with manifestations in the brain, upper respiratory tract, heart, abdomen, joints and bones. Bone involvement leads to decreased growth velocity and short stature in nearly all patients. A therapeutic option for patients with MPS II is enzyme replacement therapy (ERT) with idursulfase (Elaprase®). We compared annual growth rates before and during ERT in 18 patients from Mainz, Germany, and Manchester, UK. Group 1 included nine patients who started ERT before 10 years of age; group 2 contained nine patients aged more than 10 years at the start of ERT. All patients had received weekly or biweekly ERT or placebo for 1 year, followed by ERT for more than 3 years. For patients in group 1, the mean (± SD) height increase was 14.6 ± 5.5 cm during 3 years of ERT. Only one patient in this group (who was below the 3rd percentile when starting ERT) deviated from the normal growth curve over this time. Patients in group 2 had a mean height increase of 8.1 ± 1.7 cm after 3 years of ERT compared with an increase of 1 cm in the year before ERT. ERT seems to have a positive influence on growth in patients with MPS II. Most benefit is seen in patients beginning ERT before the age of 10 years. This supports the recommendation that ERT should be started as early as possible in patients with MPS II.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Mucopolysaccharidosis type II (MPS II or Hunter syndrome; OMIM 309900) is an X-linked recessive disease caused by a deficiency of the lysosomal enzyme iduronate-2-sulfatase, which catalyses the degradation of the glycosaminoglycans (GAGs) dermatan sulfate and heparan sulphate (Neufeld and Muenzer 2001). This enzyme deficiency leads to progressive lysosomal storage of non-degraded GAGs in nearly all cell types, tissues and organs. The phenotypic expression of MPS II is thought to be due to the intracellular accumulation of GAGs.
Phenotypic expression varies considerably. Clinically, MPS II should be regarded as a continuum between the two extreme forms of the disease (severe and attenuated). Patients with severe MPS II may exhibit somatic involvement between 2 and 4 years of age, with variable progressive neurological involvement leading to mental impairment. In these patients, death occurs in the first or second decade of life, usually due to progressive neurodegeneration, associated with obstructive airway disease and/or cardiac failure (Neufeld and Muenzer 2001).
Although the clinical course for the more severely affected patients is relatively predictable, there is considerable variability in the clinical phenotype and progression of the attenuated form of the disease. In patients with the attenuated form of MPS II, there is minimal neurological involvement, and patients can survive into young adulthood. They may, however, present with mild-to-moderate learning difficulties and often have symptoms and complications that cause significant morbidity and disability. Both severely affected individuals and those with attenuated disease have a range of symptoms including short stature, dysostosis multiplex, hearing impairment, enlarged tongue, abnormal dentition, upper airway obstruction, hepatosplenomegaly and joint contractures associated with a decreased range of joint movement.
Infants with MPS II appear normal at birth, and early developmental milestones may also be within the normal range; in the first years of life the height of most patients with MPS II is above the 50th percentile and in some cases is over the 97th percentile. However, growth velocity decreases with age: by the age of 8 years, height is below the 3rd percentile (Schwartz et al. 2007), and nearly all patients exhibit growth retardation before puberty [Hunter Outcome Survey (HOS); unpublished data]. In a prospective study of height in seven Brazilian patients followed-up over 1 year (Pinto et al. 2006), MPS II was associated with a decreased growth velocity compared with year 2000 reference values from the US Centers for Disease Control (CDC) (Kuczmarski et al. 2000).
Physical growth is an issue of paramount importance in paediatric practice and a highly emotive issue for parents. Individuals with short stature encounter many challenges in daily life. In addition, patients with MPS II have serious medical problems and their short stature may make life even more strenuous. The fact that their appearance makes them extremely visible in society puts an additional strain on their lives and those of their parents (Hunter 1998; Moneymaker 1989).
Enzyme replacement therapy (ERT) has been available for patients with MPS II since August 2006 in the USA and since March 2007 in Europe. In a phase II/III clinical trial, ERT with idursulfase (Elaprase®; Shire HGT Pharmaceuticals, Cambridge, MA, USA) produced statistically significant improvements in the primary composite end point—the sum of ranked changes in the 6-min walking test distance and ranked changes in the percentage predicted forced vital capacity—compared with placebo, in patients with attenuated disease (Muenzer et al. 2006).
The effect of ERT on height in patients with MPS I has been reported (Sifuentes et al. 2007). Mean height increased from 139 cm (SD ± 19 cm) at baseline to 159 cm (SD ± 3 cm) at year 6. For patients who started ERT before puberty the mean gain in height was 33 cm. To date, no trial data have been published that examine the effect of ERT on growth in MPS II. The present retrospective analysis of patients enrolled in a clinical trial aimed to assess the effect of ERT on linear growth in patients with the attenuated phenotype of MPS II.
Materials and methods
Patient population
Participants were recruited from the Metabolic Department of the Mainz Children’s Hospital (Germany) and the Royal Manchester Children’s Hospital (UK). All patients and/or parents signed an informed consent form before the study.
The eligible patient population for this analysis consisted of 18 patients: 10 from the Metabolic Department of the Mainz Children’s Hospital and 8 from the Royal Manchester Children’s Hospital. All patients had attenuated disease but with variable organ involvement. No patients had cardiac failure or were on nocturnal respiratory support. No patients had cognitive impairment.
Male patients with a confirmed diagnosis of MPS II, who had commenced ERT with idursulfase before the end of puberty and who had received idursulfase for 3 years were included in this analysis. All patients had previously enrolled in a phase II/III clinical trial of ERT (Muenzer et al. 2006). Patients received ERT with idursulfase, 0.5 mg/kg, either every week (n = 5) or every other week (n = 7), or placebo (n = 6) for the first year. After the first year, all patients received idursulfase on a weekly basis. Patients on long-term oral steroid treatment and those who had previously received growth hormone therapy were excluded from the analysis.
Height measurements were available at all time points (the year before starting ERT, at baseline and at years 1, 2 and 3 on treatment) for 15 patients; complete data were not available for 3 patients (2 patients for the year before starting ERT and 1 patient for 3 years on ERT). Height was measured using a stadiometer according to standard protocols.
Statistical analysis
Two groups of patients were analysed according to their age at the start of ERT (baseline): group 1 included patients under 10 years of age (n = 9); group 2 included patients over 10 years of age (n = 9).
Height measurements were plotted against normal height data for boys obtained from the CDC growth charts (Kuczmarski et al. 2000). These charts were used as they were the ones which had been used in the phase II/III study (Muenzer et al. 2006). A Z score (the number of standard deviations a particular value is from the mean) was calculated for these height measurements and plotted in a similar way.
For each age group, the mean changes in height and Z score (± SD) from baseline were calculated. The velocity and the yearly change in Z score were assessed from the year before to 3 years after the start of ERT. For these analyses, the population was restricted to patients with available data for all time points (n = 15).
The mean change in growth velocity (± SD) was calculated for each time point from the year prior to starting ERT.
Results
For the whole sample (n = 18; age range at baseline, 6–19 years), height was 108–154 cm (median, 126.5 cm); ten of the patients (55.5%) were considered to be of short stature, defined as having a height below the 3rd percentile for age.
In group 1 (n = 9; age range at baseline, 6–9 years) height was 108–130 cm (median, 124 cm); only one boy was of short stature. The mean increase in height over the 3-year period of ERT was 14.6 cm (SD ± 5.5 cm). The growth curves during ERT show that the height of eight of these patients was still within the normal range based on CDC growth charts (Kuczmarski et al. 2000); one patient was more than 2 SD below the mean before starting treatment (Figs. 1 and 2).

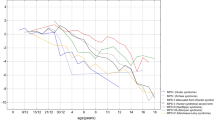
Growth charts for MPS II patients under 10 years of age at the start of enzyme replacement therapy (ERT). The dotted lines illustrate the growth before ERT and the continuous lines the growth on ERT. The shaded area represents the 3rd to the 97th percentiles of height in boys based on CDC growth charts (Kuczmarski et al. 2000)

Z scores for height in MPS II patients under 10 years of age at the start of enzyme replacement therapy (ERT). The dotted lines illustrate the scores before ERT and the continuous lines the scores on ERT (based on CDC growth charts; Kuczmarski et al. 2000).
The Z scores calculated by year were –0.05 ± 0.25 for the first year, and –0.12 ± 0.39 and –0.12 ± 0.57 for the second and third years, respectively. The growth velocity the year before ERT and for 3 years on ERT was calculated in seven patients. This analysis reveals an increase in height of about 3 cm (Z score = −0.5) the year before ERT and 5.3 cm (Z score = 0.02), 4.5 cm (Z score = −0.07) and 5.7 cm (Z score = 0.08) for the first, second and third years on ERT respectively (Figs. 3 and 4).

Yearly growth velocity for patients with MPS II under 10 years of age at the start of enzyme replacement therapy (ERT)

Z scores for data in Fig. 3 (MPS II patients under 10 years of age at the start of enzyme replacement therapy; ERT). A Z score of 0 means that height is at the mean value for the normal population. A negative Z score means that height is below the 50th percentile
In group 2, all nine patients were considered to be of short stature (height range, 121–154 cm; median 130 cm). During 3 years of ERT the mean increase in height was 8.1 ± 1.6 cm. Growth charts and Z scores are shown in Figs. 5 and 6.

Growth charts for MPS II patients over 10 years of age at the start of enzyme replacement therapy (ERT). The dotted lines show the growth before ERT and the continuous lines the growth on ERT. The shaded area represents the 3rd to the 97th percentiles of height in boys based on CDC growth charts (Kuczmarski et al. 2000)

Z scores for height in MPS II patients over 10 years of age at the start of enzyme replacement therapy (ERT). The dotted lines illustrate the scores before ERT and the continuous lines the scores on ERT (based on CDC growth charts; Kuczmarski et al. 2000)
Yearly growth velocity was calculated in all nine patients in group 2. The increase in height was 1.5 cm (Z score = −0.8) in the year before ERT compared with 3.9 cm (Z score = −0.17), 3.6 cm (Z score = 0.23) and 1.3 cm (Z score = −0.06) for the first, second and third years of ERT respectively (Figs. 7 and 8).

Yearly growth velocity for MPS II patients over 10 years of age at the start of enzyme replacement therapy (ERT)

Z score for data in Fig. 7 (MPS II patients over 10 years of age at the start of enzyme replacement therapy; ERT). A Z score of 0 means that height is at the mean value for the normal population. A negative Z score means that height is below the 50th percentile
Discussion
Short stature in MPS is linked to dysostosis multiplex. Typical signs of this skeletal dysplasia are gibbus, scoliosis, epiphyseal dysplasia and degenerative joint disease (Areu et al. 1995). A follow-up study on patients with MPS I on ERT for 6 years did not reveal any distinct changes in dysostosis multiplex (Muenzer et al. 2006). We assume, therefore, that ERT in patients with MPS II will also have little or no effect on these symptoms. Histological examinations of a biopsy from a Hurler syndrome patient or from animal models with different types of MPS revealed pathology of the growth plate possibly related to GAG accumulation (Areu et al. 1995; Silveri et al. 1991; Russell et al. 1998). Pathophysiological studies of the skeletal manifestations of MPS II may also help to understand the effects of ERT.
Although short stature is common to most types of MPS, there are few published data on the effects of ERT on growth in patients with other mucopolysaccharidoses, other than one study in patients with MPS I (Sifuentes et al. 2007). In this report, we describe the first long-term analysis of the effects of ERT on height in children with MPS II. Height measurements were analysed within two age-stratified cohorts. The age cut-off of 10 years was selected because growth in patients with MPS II tends to follow a normal trajectory until 8 years of age after which growth is markedly reduced (Schwartz et al. 2007). Our cohorts reflect this growth pattern; in group 1 (<10 years of age at the start of ERT) only one of the nine patients was considered to be of short stature compared with all nine patients in group 2 (>10 years of age at the start of ERT).
ERT with idursulfase improved growth when given before the age of 10 years. With one exception, the height of boys in group 1 remained above –2 SD even beyond the age of 10 years. The exception was a boy who was already below –2 SD before starting treatment. His relatively poor response may have been associated with the development of antibodies that, in vitro, appear to have had some neutralizing activity. Further studies, however, are needed to determine the clinical significance of the development of antibodies.
The boys in group 2, who were above 10 years of age at the start of ERT, also showed an increase of growth velocity in their first 2 years of ERT compared with the year before ERT; growth rate in the third year was similar to that in the year before ERT. It is possible that this slower growth rate during the third year of treatment is related to the completion of puberty in these older boys. However, this cannot be confirmed, as the stage of puberty was not documented in this population. Also, patients with MPS II may have delayed puberty. It is important to note that the height of two of the boys in this group was above the 3rd percentile for age at the start of treatment and that one of the patients was particularly short, with a height Z score of approximately –7 at the start of treatment.
The continued increase in height over 3 years, particularly in the group aged under 10 years at the start of ERT, almost certainly represents real growth and is not due to patients standing straighter because of a reduction in joint contractures. In fact, an increase in height can contribute to joint contractures until the muscles and tendons adapt to the new bone growth. Physiotherapy may be beneficial in this respect, resulting in reduction of joint contractures and an apparent increase in height.
A recent non-age-stratified analysis of data from HOS revealed a similar growth acceleration in patients with MPS II given ERT with idursulfase for at least 1 year (Beck et al. 2008). HOS is a multinational long-term outcomes survey covering the natural history of Hunter syndrome and the safety and effectiveness of ERT with idursulfase. Ongoing collection of data in HOS, including analysis of the response to ERT and pubertal development status, will further elucidate the effect of ERT with idursulfase on growth.
Studies into the effects of short stature and the response to ERT are important as there is an assumption that short stature may lead to psychosocial stress in childhood and adolescence (Siegel et al. 1991), which may be at least partially relieved by bringing height closer to the mean for age. One study has shown a significant correlation between adult short stature and health-related quality of life (HRQoL), which suggests that increasing final height in children with short stature may be beneficial and could enhance HRQoL outcomes (Christensen et al. 2007).
There has been limited research on the psychological and social effects of stature in patients with MPS II, although one study reports significant psychosocial problems in teenagers and young adults (Young and Harper 1981). For young adults with short stature due to growth hormone deficiency, childhood onset of renal failure or Turner syndrome, the opportunity for having a partner was low (Busschbach et al. 1998). Young adults with MPS II in our clinics also report problems in finding a partner.
It is unwise, however, to extrapolate the findings from general research into the effects of short stature. Individuals with MPS II have dysmorphism, pain and other medical complications and so might encounter very different psychosocial and HRQoL problems than those with other causes of short stature. Nevertheless, as in many similar diseases, short stature serves as a distinguishing characteristic for MPS II. An increase of height towards normal would remove one of the most visible features of the disease, which may have a positive impact on both the patients and their parents.
Conclusions
MPS II is a severe progressive multisystemic disorder that has the potential to cause disease in most body systems and is associated with small stature. ERT has been shown to be effective in treating many of the manifestations of MPS II, especially if started early in the course of the disease. The present data show that ERT with idursulfase also has a positive effect on growth velocity in patients with MPS II. The effect is more obvious in patients who started ERT before the age of 10 years. This is the first published report of the impact of ERT on growth in young patients with Hunter syndrome. Further analyses in larger groups of patients will be needed to add to these findings.
Abbreviations
- CDC:
-
US Centers for Disease Control
- ERT:
-
Enzyme replacement therapy
- GAGs:
-
Glycosaminoglycans
- HRQoL:
-
Health-related quality of life
- HOS:
-
Hunter Outcome Survey
- MPS II:
-
Mucopolysaccharidosis type II
References
Areu S, Hayden J, Berthold P et al (1995) Growth plate pathology in feline mucopolysaccharidosis VI. Calcif Tissue Int 57(3):185–190
Beck M, Muenzer J, Scarpa M, Schulze Frenking G, Wraith E, on behalf of the HOS investigators (2008) Effect of enzyme replacement therapy on growth in patients with Hunter syndrome: results from the Hunter Outcome Survey. Abstract presented at the American Society of Human Genetics 2008. http://www.ashg.org/2008meeting/abstracts/fulltext/f20738.htm. Accessed January 2010
Busschbach JJ, Rikken B, Grobbee DE, De Charro FT, Wit JM (1998) Quality of life in short adults. Horm Res 49(1):32–38
Christensen TL, Djurhuus CB, Clayton P, Christiansen JS (2007) An evaluation of the relationship between adult height and health-related quality of life in the general UK population. Clin Endocrinol (Oxf) 67:407–412
Hunter AGW (1998) Some psychosocial aspects of nonlethal chondrodysplasias: I. Assessment using a life-styles questionnaire. Am J Med Genet 78:1–8
Kuczmarski RJ, Ogden CL, Grummer-Strawn LM et al (2000) CDC growth charts: United States. Adv Data 314:1–27
Moneymaker JM (1989) The social significance of short stature: astudy of the problems of dwarfs and midgets. Loss Grief Care 3:183–189
Muenzer J, Wraith JE, Beck M et al (2006) A phase II/III clinical study of enzyme replacement therapy with idursulfase in mucopolysaccharidosis II (Hunter syndrome). Genet Med 8(8):465–473
Neufeld EF, Muenzer J (2001) The mucopolysaccharidoses. In: Scriver CR, Beandet AL, Sly S, Valle D, Childs B, Kinzler KW, Volgesltein B (eds) The metabolic and molecular basis of inherited disease. McGraw-Hill, New York, pp 3421–3452
Pinto LL, Schwartz IV, Puga AC, Vieira TA, Munoz MV, Giugliani R (2006) Prospective study of 11 Brazilian patients with mucopolysaccharidosis II. J Pediatr (Rio J) 82(4):273–278
Russell C, Hendson G, Jevon G et al (1998) Murine MPS I: insights into the pathogenesis of Hurler syndrome. Clin Genet 53(5):349–361
Schwartz IV, Ribeiro MG, Mota JG et al (2007) A clinical study of 77 patients with mucopolysaccharidosis type II. Acta Paediatr Suppl 96(455):63–70
Siegel PT, Clopper R, Stabler B (1991) Psychological impact of significantly short stature. Acta Paediatr Scand Suppl 377:14–18
Sifuentes M, Doroshow R, Hoft R et al (2007) A follow-up study of MPS I patients treated with laronidase enzyme replacement therapy for 6 years. Mol Genet Metab 90(2):171–180
Silveri CP, Kaplan FS, Fallon MD, Bayever E, August CS (1991) Hurler syndrome with special reference to histologic abnormalities of the growth plate. Clin Orthop Relat Res 269:305–311
Young ID, Harper PS (1981) Psychosocial problems in Hunter’s syndrome. Child Care Health Dev 7:201–209
Financial disclosures
J.E. Wraith and S.A. Jones received honoraria and travel grants to attend meetings sponsored by Shire Human Genetic Therapies; M. Beck has received unrestricted grants, honoraria and travel support to attend meetings sponsored by Shire Human Genetic Therapies. The authors confirm that the content of the article has not been influenced by the sponsors.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Additional information
Communicated by: Frits Wijburg
Competing interest: None declared.
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Schulze-Frenking, G., Jones, S.A., Roberts, J. et al. Effects of enzyme replacement therapy on growth in patients with mucopolysaccharidosis type II. J Inherit Metab Dis 34, 203–208 (2011). https://doi.org/10.1007/s10545-010-9215-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10545-010-9215-2