
Abstract
For many partnered sexual minority men (SMM), PrEP decisions are shaped by their relationships. Recent innovations in HIV risk reduction interventions tailored for partnered SMM include the integration of video-based communication skill building. The purpose of the current study was to examine the responses of 37 SMM in relationships with cismale partners to understand how actual or anticipated conversations between partners may influence PrEP decision making. Results suggested an individual intervention has the ability to elicit detailed content about interactions between partners. When SMM anticipated being in agreement with their partner about PrEP, they described few challenges to discussing HIV prevention. In contrast, when SMM anticipated relationship-related concerns about PrEP, they also anticipated conversations with their partner would be challenging and likely to involve conflict. This often-diminished SMM’s motivation to engage partners and develop shared HIV-prevention goals. These SMM may benefit from integrated communications skills building to overcome challenges and work collaboratively with partners around PrEP use.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Despite the efficacy of pre-exposure prophylaxis (PrEP) to reduce HIV infections, sexual minority men (SMM)—including gay, bisexual and other men who have sex with men—have experienced largely unchanged rates of new HIV infections since 2010 [1]. They continue to account for the highest proportion of HIV diagnoses in the United States—65% of new diagnoses in 2019 [2]. Condomless anal sex (CAS) in the absence of PrEP is the most common mode of HIV transmission [3].
Roughly a decade ago, epidemiological studies estimated that between 35 and 68% of new HIV infections among SMM were transmitted between main or primary (rather than casual or anonymous) partners [4, 5]. Recent evidence suggests that SMM in non-monogamous relationships (where main partners have agreed that sex with outside partners is permissible under some circumstances) engage in CAS with casual partners at rates comparable to single SMM [6, 7]. While partnered SMM who have monogamous sexual agreements (where sex with outside partners is not permitted) are less likely to engage in CAS with casual partners, there is some indication that those who do so actually engage in more frequent CAS than non-monogamous SMM [6].
Partnered SMM and PrEP
Oral tenofovir disoproxil fumarate/emtricitabine (Truvada ®) and tenofovir alafenamide/emtricitabine (Descovy ®) PrEP prevent 97% of HIV infections [8,9,10] when taken daily and are comparably effective with event-driven or intermittent dosing (sometimes referred to as 2-1-1) [11]. PrEP is recommended by CDC for high risk groups, including SMM in non-monogamous or sero-discordant relationships [12], yet uptake and adherence remain a challenge [13,14,15,16]. For SMM in relationships, PrEP uptake and adherence are often associated with sexual agreements concerning casual partners [6], HIV risk perceptions, partner’s drug use [17], and partner’s approval for PrEP use [16].
The decisions partnered SMM make about PrEP initiation, adherence, and sustainment are often shaped by the context of their relationship [18,19,20,21,22]. Two prominent findings have emerged from this work. First, SMM in non-monogamous relationships perceive themselves to be at higher risk for HIV infection than SMM in monogamous relationships [23] and higher perceived risk for HIV acquisition is associated with higher intentions for PrEP use [17]. Correspondingly, they are more likely to get tested for HIV regularly [24], perceive PrEP as more personally relevant [19], have a PrEP prescription [6], discuss PrEP with partners [25], and persuade an HIV negative partner to go on PrEP [26]. Second, relationship functioning (e.g., commitment, satisfaction, trust, and emotional investment) has a paradoxical negative association with HIV prevention. In most instances, being partnered is associated with better health and wellness [27,28,29], and relationship quality is ordinarily correlated positively with health and wellness among partnered people [30]. Similar effects have been observed among SMM for outcomes like depression [31] and substance use [6]. In contrast to this general trend, relationship commitment and emotional investment may serve as deterrents to HIV prevention among SMM. SMM report concerns that condom use would signal a lack of commitment or trust in the relationship and serve as a barrier to emotional closeness [32]. While some evidence suggests that men who believe condoms are a barrier to emotional closeness find PrEP a more appealing HIV prevention strategy, at least some partnered SMM report concerns that going on PrEP would similarly convey a lack of commitment or emotional investment to their partner [19, 20, 33].
Interventions for Partnered SMM
In response to these challenges, novel interventions have been developed to reduce sexual risk among SMM couples in the US. This work was largely catalyzed by the introduction of couples HIV testing and counseling [34]. More recently, dyadic applications of Motivational Interviewing (MI) [35,36,37]; cognitive behavioral [38], and psychoeducation interventions [39] have shown promise. These interventions variously seek to enhance dyadic functioning [35, 36, 39, 40], and thereby increase partners’ motivation to respond constructively when discussing health-related goals. Most also involve the explicit negotiation of health-related goals (e.g., sexual agreements, HIV prevention plans, or limits on substance use) that are shared by both partners [35, 36]. At least some interventions have incorporated specific components that foster adaptive communication skills [35, 36, 39] and strategies for providers to mitigate conflict [41].
While this work has substantial merit, its reach may be limited. Dyadic participation increases the logistical demands of intervention participation. Partners must coordinate their activities to engage in the intervention together. Not all SMM in relationships are willing and able to meet these demands. At least some evidence suggests that those SMM who are less satisfied with their relationships may be the least likely to recruit their partner to participate in couples counseling with them [42]. Individual interventions that address relationship skills building for partnered SMM are therefore a necessary component of a comprehensive HIV prevention strategy. In the absence of such interventions, those SMM in the poorest functioning relationships may be the least likely to receive tailored services.
The integration of communication skills training into individual interventions tailored for partnered SMM is predicated on a number of assumptions arising primarily from Interdependence Theory [43] and the Investment Model [44]. Situations characterized by dyadic ambivalence—those in which partners’ goals or priorities diverge or one partner’s priorities present a threat to the relationship—create the potential for conflict. Conflict in response to dyadic ambivalence is not inevitable. Its occurrence is determined by how partners respond to one another in these moments of disagreement.
Yovetich and Rusbult [45] offered a taxonomy of accommodation responses to dyadic ambivalence. They organized these around two dimensions capturing the extent to which the response is constructive (versus destructive) and active (versus passive). Voice and loyalty responses represent active and passive forms of constructive accommodation responses. A voice response occurs when partners achieve shared consensus through negotiation and effective communication is a key feature of this active accommodation response. Loyalty is also a constructive accommodation, but more passive as one partner will acquiesce to the other partner’s preferences for the shared good. In contrast, exit and neglect responses represent active and passive forms of destructive accommodation. An exit response occurs when apparent arguments may escalate into termination of the relationship. Neglect is also a destructive accommodation, but more passive as one partner will accept the other partner’s behavior to avoid conflict.
In separate but related work, Christiansen and colleagues have identified adaptive and maladaptive patterns of couples communication [46,47,48]. Whereas Yovetich and Rusbult’s taxonomy of accommodation responses are primarily behaviors displayed by one partner, Christiansen et al.’s patterns of communication involve dyadic exchanges between partners. They therefore provide a framework for conceptualizing how partners’ responses in times of dyadic ambivalence might follow one another sequentially in a conversational exchange. Examples of adaptive communication patterns are mutual discussion, mutual negotiation, and mutual expression. Examples of maladaptive communication patterns are mutual avoidance, mutual blame, and demand/withdraw. Mutual avoidance is an escape behavior characterized by both partners actively avoiding discussion of topics that would produce conflict. In contrast, mutual blame is characterized by partners’ assignment of fault or responsibility (i.e., blame) for a problem to one another during discussions of conflict. Demand/withdraw happens when one partner’s attempts to problem-solve are met with avoidance by the other partner.
The ability of partnered SMM to engage in constructive communication and adaptive accommodation responses will lead to communal coping and the development of joint HIV prevention goal formation [49, 50]. However, when SMM experience dyadic ambivalence, potential conflict, and the anticipation of maladaptive communication styles, they may be more hesitant to engage their partner in discussions around sexual risk reduction and need further communication skills to navigate responses in these conversations. One approach to communication training often integrated into brief MI interventions is video-based conversations about HIV prevention (e.g., HIV testing, sexual agreements, PrEP) [36, 51, 52]. The videos in all of these studies simultaneously demonstrate communication skills and also deliver information about HIV prevention practices relevant to partnered SMM. In this way, they have the potential to evoke motivation for prevention strategies, such as PrEP use, while also modeling communication skills that might help to enact these prevention strategies.
While the integration of communication skills training videos depicting HIV prevention conversations with male couples has shown some promise to facilitate behavior change [36], no research has yet examined how these integrated intervention components impact the dialogue between counselor and client after their use in session. This represents a missed opportunity to understand how these intervention components elicit motivation for change and also what barriers to change may be activated by viewing them. The goal of the current study was to explore client responses to video-based modeling of sexual health communication for PrEP administered in the context of an integrated MI intervention. Informed by Interdependence Theory, we approached the data with the specific intention of identifying how the presence of dyadic ambivalence would influence actual or anticipated conversations between participants and their relationship partners about PrEP. Furthermore, we sought to examine the implications of dyadic ambivalence about PrEP on relationship functioning, actual or anticipated accommodation responses evident in PrEP-related discussions characterized by dyadic ambivalence, and partners’ ability to support PrEP uptake and adherence as part of a shared HIV prevention strategy.
Methods
Participants and Procedures
Qualitative data were derived from intervention session recordings completed in person with partnered SMM. Sessions were conducted as part of Project PARTNER, a randomized control trial testing the efficacy of a 4-session MI intervention tailored for SMM in relationships [51]. All sessions analyzed were conducted between March 2018 and January 2020 before any study procedures were modified in response to the COVID-19 pandemic.
Participants were recruited through online advertising targeting SMM in the New York City metropolitan area on geo-social dating apps and social media platforms. SMM completed an online screening survey and were eligible to enroll in the trial if they met the following criteria: (1) 18–29 years of age or 30–34 if their partner is 18–29; (2) cisgender male; (3) have a main partner, for at least 1 month, who is male and aged 18 years or older; (4) HIV negative (confirmed by HIV rapid testing); (5) report drug use in the past 30 days; (6) condomless anal sex with casual partners or a non-monogamous primary partner (regardless of HIV status) or a sero-discordant primary partner (regardless of sexual agreement); (7) lived in the New York City metropolitan area; and (8) able to speak and read in English. If eligible, they were scheduled to complete an in-office baseline appointment, which began with a review of informed consent and included a Qualtrics survey assessment and biological testing. They were then randomized to either a 4-session MI intervention delivered by a counselor with advanced training in mental health counseling (Master’s degree, PhD, or doctoral student trainee) or a content and attention matched 4-session health education control condition. Participants received $50 for completing the baseline assessment and $20 for completion of each intervention session. All study procedures were approved by the CUNY University Integrated Institutional Review Board (CUNY-UI IRB).
Intervention Description
The current analysis focused on intervention content that emerged in session 3 after the client viewed a communication skills training video created for this study. The video is comprised of three scenes. Each scene depicts a SMM couple having a conversation about sexual health that involves PrEP. The scenes all follow the same pattern. Initially the couple makes a communication error. A narrator interrupts the scene to point out this error and suggest a more adaptive alternative communication strategy. The couple then continues the conversation implementing the suggested strategy culminating in a more successful conclusion.
-
Scene 1 depicts a couple with a non-monogamous agreement talking about how to handle HIV status disclosure with casual partners. They discuss the advantages PrEP might offer in reducing the need for these discussions.
-
Scene 2 depicts a couple who has recently completed a couples HIV testing session in which they agreed to be monogamous. The partners remain concerned about their ability to adhere to the agreement they have just created. They discuss the utility of PrEP for reducing risk and related anxiety about breaks in their agreement.
-
Scene 3 depicts a sero-discordant couple discussing HIV transmission risk in their relationship. They discuss PrEP as a tool to reduce the HIV positive partner’s primary concern about transmitting HIV to the negative partner. They also talk about PrEP as something that would reduce risk sufficiently to enable the HIV negative partner to take on the receptive role during sex.
During PARTNER session 3, the counselor showed the participants the communication skills training video. The video was followed by a debrief that reviewed two essential components of the video. The first component of the debrief focused on communication. The second focused on PrEP.
In the initial phase of the video debrief, the counselor focused on communication error and skill identification. The counselor asked the client to reflect on “what went wrong” in each scene and then “what the couple changed” in the second portion of each scene so that things went better. In instances where clients were unable to correctly label communication errors and skills, counselors provided this information. Clients were also invited to reflect on the communication challenges they experience in their own relationships. These were compared and contrasted with the couples in the video in order to identify opportunities for the client to implement skills in their interactions with their own partners.
In the second phase of the video debrief, counselors invited participants to reflect on the video with respect to PrEP. This section opened with a general question that elicited the client’s perspective on PrEP’s utility. For participants not on PrEP, the counselor then focused on examining the participant’s perspective on PrEP and enhancing motivation for PrEP uptake using MI skills. Participants who were on PrEP reflected on why they made the decision to utilize PrEP. Counselors also inquired about PrEP adherence and used MI skills to enhance motivation to sustain and adhere to PrEP. Consistent with the overall goal to address factors relevant for SMM in relationships specifically, this discussion of PrEP motivation specifically incorporated attention to the role relationship partners play in shaping decisions about PrEP.
Analytic Approach
Sessions were reviewed for content regarding motivating factors for PrEP uptake or sustainment. Such utterances, including those belonging to counselor, were transcribed verbatim and organized into a matrix using Microsoft Excel. Analysis of the data was conducted by first and second authors with oversight of the senior author of the authorship team. A combination of both inductive and deductive methods were used in order to derive the results presented—namely, a Framework Analysis and Consensual Qualitative Research (CQR) approach [53, 54]. Though seemingly antithetical analytic methods, a CQR approach provides initial steps that allow for systematic familiarization with data while a Framework Analysis ties the categories that emerge from the data to a theoretical framework using the language employed by the framework itself.
As the data transcribed had already comprised a broader domain encompassing PrEP and communication, each meaning unit (i.e., the transcribed utterance) was initially summarized succinctly in order to define the core idea of the utterance itself, emblematic of the second step of a CQR approach [53]. Once all core ideas were defined, the first and second authors met regularly to cross-analyze said core ideas and establish an initial set of apparent and broad categories. Categories were initially expansive in scope (e.g., Challenges in Communication Regarding PrEP Uptake) and were pared down to more granular sub-categories (e.g., One-sided Discussion). As a set of categories emerged, the authorship team identified the theoretical framework that may apply to contextualize the findings—the second step of a Framework Analysis that endeavors researchers to identify a framework of a priori issues or emergent themes [54].
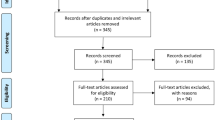
The apparent categories mapped on to established constructs belonging to Interdependence Theory, specifically: relationship functioning, accommodation, and the emergence (or lack thereof) of shared goals towards which partners directed joint effort [45, 55, 56]. Thus, all raw data related to the uptake or sustainment of PrEP were recoded and reorganized into a framework aligned with these constructs. The first and second authors individually recoded the raw data and met regularly to reach consensus on any discrepant codes. A total of 37 sessions were available for review. The team reviewed the first 30 sessions completed in order by date, by which point there were indications that they had obtained thematic saturation.
Results
Data were taken from the thirty-seven individuals who completed the PARTNER intervention session 3. There were no demographic differences between those participants randomized to intervention who completed (n = 37) and did not complete (n = 13) session 3. The average age was 26.65 years old. The majority of participants identified as White (62%), the second most represented group identified as Hispanic or Latino (24%). A minority of participants identified as Mixed Race or other (14%), of which one individual identified as Black and another race. Further, 81% identified as gay, 65% reported an annual income of $30,000 or more, and the majority of participants reported having earned a 4-year degree or more (86%).
The participant responses were coded and grouped into four themes: (1) PrEP related communication in the absence of dyadic ambivalence; (2) PrEP related communication in the presence of dyadic ambivalence; (3) Accommodation in PrEP discussions with primary partners: Responses to dyadic ambivalence; and (4) Representations of joint versus individual effort directed towards PrEP as an HIV prevention goal.
PrEP Related Communication in the Absence of Dyadic Ambivalence
In many instances, participants indicated little or no dyadic ambivalence regarding PrEP (i.e., differing opinions, goals, or expectations in respect to uptake). This theme was characterized by experience of alignment in partners’ attitudes about PrEP. Participants either experienced or anticipated that they and their partners had a mutually shared view of PrEP. Participants with and without an active PrEP prescription represented this theme. Among those with an active PrEP prescription, participants expressed that, historically, the discussion of PrEP was a perfunctory conversation, as shown in the session content below:
We literally met in the bar arguing about Truvada pricing. Like bam.
Like the first 10 min of conversation was: "Are you on PrEP? Great.
Do you have to pay anything for it? Great." (P110)
In other instances, participants referenced shared values—or a shared understanding of the importance of PrEP uptake—as guiding their discussion of beginning a regimen. The participant below, for example, disclosed that though his partner continued to prompt him to take up a regimen, the discussion regarding uptake was not premised on differing views of the benefits of PrEP, but rather his own lack of motivation to start PrEP.
He didn't have to convince me at all [to get on PrEP]. It was just like:
"You need to make sure you're getting on it. Are you on it?" Like, "are
you on a program? Are you looking for a program?" It was more like
me just dragging my feet about it, but there was never disagreement about
needing to get on it or its importance. (P127)
In some cases, participants who did not have active PrEP prescriptions expressed that they anticipated their partners would be receptive to a conversation about PrEP uptake. With these, participants indicated that they and their partners would mutually benefit from a regimen. Thus, some believed—such as the participant below—that the relative ease of such a discussion would be a function of having a mutual interest in a regimen.
I couldn't imagine arguing over it, we both get what we want
[by taking PrEP]. (P107)
Finally, participants sometimes expressed content consistent with this theme by explaining that their partners’ resistance to the prospect of PrEP would be wholly unexpected. In the session, such participants seemed to proffer hypothetical counter-arguments in the event that they may meet such resistance from their partner. The participant below compared PrEP uptake to that of other protective health behaviors that require minimal effort and were practiced by his partner—and as such, expected that his partner would be amenable to the notion of uptake.
Counselor: So if you were to have this conversation about being
open, it sounds like it would go well.
Participant: Yeah.
Counselor: You don't have any concerns.
Participant: No concerns whatsoever, I would be really surprised if he
said no [to being on PrEP]. I would be like: “You wear sunscreen everyday
and you wouldn't do this?” (P103)
PrEP Related Communication in the Presence of Dyadic Ambivalence—Implications for Relationship Functioning
In some instances, participants indicated relationship-related concerns served as a barrier to PrEP uptake. Responses in this category all suggested that PrEP use would, in some way, convey a negative message about how they felt towards their partner and the relationship overall. In other words, they implied some form of dyadic ambivalence. While participants may have had some level of personal receptivity to the idea of PrEP, they were concerned that PrEP would connote or represent something very different to their partner. These responses centered on three primary domains of relationship functioning: (1) implied infidelity, (2) implied exploration of relationship alternatives, and (3) implied commitment.
Implied Infidelity
Participants expressed concerns that broaching the subject of PrEP uptake would be seen by their main partner either as an admission of sex with casual partners or as an accusation that their partner was having sex with casual partners. The assumption was that PrEP would inherently convey concerns about trust or trustworthiness, as demonstrated below.
I think it would be suspicious. Like, “Oh, I'm back on PrEP, by
the way.” But like … why? (P103)
If [my partner] and I continued being monogamous it would be hard
to talk about PrEP. Other than saying, “this is in case we don't trust
each other.” (P112)
As indicated by these quotes, participants acknowledged that a conversation regarding PrEP uptake would include a simultaneous discussion about sexual agreement violations or sexual risk-taking concerns. By extension, such quotes likewise suggested how PrEP uptake may be met with dyadic ambivalence among couples who are explicitly monogamous and, thus, may perceive themselves to be at relatively low risk of HIV infection.
The idea that PrEP use conveys a message about relationship functioning was not restricted to men considering PrEP uptake. It was also observed in content from participants who were on PrEP. In this case, PrEP sustainment was considered an admission of ongoing sex with casual partners.
When we started dating I had been on PrEP because I had gone on it
a year before that. […] Kind of when we started dating and when it
moved into being monogamous I mentioned how would he feel if I
stayed on it, my perception was that he was a little uneasy with that.
He thought that if I were on it then I would clearly be having sex with
other people. (P114)
Responses like the one above illustrate the potential for concerns about partner perceptions to amplify ambivalence about PrEP. The participant perceives many benefits to PrEP. At the same time, he is also concerned because he anticipates his partner will see PrEP as a cause for concern. This phenomenon aligns with the concept of dyadic ambivalence. It represents an instance in which the participant believes he and his partner feel differently about PrEP use.
Implied Exploration of Relationship Alternatives
This idea that a discussion of PrEP had threatened—or held the potential to threaten–relationship functioning was not limited to participants in monogamous agreements. In some cases, participants in non-monogamous relationships disclosed that when they had introduced the notion of PrEP uptake, their partners believed that beginning such a regimen implied intention to explore alternatives to their primary relationship. Some participants specified that such exploration might take the form of engaging in CAS with casual partners (sexual practices considered reserved purely for their primary partners). The participant below described a discussion with his primary partner about PrEP uptake that simultaneously centered his partner’s concern regarding the intimacy shared with casual partners that PrEP might facilitate.
When I told my boyfriend I'm gonna start taking PrEP, his first
question was: “Are you going to start hooking up with other
people raw? Why are you taking it? Are you going to have unprotected
sex with other people, is that why you want to take it?” So that's why
I said: “No, I'm doing it because it's another layer of protection for
me. For myself. Not for you. Not because I want to have raw sex
with other people. It's something I need to do for myself.” (P122)
In the quote above, the participant’s partner was concerned that the participant’s PrEP use implied he was exploring alternatives to the relationship. In a complementary way, some participants conveyed the symmetrical concern that their partner’s use of PrEP would create the opportunity for their partner to engage in sexual behavior considered exclusive to the primary relationship (i.e., CAS).
Participant: If he wants to be on PrEP, I do find that a little bit threatening for some reason. I don't know exactly why.
Counselor: You mean outside of the health part.
Participant: I find it threatening that he would take PrEP, which is a
little bit fucked up.
Counselor: How so?
Participant: I do want to maintain some kind of control of whose
loads we're receiving […]. To have someone's bodily fluids sit in your
ass—that's very intimate. That's maybe something that I don't want to
share with other people. (P125)
Implied commitment. Participants also indicated that PrEP use or cessation was perceived as an indication of relationship commitment—or conversely that relationship commitment had direct implications for the ongoing relevance or utility of PrEP. These comments conveyed that either participants or their partners perceived PrEP use and cessation as a relationship milestone of sorts. In some instances, this idea that PrEP use connoted commitment emerged in the belief that discussions about PrEP cessation served as proxy conversation about commitment to the relationship.
It wasn't like—the conversation wasn't like, “I'm gonna stop taking
PrEP.” It was like “I didn't go in [for my medical appointment].”
And he was like, “Oh, I forgot mine as well.” And we're dating
now, so. (P103)
In other instances, the idea that PrEP use implies something about relationship commitment was manifest in the idea that bringing up the topic of PrEP, and considering whether or not PrEP was necessary in their relationship, needed to be situated in the larger context of relationship development. These concerns were less about the risk associated with the content of the conversation. They instead focused on the notion of timing. In some cases, participants were concerned that it was “too soon” or that the relationship was not ready for such a discussion.
Participant: […] It's kind of like the way things played out in such
an exponential way—like we started seeing each other and having sex
within 2 weeks and then he kind of cut things off and we went on a break.
And I definitely play a more passive role because I want him to lead in
terms of where it goes.
Counselor: You don't want to be overbearing and talking about PrEP
with him would be skipping some steps in a way.
Participant: Completely. (P111)
Existing research on adult SMM has largely focused on the idea that high levels of relationship commitment are a barrier to HIV prevention and lower levels of commitment have been associated with more HIV prevention. This idea of a communication double bind, in which both high and low levels of commitment experienced in established and early relationships respectively both serve as barriers to discussing HIV prevention.
Accommodation in PrEP Discussions with Primary Partners: Responses to Dyadic Ambivalence
In instances of dyadic ambivalence around PrEP, where participants experienced or anticipated that their partners would feel differently, they often went on to explain the nature of the communication exchange they thought would result if PrEP was discussed. As a result, these utterances included some indication of how the participant and their partner communicated in the face of this conflict. In some cases, this discussion of communication was a report of how communication had proceeded in the past. In others, it took the form of anticipated future communication. These responses centered on the four primary accommodation response domains identified by Yovetich and Rusbult [45]: (1) voice, (2) loyalty, (3) neglect, and (4) exit.
Voice. In some instances, participants commented that—although their partner would feel different—the conversation about PrEP was (or would be) constructive.
Participant: “We have actually had pretty open discussions about PrEP usage. [...] We ended up making a Google doc. [...] There was a time when my partner wasn't so sure that I am as committed to his sexual needs and interests and whether I am committed to doing PrEP. And I had the same argument that I don't really [have sex] outside [the relationship] anyway too much. But I am committed to what you need and that is what the Google doc came up with. Here is the document and here are the [chances] of two partners spreading [HIV], you choose.
Counselor: It was your way of saying you do care.
Participant: Like I did the research. (P119)
The participant’s description is consistent with a situation in which both he and his partner gave a voice accommodation response [56], one in which they constructively disclosed the rationale for their perspectives. At the dyadic level, this exchange may be understood as a mutual discussion whereby both partners voiced their concerns and proffered solutions when ambivalence emerged [46, 47].
Not all voice responses were met with success. In some instances, a participant’s attempt at a voice response was confronted with blame and accusations from their partner. These exchanges demonstrated the potential for an initial attempt at adaptive accommodation to devolve into mutual blame [46, 47]. In the exchange that follows, the participant initially disclosed his intention to go on PrEP as part of a mutual discussion and negotiation. Once PrEP emerged as a topic, partners began to express their perspectives via accusations of exploring alternatives to the relationship and emphasizing individual benefit of PrEP as opposed to benefit that may be shared by both partners.
For me, I told him I'm gonna start taking PrEP again. His first idea was,
“Are you gonna be bareback with other people?” And I was like, not
necessarily, but it's another layer of protection. Like I'm taking it because
I'm protecting myself. Because right now you can test positive for an
STD, but I don't want to get infected with HIV or something like that and
then give it to you. And I don't want it myself. Or what if you get infected
and then you give it to me? So, I was like, I'm doing it for myself. I'm not
doing it for you. I'm not doing it for our relationship. This is for me. Like
I feel more comfortable in an open relationship, or with anyone [when I take] PrEP. And he was like: “Okay! You made your point.” And that's how
we are. He doesn't take PrEP because he's lazy” (P122)
The juxtaposition of these examples—wherein sometimes voice accommodation responses lead to adaptive conversational exchanges and other times they set off conflict characterized by mutual blame—represents an opportunity for the counselor to integrate communication skills training. This might take the form of asking the participant to identify “what went wrong” and “what they might do differently next time” utilizing communication skills demonstrated in video-based models.
Loyalty
Participants also made disclosures that suggested that they had, at some point, acquiesced to their partner’s preferences with respect to PrEP. Consistent with the concept of a loyalty response, the concession here is made for pro-social reasons [57]. While the motivation arises from a desire to support the partner and the relationship as a whole, PrEP use is ultimately forgone.
[I stopped taking PrEP] because I was with [my partner] and we had a conversation and he was like, “I'm not on PrEP. And if we're serious
about this I guess I don't need to refill.” And I just didn't. (P103)
Although this participant’s loyalty-type accommodation response is considered constructive—because it ultimately preserves and enhances relationship quality in the long-term—it ultimately exposes him to some added level of risk because it inhibits his ability to work with his partner to reduce HIV infection risk. The communication pattern that plays out between the two men then could best be understood as a demand/withdrawal pattern [46, 47]. This dyadic pattern is understood as maladaptive generally and here it undercuts the couple’s ability to coordinate effort around prevention.
Not all loyalty responses are elicited by a partner’s demand. The participant below adopts a similarly passive response intended to preserve and enhance the relationship. The participant’s partner’s complementary response to avoid a discussion of HIV prevention results in a dyadic pattern of mutual avoidance.
Counselor: So I want to ask, how do you think you could clear the air
between you and your partner about PrEP? Because he's not one hundred
percent sold, it sounds like.
Participant: I don't know. I don't know if that is even something that
needs to be done because it's kind of on him to take care of himself.
I obviously want to take care of him as well, but I'm not about to tie him
down and force him. (P126)
Neglect. Avoidance was not always motivated by the desire to preserve or enhance the relationship. In some instances, participants described acquiescing to a partner’s preferences in order to avoid relationship conflict in the short term—even when doing so may harm the relationship in the long-term.
Participant: I'm fearful of losing him by bringing [PrEP] up […] I know
that in high school and college [my partner] wasn’t that promiscuous. So
I don’t know from moving to the city until now what his sexual encounters
have been like …
Counselor: So talking about PrEP with [your partner] doesn't fit in right
now because—
Participant: We don't even talk about our emotions. (P111)
Similar to the previous example, the participant utterance below demonstrates avoidance of a potential conflict in the short-term without regard for the long-term implications of that avoidance for overall relationship quality.
I did plan on being monogamous and not cheating on him. One of the
times that I did, I used a condom so I was safe. But I just didn't want to
have to have that conversation with him. If we were going to have an open relationship or continue to sleep with people then I would've stayed on
[PrEP]. But I got the sense that he was uneasy or confused that I would
stay on it. (P114)
Both loyalty and neglect accommodation responses illustrate the potential for counselors to engage in communication skills training. The counselor might explore how these responses characterized by avoidance of HIV prevention discussions enhance risk in the relationship—generating motivation for communication with partners. Subsequently, the counselor might work with the client to identify and practice skills that could be used to initiate and navigate these conversations.
Exit
In some instances, considering discussions of PrEP led participants to discuss the prospect of relationship dissolution with their counselors. In some instances, participants indicated they would consider dissolving their relationship should their partner wish to abstain from a regimen or when they could not communicate about PrEP with their partner. These utterances indicated an exit response–willingness to leave the relationship entirely in the face of conflict around PrEP. Notably, those participants who expressed utterances indicative of an exit response all did so in the context of wanting to take PrEP and contending with their partner preferring to abstain.
If he were to say no [to being on PrEP if in the case of an open
relationship], I would agree to being open and think about whether
I would want to be with [my partner]. That safety is really important.
I would want to be aligned and have ground rules of being open. (P103)
Part of the reason that I want to end the relationship with my boyfriend
is because I want to find someone who I am able to have that conversation
with [about PrEP]. (P116)
Exit responses also demonstrate an opportunity to extend communication skill building in session. These utterances all indicate a clear desire to go on PrEP. Counselors have the opportunity not only to harness that motivation for risk reduction, but also to explore ways that the client might approach their partner in conversation successfully. Introducing the topic of PrEP as an ultimatum or accusation is more likely to elicit a complementary response of defensiveness and blaming from a partner. In contrast, opening an exchange with a non-judgmental explanation for the importance of PrEP might elicit a mutual and constructive discussion between partners.
Representations of Joint Versus Individual Effort Directed Towards PrEP as an HIV Prevention Goal
Finally, participants often described the effort involved in acquiring or adhering to a PrEP regimen. These discussions generally characterized these efforts in one of two ways. In some instances, participants described PrEP uptake and adherence in terms of joint effort and integrated a description of the role their partner played in the decision. In other instances, participants described PrEP uptake and adherence in terms of their individual effort—providing relatively little mention of their partner’s support for PrEP.
Joint Effort
Some participants expressed that they have or would work together with their partners to get on PrEP. In virtually all instances, these utterances implied that partners had arrived at a shared vision for HIV prevention and the role of PrEP as a prevention strategy. In other words, utterances that indicated couples’ capacity for joint effort were often characterized by the absence—or prior resolution—of dyadic ambivalence.
Counselor: You mentioned he was the one who kind of got you on
PrEP to begin with.
Participant: He was the one who kept yelling at me: “You need to be
on it! You need to be on it!” And I knew I did, but I didn't have insurance
so it was several steps to get on it. And so I finally did. But I wouldn't
have done it as soon as I did if he hadn't been harping on me about it. (P127)
Session content also included disclosures of joint effort pertaining to PrEP adherence and sustainment. Similar to the previous quote, the following participants described how they and their partner coordinate reminders to take their daily dose of PrEP or refill their respective prescriptions.
Yesterday [my partner] actually reminded me. He was like, “I just got
my new PrEP prescription, did you refill yours?” And I was like, “No!” I
guess it's a whole kind of checking in thing. But it's not formalized at all,
just if you're thinking about it. (P110)
I think our PrEP use is very much in each other's minds because I take it right before we go to bed, so when I'm over at his house three nights in a row he sees it. And he takes it every morning. So it's a very visible thing between us. We've definitely talked about it multiple times, but it's never been something that we question. (P129)
In both instances, these quotes are highly consistent with the concept of communal coping [50]. They illustrate the benefits associated with joint goal formation and the role partners can play in supporting health behavior when they are invested in one another’s outcomes.
Individual Effort
In contrast, participants in some cases regarded PrEP uptake as a uniquely individual concern. These instances were in some way characterized by dyadic ambivalence. Partners were unable to arrive at a shared or mutual HIV prevention plan and therefore the individual partners either proceeded with PrEP independently—or not—without one another’s support. In some instances, the session content indicated that participants and their partners had relatively limited knowledge of one another’s behavior. Their lack of engagement and support for one another translated to a vague or indirect awareness of exactly which steps were being taken to prevent HIV.
Counselor: You are on PrEP.
Participant: Yes.
Counselor: And [your partner] is trying to get on it, if I remember
correctly.
Participant: He started new insurance now […] my understanding is
he is going to get on it soon. We haven't talked about it. (P115)
Participants sometimes also described PrEP sustainment in terms of individual effort. In so doing, they often described differing appraisals of the threat of HIV. The participant below, for example, illustrated that he and his partner had divergent perceptions of HIV risk that informed their respective adherence to PrEP.
Participant: [My partner is] way more diligent [about PrEP adherence]
than I am because he's hella anxious.
Counselor: Like if he misses a dose—
Participant: He freaks out.
Counselor: And if you do—
Participant: It's like—I'll take it when I get home. Like if I miss a
dose, it's not the end of the world. Even if I get HIV, it's not the end
of the world. (P113)
In both instances, these quotes illustrate that the absence of a joint goal diminishes partners’ capacity to support one another’s health behavior. These participants who viewed PrEP as an individual health behavior had limited knowledge of their partner’s behavior and a diminished sense of the degree to which their partner’s behavior was relevant to their own level of risk (and vice versa). As a result, the degree of HIV risk experienced by one or both partners is increased.
Discussion
These findings represent the first examination of content from one component of an individually delivered MI intervention tailored for SMM in relationships. At the broadest level, the session content analyzed provides evidence that an intervention that engages only one partner in the relationship can elicit detailed content about how partner interactions shape the respondent’s health-related behavior. Consistent with Interdependence Theory, these analyses provide evidence that dyadic ambivalence (i.e., wherein partners’ priorities or perceptions are incongruent) generate a number of relational barriers to PrEP uptake, adherence, and sustainment. These include concerns about the implications of PrEP for relationship functioning and the precipitation of conflict in PrEP related discussions. When constructive accommodation responses and adaptive communication were anticipated, participants identified the potential for joint effort to promote PrEP use. In contrast, the anticipation of conflict or destructive accommodation in response dyadic ambivalence diminished joint effort for PrEP.
Consistent with this, when participants believed their partners shared their perspective on PrEP, they anticipated few challenges in communicating with about PrEP. Participants in these cases either described previous conversations around PrEP with their partner or suggested hypothetical conversations with limited tension. In addition, representations of joint effort—or narratives that described actual partner support or suggested participants believed their partner would be supportive of PrEP uptake and sustainment—were characterized by the absence (or successful resolution) of dyadic ambivalence. When both a participant and their partner are inclined towards PrEP uptake and adherence, the primary value of communication skills training may be to activate and access partner support within the context of planning for how to enact change (e.g., obtain PrEP) or maintain current health behavior practice (e.g., ongoing support for adherence).
Meanwhile, participants sometimes described instances of dyadic ambivalence and anticipated several challenges in communicating with their partners about PrEP. For participants who believed that their partners did not share their perspective on PrEP, the topic activated a number of relationship-related concerns. They worried that using PrEP, or raising the possibility in discussion, would signal the desire to have sex with other people, exploring other relationship options, or experiencing diminished levels of commitment to the relationship. In the presence of dyadic ambivalence and considering such potential conflict, participants described anticipated exchanges with their partner that represented the range of accommodation responses proposed by Rusbult et al. [45].
These distinctions provide important information to an MI counselor. Participants who anticipate Voice-type interactions, which involve the assertive and constructive exchange of priorities and perspectives, may need relatively little communication skills training. Instead, counselors might productively focus on eliciting motivation for these participants to engage in PrEP-related discussions with their partner. Participants who anticipate maladaptive interactions (e.g., mutual blame, demand/withdraw responses) if they broach the subject of PrEP, which may include accusatory language, may require additional communication skills training [51]. These participants may benefit more from a discussion of relevant communication skills and strategies for responding adaptively to a partner’s accusations or complaints or to limit their own accommodation responses that tend to be passive and withdrawn. In other words, in addition to eliciting motivation to engage partners in a discussion of PrEP, participants who anticipate maladaptive accommodation responses may need added support to develop the skills required to navigate these conversations successfully.
In some respects, findings that relationship concerns (perceptions of infidelity, exploration of relationship alternatives, or limited commitment) diminish motivation for PrEP replicate previous findings from earlier qualitative studies [19, 20, 33]. This analysis yielded indications that relationship concerns may diminish PrEP uptake among SMM in non-monogamous relationships in two ways not previously documented. First, while “infidelity” or the mere occurrence of sex with a casual partner was less of a concern, some non-monogamous SMM indicated that PrEP use may signal a desire to have CAS with casual partners, an activity that some men in non-monogamous men preferred to restrict to the primary partnership. Second, some SMM in non-monogamous relationships indicated that PrEP could signal a desire to explore relationship alternatives. These concerns can be understood in terms of the concept of relationship maintenance in Interdependence Theory [58]. Rusbult et al. [44] suggested that as commitment increases, partners are motivated to engage in behaviors that serve to ensure the durability of the relationship. These include discounting the value of relationship alternatives. For at least some non-monogamous men, the use of PrEP may signal a threat to the “special status” of the main partnership and raise concerns that outside partners may representative alternatives that could encroach on the integrity of the primary partnership.
These findings broadly align with the premise that cultivating couples’ capacity for joint effort can improve health behavior [45, 55, 56]. While there are challenges inherent in supporting SMM engaging their relationship partners in HIV-prevention decision making, there are also potential opportunities to expand the efficacy of prevention for this high-risk group. When partners are aligned on a goal, their efforts at social control—or the regulation of one another’s health behavior—are more likely to be positive versus negative and experienced as supportive versus aversive [44, 50]. Consistent with this, SMM who engage in communication to establish common goals for sexual agreements and discuss PrEP uptake or adherence are more likely to reduce HIV sexual transmission risk for themselves and their partner. Conversely, those who are unable to communicate with their partner to establish common goals may pursue individual effort for PrEP uptake or adherence, potentially resulting in a disjointed alignment of HIV prevention goals between partners. Partners may become less concerned with their partner’s health and vice versa. This results in more negative instances for social control and a decreased ability for SMM to regulate their partner’s behavior, which increases HIV risk for the couple. This supports the inclusion of addressing dyadic ambivalence and joint goal formation into MI interventions to establish more clearly defined HIV prevention goals for SMM and their partners.
Implications for the Development of Individual MI Interventions Tailored for SMM in Relationships
These findings provide preliminary indications that an individually delivered MI intervention has the ability to elicit content that is relevant for SMM in relationships. Most existing interventions that address sexual risk reduction in ways tailored for SMM in relationships are dyadic (e.g., [34, 36, 59, 60]) and involve both partners participating to establish sexual agreements and other joint goals for HIV prevention. Not all SMM in relationships are able to participate in a dyadic intervention with their partner because of competing schedules or a lack of interest in recruiting their partner in relationships characterized by less satisfaction [42, 51]. Conversely, most individual interventions for SMM do not address relationship factors and mostly support individual effort for HIV prevention. These findings support the ability for an individual MI intervention to address relationship factors by eliciting content relevant to interactions between partners. This allows for further exploration of potential dyadic ambivalence and the factors that motivate SMM to discuss PrEP uptake or adherence with their partner.
In addition, these results illustrate the potential utility of integrating communication skills training into individually delivered MI interventions tailored for SMM in relationships. While MI assists in exploring dyadic ambivalence and builds motivation for behavior change, communication skills training provides guidance for SMM to communicate with their partner in a non-judgmental way to encourage and promote constructive discussions between partners, which can improve relationship functioning [61]. Thus, integrating communication skills training and other cognitive behavioral training into MI may strengthen the overall impact of an intervention for HIV prevention among SMM [37, 51, 62]. Counselors can incorporate these strategies to build motivation to continue conversations regarding PrEP and other HIV prevention strategies. In instances where potential conflict may exist in the relationship, the counselor has the potential to follow the descriptions of these conversation exchanges with an examination of what went wrong and what could go better next time. Communication skills training can build confidence in SMM who want to start or maintain PrEP but have difficulty communicating when discussions bring up defensiveness and blame from their partner.
Finally, these results have implications for other single session interventions, such as HIV testing counseling and PrEP navigation. These interventions would benefit from probing client’s relationship status and the extent to which relationship considerations present a barrier (or support) for HIV prevention and PrEP uptake. To facilitate rapport building, counselors can ask clients to tell them about their relationship and discuss how they and their partner currently manage HIV risk in their relationship. The conversation can also include a discussion of the couple’s sexual agreement. Fortunately, such a discussion should fit well within the existing skill set of most HIV testing and PrEP navigation providers. This can be accomplished in 5 to 10 min of the session through a brief series of open questions followed by reflections of client’s response. Providers can also ask clients to reflect on how their partners’ perceive HIV prevention or PrEP uptake and the impact those perceptions have on their decisions. The use of video-based communication skill building has the potential to enhance the portability of this activity to these single session intervention applications. The videos provide standardized models of couples engaging in sexual health discussions. HIV prevention planning or PrEP linkage plans might then incorporate strategies for communicating with partners in ways that maximize partner support and minimize the potential for relationship conflict or partner interference with prevention implementation. These components of the intervention follow a protocol that could be delivered readily by anyone with knowledge of sexual health care services. This minimizes the need for counselors to have specialized training in cognitive behavioral or social problem solving skills techniques. It therefore presents one possible way to enhance existing single session services by incorporating components that address primary relationships without substantially enhancing provider skill demands.
Limitations
Several limitations should be considered in the context of our results. First, all data was obtained from intervention session content and not from a structured interview on relationships and PrEP. While results are extrapolated in context of an intervention session, the content of the couple and their actual or hypothetical PrEP conversations are more applicable to addressing barriers in MI counseling practice. Second, this sample includes all SMM who are in a non-monogamous relationship and report drug use. Their ability to engage in PrEP discussions with their partner may be more challenging then SMM in monogamous relationships or who are not actively using drugs. Third, the intervention was conducted in New York City where PrEP is easily accessible and conversations between partners regarding PrEP uptake or adherence may include additional accessibility challenges if conducted in other locations. Fourth, our analytic sample of individuals who completed session 3 only had one participant who identified as Black and another race. Cross examination of racial and ethnic identity suggested that all themes were manifest in content of at least two different racial and ethnic groups. We acknowledge the lower percentage of Black participants who completed this session and suggest future communication research should include greater representation of all racial and ethnic groups. Finally, the sample is made up of emerging adults who may be experiencing additional communication challenges.
Conclusion
Partners may actively encourage and discourage each other to initiate, sustain, or stop PrEP [26], presenting unique challenges and catalysts for prevention. Understanding the relationship factors influencing PrEP initiation and adherence is imperative. Discussions around PrEP can be challenging for SMM in relationships due to potential sources of conflict arising from PrEP being associated with diminished relationship functioning. Individual MI interventions for partnered SMM are feasible and benefit SMM in relationships by addressing dyadic ambivalence regarding PrEP and including communication skills building around PrEP to empower clients to discuss sexual health goals with partners.
Data Availability
Data not publicly available. Please contact the corresponding author.
Code Availability
Descriptive statistics were analyzed using SPSS version 27.
References
Pitasi MA, Beer L, Cha S, Lyons SJ, Hernandez AL, Prejean J, et al. Vital signs: HIV infection, diagnosis, treatment, and prevention among gay, bisexual, and other men who have sex with men—United States, 2010–2019. Morb Mortal Wkly Rep. 2021;70(48):1669.
CDC. Diagnoses of HIV infection in the United States and Dependent Areas, 2019 2021 https://www.cdc.gov/hiv/library/reports/hiv-surveillance/vol-32/index.html.
CDC. HIV Transmission 2019 https://www.cdc.gov/hiv/basics/transmission.html.
Sullivan PS, Salazar L, Buchbinder S, Sanchez TH. Estimating the proportion of HIV transmissions from main sex partners among men who have sex with men in five US cities. AIDS. 2009;23(9):1153–62.
Goodreau SM, Carnegie NB, Vittinghoff E, Lama JR, Sanchez J, Grinsztejn B, et al. What drives the US and Peruvian HIV epidemics in men who have sex with men (MSM)? PLoS ONE. 2012;7(11): e50522.
Starks TJ, Jones SS, Kyre K, Robles G, Cain D, Jimenez R, et al. Testing the drug use and condomless anal sex link among sexual minority men: the predictive utility of marijuana and interactions with relationship status. Drug Alcohol Depend. 2020;216: 108318.
Starks TJ, Robles G, Bosco SC, Dellucci TV, Grov C, Parsons JT. The prevalence and correlates of sexual arrangements in a national cohort of HIV-negative gay and bisexual men in the United States. Arch Sex Behav. 2019;48(1):369–82.
Buchbinder SP, Glidden DV, Liu AY, McMahan V, Guanira JV, Mayer KH, et al. HIV pre-exposure prophylaxis in men who have sex with men and transgender women: a secondary analysis of a phase 3 randomised controlled efficacy trial. Lancet Infect Dis. 2014;14(6):468–75.
Anderson PL, Glidden DV, Liu A, Buchbinder S, Lama JR, Guanira JV, et al. Emtricitabine-tenofovir concentrations and pre-exposure prophylaxis efficacy in men who have sex with men. Sci Transl Med. 2012;4(151):151ra25.
Grant RM, Lama JR, Anderson PL, McMahan V, Liu AY, Vargas L, et al. Preexposure chemoprophylaxis for HIV prevention in men who have sex with men. N Engl J Med. 2010;363(27):2587–99.
Molina J-M, Charreau I, Spire B, Cotte L, Chas J, Capitant C, et al. Efficacy, safety, and effect on sexual behaviour of on-demand pre-exposure prophylaxis for HIV in men who have sex with men: an observational cohort study. Lancet HIV. 2017;4(9):e402–10.
CDC. Prexposure Prohphylaxis for the prevention of HIV infection in the United States- 2017 Update. Atlanta, GA: CDC; 2018.
Halkitis PN, Jaiswal J, Griffin-Tomas M, Krause KD, D’Avanzo P, Kapadia F. Beliefs about the end of AIDS, concerns about PrEP functionality, and perceptions of HIV risk as drivers of PrEP use in urban sexual minority men: the P18 cohort study. AIDS Behav. 2018;22(11):3705–17.
Sullivan MC, Eaton LA. Intersecting barriers to PrEP awareness and uptake in black men who have sex with men in Atlanta, GA: a syndemic perspective. Int J Behav Med. 2020;28:1–11.
Edeza A, Karina Santamaria E, Valente PK, Gomez A, Ogunbajo A, Biello K. Experienced barriers to adherence to pre-exposure prophylaxis for HIV prevention among MSM: a systematic review and meta-ethnography of qualitative studies. AIDS Care. 2020;33:1–9.
Robles G, Hong C, Yu M, Starks TJ. Intersecting communities and PrEP uptake among US-based Latinx sexual minority men. J Racial Ethnic Health Disparities. 2021;9:1–7.
Stephenson R, Chavanduka T, Sullivan SP, Mitchell JW. Dyadic influences on pre-exposure prophylaxis (PrEP) use and attitudes among male couples. AIDS Behav. 2021;26:1–14.
Gamarel KE, Golub SA. Sexual goals and perceptions of goal congruence in individuals’ PrEP adoption decisions: a mixed-methods study of gay and bisexual men who are in primary relationships. Ann Behav Med. 2020;54(4):237–48.
Starks TJ, Doyle KM, Shalhav O, John SA, Parsons JT. An examination of gay couples’ motivations to use (or forego) pre-exposure prophylaxis expressed during couples HIV testing and counseling (CHTC) sessions. Prev Sci. 2019;20(1):157–67.
Bosco SC, Pawson M, Parsons JT, Starks TJ. Biomedical HIV prevention among gay male couples: a qualitative study of motivations and concerns. J Homosex. 2019;68:1–18.
John SA, Robles G, Starks TJ, Rendina HJ. Differences between groups of pre-exposure prophylaxis (PrEP) using couples in HIV-negative/unknown relationships. JAIDS J Acquir Immune Defic Syndr. 2019;81(4):419–28.
Ware NC, Wyatt MA, Haberer JE, Baeten JM, Kintu A, Psaros C, et al. What’s love got to do with it? Explaining adherence to oral antiretroviral pre-exposure prophylaxis for HIV-serodiscordant couples. J Acquir Immune Defic Syndr. 2012;59(5):463–8.
Stephenson R, White D, Mitchell JW. Sexual agreements and perception of HIV prevalence among an online sample of partnered men who have sex with men. Arch Sex Behav. 2015;44(7):1813–9.
Mitchell JW, Petroll AE. HIV testing rates and factors associated with recent HIV testing among male couples. Sex Transm Dis. 2012;39(5):379.
Walsh JL, John SA, Robles G, Wesche R, Hirshfield S. Talking to my partners about PrEP: factors associated with PrEP-related communication in a longitudinal US study of sexual minority men living with HIV. Prev Sci. 2022. https://doi.org/10.1007/s11121-022-01372-6.
John SA, Starks TJ, Rendina HJ, Grov C, Parsons JT. Should I convince my partner to go on pre-exposure prophylaxis (PrEP)? The role of personal and relationship factors on PrEP-related social control among gay and bisexual men. AIDS Behav. 2018;22(4):1239–52.
Braithwaite S, Holt-Lunstad J. Romantic relationships and mental health. Curr Opin Psychol. 2017;13:120–5.
Robles TF, Slatcher RB, Trombello JM, McGinn MM. Marital quality and health: a meta-analytic review. Psychol Bull. 2014;140(1):140.
Loving TJ, Slatcher RB. Romantic relationships and health. 2013.
Dunkel SC. Moving research on health and close relationships forward—a challenge and an obligation: introduction to the special issue. Am Psychol. 2017;72(6):511.
Starks TJ, Doyle KM, Millar BM, Parsons JT. Eriksonian intimacy development, relationship satisfaction, and depression in gay male couples. Psychol Sex Orientat Gend Divers. 2017;4(2):241.
Starks TJ, Pawson M, Stephenson R, Sullivan P, Parsons JT. Dyadic qualitative analysis of condom use scripts among emerging adult gay male couples. J Sex Marital Ther. 2018;44(3):269–80.
Quinn KG, Zarwell M, John SA, Christenson E, Walsh JL. Perceptions of PrEP use within primary relationships among young black gay, bisexual, and other men who have sex with men. Arch Sex Behav. 2020;49(6):2117–28.
Sullivan PS, White D, Rosenberg ES, Barnes J, Jones J, Dasgupta S, et al. Safety and acceptability of couples HIV testing and counseling for US men who have sex with men: a randomized prevention study. J Int Assoc Provid AIDS Care (JIAPAC). 2014;13(2):135–44.
Starks TJ, Adebayo T, Kyre KD, Millar BM, Stratton MJ, Gandhi M, et al. Pilot randomized controlled trial of motivational interviewing with sexual minority male couples to reduce drug use and sexual risk: the couples health project. AIDS Behav. 2021;26:1–18.
Starks TJ, Dellucci TV, Gupta S, Robles G, Stephenson R, et al. A pilot randomized trial of intervention components addressing drug use in couples HIV testing and counseling (CHTC) with male couples. AIDS Behav. 2019;23(9):2407–20.
Starks TJ. Couples motivational interviewing: a framework for behavior change developed with sexual minority men. Oxford: Oxford University Press; 2022.
Wu E, El-Bassel N, McVinney LD, Hess L, Remien RH, Charania M, et al. Feasibility and promise of a couple-based HIV/STI preventive intervention for methamphetamine-using, black men who have sex with men. AIDS Behav. 2011;15(8):1745.
Newcomb ME, Macapagal KR, Feinstein BA, Bettin E, Swann G, Whitton SW. Integrating HIV prevention and relationship education for young same-sex male couples: a pilot trial of the 2GETHER intervention. AIDS Behav. 2017;21(8):2464–78.
Stephenson R, Sullivan SP, Mitchell JW, Johnson BA, Sullvian PS. Efficacy of a telehealth delivered couples’ HIV counseling and testing (CHTC) intervention to improve formation and adherence to safer sexual agreements among male couples in the US: results from a randomized control trial. AIDS Behav. 2022. https://doi.org/10.2139/ssrn.3893541.
Starks TJ, Robles G, Doyle KM, Pawson M, Bertone P, Millar BM, et al. Motivational interviewing with male couples to reduce substance use and HIV risk: Manifestations of partner discord and strategies for facilitating dyadic functioning. Psychotherapy. 2020;57:58–67.
Starks TJ, Millar B, Parsons JT. Correlates of individual versus joint participation in online survey research with same-sex male couples. AIDS Behav. 2015;19:963–9.
Kelley HH, Thibaut TW. Interpersonal relations: a theory of interdependence. New York: Wiley; 1978.
Rusbult CE. Commitment and satisfaction in romantic associations: a test of the investment model. J Exp Soc Psychol. 1980;16(2):172–86.
Yovetich NA, Rusbult CE. Accommodative behavior in close relationships: exploring transformation of motivation. J Exp Soc Psychol. 1994;30(2):138–64.
Christensen A. Detection of conflict patterns in couples. 1987.
Christensen A. Dysfunctional interaction patterns in couples. 1988.
Sullaway M, Christensen A. Assessment of dysfunctional interaction patterns in couples. J Marriage Family. 1983;45:653–60.
Albarracín D, Gillette JC, Earl AN, Glasman LR, Durantini MR, Ho M-H. A test of major assumptions about behavior change: a comprehensive look at the effects of passive and active HIV-prevention interventions since the beginning of the epidemic. Psychol Bull. 2005;131(6):856.
Lewis MA, McBride CM, Pollak KI, Puleo E, Butterfield RM, Emmons KM. Understanding health behavior change among couples: an interdependence and communal coping approach. Soc Sci Med. 2006;62(6):1369–80.
Starks TJ, Robles G, Pawson M, Jimenez RH, Gandhi M, Parsons JT, et al. Motivational interviewing to reduce drug use and HIV incidence among young men who have sex with men in relationships and are high priority for pre-exposure prophylaxis (Project PARTNER): randomized controlled trial protocol. JMIR Res Protoc. 2019;8(7): e13015.
Starks TJ, Feldstein Ewing SW, Lovejoy T, Gurung S, Cain D, Fan CA, et al. Adolescent male couples-based HIV testing intervention (we test): protocol for a type 1, hybrid implementation-effectiveness trial. JMIR Res Protoc. 2019;8(6): e11186.
Hill CE. Consensual qualitative research: a practical resource for investigating social science phenomena. Washington: American Psychological Association; 2012.
Ritchie J, Spencer L. Qualitative data analysis for applied policy research. London: Routledge; 2002. p. 187–208.
Rusbult CE, Van Lange PA. Interdependence, interaction, and relationships. Annu Rev Psychol. 2003;54:351–75.
Rusbult CE, Zembrodt IM, Gunn LK. Exit, voice, loyalty, and neglect: responses to dissatisfaction in romantic involvements. J Pers Soc Psychol. 1982;43(6):1230.
Rusbult CE, Zembrodt IM. Responses to dissatisfaction in romantic involvements: a multidimensional scaling analysis. J Exp Soc Psychol. 1983;19(3):274–93.
Rusbult CE, Olsen N, Davis JL, Hannon PA. Commitment and relationship maintenance mechanisms. London: Psychology Press; 2001. p. 95–122.
Stephenson R, Freeland R, Sullivan SP, Riley E, Johnson BA, Mitchell J, et al. Home-based HIV testing and counseling for male couples (Project Nexus): a protocol for a randomized controlled trial. JMIR Res Protoc. 2017;6(5): e101.
Gamarel KE, Darbes LA, Hightow-Weidman L, Sullivan P, Stephenson R. The development and testing of a relationship skills intervention to improve HIV prevention uptake among young gay, bisexual, and other men who have sex with men and their primary partners (we prevent): protocol for a randomized controlled trial. JMIR Res Protoc. 2019;8(1): e10370.
Baucom KJ, Baucom BR, Christensen A. Changes in dyadic communication during and after integrative and traditional behavioral couple therapy. Behav Res Ther. 2015;65:18–28.
Naar S, Safren SA. Motivational interviewing and CBT: combining strategies for maximum effectiveness. New York: Guilford Publications; 2017.
Acknowledgements
The authors acknowledge the contributions of Christine Cowles, Beeta Salsabilian, Joseph Hillesheim, Kory Kyre, Mark Pawson, Michael Suarez, Nahual Smith Becerra, Jonathan O’Hadi, Cynthia Cabral, Paula Bertone, Gabriel Robles Alberto, Thomas Whitfield, Laurel Weaver, Sugandha Gupta, as well as our recruitment and data management teams.
Funding
This study was funded by a grant from the National Institute on Drug Abuse (NIDA) (R01DA045613;PI Starks).
Author information
Authors and Affiliations
Contributions
DC was primarily responsible for development and execution of the analytic plan, coded the data, drafting text, and manuscript submission. DS contributed to the analytic plan, coded the data, and drafted the results section. TJS was primarily responsible for development of the intervention, study execution and oversight, development of the analytic plan, drafting text, and feedback on the manuscript overall. All authors reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
No conflict of interest declared.
Ethical Approval
The study was approved by the City University of New York Integrated Institutional Review Board (CUNY-UI IRB).
Consent to Participate
All participants were provided written informed consent information, and this was reviewed verbally prior to the start of the study.
Consent for Publication
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Cain, D., Sauermilch, D. & Starks, T.J. Client Responses to Video-Based Communication Skills Training Involving PrEP for HIV: Tailoring an Individual Sexual Health Intervention for Sexual Minority Men in Relationships. AIDS Behav 27, 2463–2477 (2023). https://doi.org/10.1007/s10461-023-03985-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-023-03985-6