
Abstract
Among people living with HIV/AIDS (PLHA), the occurrence of post-traumatic stress disorder (PTSD) symptoms associated with HIV diagnosis is a common problem. This study examined HIV diagnosis-related PTSD symptoms and its associated factors among PLHA in rural China. We used baseline data from a randomized controlled trial conducted in Anhui Province, China. Surveys of 522 PLHA were conducted via computer-assisted personal interview method. PTSD symptoms were measured based on re-experiencing, avoidance and arousal of the day of HIV diagnosis. Association between PTSD symptoms and demographic characteristics, physical and social functioning were assessed by multiple regression analysis and structural equation modeling. Social functioning exhibited a direct association with HIV diagnosis-related PTSD symptoms, and also mediated the association between PTSD symptoms and age, family income, and physical functioning. The study findings underscore the importance of developing interventions that alleviate PTSD symptoms and improve social functioning among PLHA in rural China.
Similar content being viewed by others


Introduction
There is growing awareness that symptoms of post-traumatic stress disorder (PTSD) are among the most common mental challenges for people living with HIV/AIDS (PLHA) around the world [1]. In 2015, there were approximately 36.9 million PLHA worldwide [2]. Although the prevalence of PTSD among PLHA varies across studies, ranging from 10 to 74% [3–8], these numbers are all much higher than those reported for the general population [1, 9, 10]. Moreover, a significant number of PLHA, although do not meet the diagnostic standard for PTSD, demonstrated symptoms associated with PTSD [11].
Prior studies have indicated that PLHA develop PTSD symptoms mainly due to being diagnosed with a life-threatening disease [4], progression of the disease [7, 12], social stigma and deterioration in quality of life [13–15]. In addition, PLHA are more likely than other individuals to experience other traumatic events, such as physical violence and sexual assault, which place them at risk of developing PTSD [3, 16]. Moreover, the presence of mental health problems such as PTSD symptoms may lead to the faster progression of HIV infection, worse physical problems, social phobia, and poor adherence to medication [1, 11, 17–20].
By the end of 2014, there were 501,000 reported HIV/AIDS cases in China [21]. The HIV epidemic in the country has overall maintained a low-prevalence trend, with a national prevalence of HIV less than 0.1%; however, the prevalence is high in some areas and among certain groups, such as injection drug users (IDUs; 6.0%) and men who have sex with men (MSM; 7.7%) [21]. Since the first case was identified in 1985, China has witnessed a tremendous and unique change of the major transmission modes of HIV: from 1985 to 2005, about 44% of newly diagnosed cases of HIV/AIDS happened in IDUs in border areas, while about 30% happened in plasma donors in central farmland of China; the virus has been then spread dramatically in both rural and urban areas through sexual transmission, with sexually transmitted cases accounting for 92% of all newly diagnosed cases in 2014 [21–24].
In China, the prevalence of PTSD among the general population is approximately 0.3% [25]. However, few studies have reported the prevalence of PTSD and its associated factors among PLHA in China. Previous HIV-related PTSD studies were mostly conducted among certain populations (e.g. MSM and heterosexual women) in western countries and Africa [3–7]. These studies have limited ability to generalize the findings to PLHA in rural China, where a sizable proportion of HIV-positive individuals were infected with HIV via infusion of contaminated blood products during paid plasma donation in 1990s [26], and where the social-economic status and the access to healthcare resources are relatively low. In this study, we primarily sought to assess levels of HIV diagnosis-related PTSD symptoms in a sample of PLHA in rural China. We also focused on investigating the association between PTSD symptoms and demographic characteristics, physical and social functioning in this population.
Methods
Participant Recruitment and Data Collection
This study used baseline data from a randomized controlled intervention trial for HIV-affected families in rural areas of Anhui Province, China; in this region, the majority of existing HIV infections were contracted via plasma donation [26]. Baseline assessments were performed from late 2011 to early 2013. We selected 32 villages from four counties in Anhui Province as study sites based on numbers of HIV-affected families. For PLHA, the inclusion criteria were (1) at least 18 years of age; (2) being a resident of the selected village; and (3) having a child between 6 and 18 years of age in his/her family. The recruitment process began at village clinics where PLHA received routine health care and services.
After a participant had provided written informed consent, the assessment was administered via computer-assisted personal interview (CAPI) method in a private room at the village clinic or at another preferred venue, with interviewers reading questions to the participants and recording their responses on computers. For illiterate participants or participants with low education attainments, the interviewer was available to explain the meaning of the survey questions. Each assessment lasted approximately 45–60 min. Participants each received 50 yuan (U.S. $8.3) for their participation. The refusal rate was less than 5%. The study protocol was approved by the institutional review boards (IRBs) of the collaborating institutions in China and the United States.
Measures
PTSD Symptoms
We evaluated HIV diagnosis-related PTSD symptoms using an eight-item scale based on the PTSD diagnostic criteria set forth in the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV; 27) and the UCLA (University of California Los Angeles) PTSD Reaction Index for DSM-IV [27]. The PTSD diagnostic criteria in DSM-IV have been widely used to capture PTSD symptoms associated with all kinds of traumatic events, and previous studies have validated its cultural adaption in rural China where the education level is limited [28, 29]. The measure has previously been pilot tested among PLHA in rural Anhui, and demonstrated an acceptable internal consistency in the pilot sample. The eight-item scale includes three clusters of characteristic symptoms of PTSD among PLHA: (1) re-experiencing (e.g. “repeated, disturbing memories, thoughts, or images of the day you found out you are HIV-positive”); (2) avoidance (e.g. “avoiding thinking, talking, or having feeling about that day”); and (3) arousal (e.g. “trouble remembering important parts of that day”). Participants were asked to rate the frequency with which they experienced each of the eight assessed symptoms during the past month (0 = not at all; 1 = a little; 2 = a moderate amount; 3 = very much; 4 = an extreme amount). Scores on each scale were totalled to create an overall measure that ranged from 0 to 32, with a higher score indicating higher level of PTSD symptoms. In our sample, the scale’s internal consistency (Cronbach’s alpha) was 0.85.
Physical Functioning
We used the Medical Outcomes Study HIV Health Survey (MOS-HIV) to evaluate participants’ physical functioning [30]. The six-item physical dimension was adopted to assess the extent to which participants’ health limited their daily activities, such as “eating, dressing, bathing or using the toilet”. This scale has been pilot validated among PLHA in rural China and rural Thailand, and demonstrated an acceptable internal consistency in the pilot sample [31]. The scores for each item were totalled to generate a physical functioning score ranging from 6 to 18, with a higher score indicating better physical functioning. The scale’s internal consistency (Cronbach’s alpha) was 0.75.
Social Functioning
The social functioning measure was adopted from the Social Adaptation Self-evaluation Scale (SASS), which was developed based on the work of Bosc et al. [32]. We selected five out of the 21 items on the SASS to evaluate participants’ social motivation and engagement. We have validated this scale in the pilot study of the aforementioned randomized controlled intervention trial among PLHA in rural Anhui. Sample items include “you find it difficult to talk to people at present” and “you prefer to spend time on your own”. Each answer was scored from 1 (definitely true) to 5 (definitely false), with a higher score indicating better social functioning. The scale’s internal consistency (Cronbach’s alpha) was 0.73.
Data Analysis
All analyses were conducted using SAS software, version 9.4 (SAS Institute, Inc., Cary, NC, USA). First, we summarized the demographic and background characteristics, and conducted analysis of variance (ANOVA) to examine differences in PTSD symptom scores across subgroups stratified by selected characteristics. Subsequently, Pearson’s correlation analysis was performed to investigate the relationship between each pair of the selected variables, which included demographic traits, PTSD symptoms, physical functioning and social functioning. Third, we used the multiple linear regression analysis to examine the adjusted association between PTSD symptoms and other selected variables. Finally, structural equation modeling (SEM) was performed to explore mediational relationships among the variables of interest. The final model excluded pathways for non-significant loadings with a p value higher than 0.100; age and gender were retained, regardless of their significance level. Goodness of model fit was evaluated using the goodness-of-fit index (GFI), p-value of Chi square test, and root mean square error of approximation (RMSEA; 33). Acceptable model fit is determined by the values of GFI greater than 0.90, p-value of Chi square test >0.05, and an RMSEA less than 0.08 [33].
Results
Out of the 522 participants who completed the survey, 288 (55%) were female. The mean age of the sample was 48.6 years old, with the majority (N = 358; 69%) between 36 and 55 years of age. Most of the participants (N = 425; 81%) were married or currently living with a partner. Approximately 40% (N = 210) of the sample were illiterate. The average total family income of last year was about 14,598 yuan (U.S. $2383). Approximately half (N = 256; 49%) of the PLHA in this study were diagnosed with HIV prior to the year of 2003. Participants’ demographic and background characteristics are summarized in Table 1.
Out of the total PTSD symptom score of 32, the study participants had an average score of 9.7 (SD = 7.2). Significant differences in PTSD symptoms were observed across subgroups stratified by age (F = 3.03; p = 0.029), gender (F = 6.74; p = 0.010), and education (F = 3.23; p = 0.040). Relatively lower level of PTSD symptoms was reported in participants who were at least 55 years of age (mean ± SD: 8.2 ± 6.9), or male (mean ± SD: 8.8 ± 6.7), or had more than 6 years of education (mean ± SD: 8.2 ± 6.9) compared to participants in other subgroups (Table 1).
Pearson’s correlation analysis showed that PTSD symptoms were significantly correlated with gender (r = 0.11; p = 0.010), physical functioning (r = −0.12; p = 0.006), and social functioning (r = −0.29; p < 0.001). Social functioning was correlated with age (r = 0.10; p = 0.020), family income (r = 0.19; p < 0.001), and physical functioning (r = 0.17; p < 0.001). We also found that physical functioning was associated with age (r = −0.32; p < 0.001), female gender (r = −0.21; p < 0.001), marriage (r = 0.10; p = 0.027), education (r = 0.21; p < 0.001) and family income (r = 0.09; p = 0.029). After controlling for other variables of interest, lower level of PTSD symptoms was only associated with better social functioning (standardized estimate = −0.26; p < 0.001). Other selected variables did not show significant associations with PTSD symptoms in the multiple linear regression analysis (Table 2).
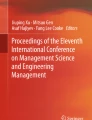
In light of the correlation and multiple regression findings, we hypothesized that social functioning might have a mediation effect on the relationship between PTSD symptoms and other demographic and background variables. Figure 1 illustrates the final mediation model fitted by SEM. Older age exhibited an indirectly negative association with PTSD symptoms mediated by better social functioning (standardized indirect estimate = −0.04; p = 0.001). Higher family income showed an indirect association with lower level of PTSD symptoms via better social functioning (standardized indirect estimate = −0.04; p < 0.001). Better physical functioning also exhibited an indirectly negative association with PTSD symptoms mediated by better social functioning (standardized indirect estimate = −0.05; p < 0.001). Gender, marital status, education, and time of HIV diagnosis were tested in the initial SEM, but did not demonstrate statistical significance (p > 0.100). The overall goodness-of-fit of the final model was adequate as the following indices suggested an acceptable fit: GFI = 0.99, p-value of Chi square test = 0.872, and RMSEA = 0.06.

The mediation effect of social functioning on association between PTSD symptoms and selected characteristics
Discussion
The participants in the study reported various levels of PTSD symptoms, and the level is particularly higher among subgroups including females, middle-age groups, and patients with low education. Given the negative impact of PTSD on progression of HIV infection, access to care and treatment adherence [17–20], the occurrence of PTSD symptoms is threatening PLHA’s quality of life in rural China. Thus, screening and management of PTSD and other mental health problems is essential and should be integrated into current HIV-related healthcare services. However, there exists a huge gap between need for mental health care and sufficiently trained professionals in rural China [34, 35]. Healthcare providers in village-level health facilities lack knowledge and skills to diagnose and treat mental illnesses of HIV-positive individuals [35]. PTSD and other psychiatric problems remained disproportionally undiagnosed, and the available mental health care is very limited [34]. Intervention efforts are urgently needed to provide training to healthcare providers in rural areas on how to identify and tackle psychiatric illnesses, like PTSD, for PLHA.
The study revealed a negatively direct association between HIV diagnosis-related PTSD symptoms and social functioning among PLHA in rural China. One possible explanation for this finding is that PLHA who have higher level of PTSD symptoms may find it more difficult or be less willing to interact with other people, adapt to their social environment and be involved in community life. In rural China, diagnosis of a life-threatening disease like HIV can easily drive people to be socially withdrawn due to enormous stress, great anxiety and deep depression [8, 21, 36, 37]. Prior studies have consistently demonstrated that mental health problems affect the abilities of PLHA to maintain their social lives and relationships with others [15, 38]. Another possible explanation of the aforementioned finding is that poor social functioning among PLHA may worsen mental health problems and PTSD symptoms. Bennett et al. [39] and Breet et al. [40] found that experiencing social isolation and negative changes in social identity (i.e. a perception of oneness with a group) might exacerbate symptoms of PTSD [41]. PLHA in rural China may suffer social isolation from their community because of reasons like stigmatization, and it would further harm their mental health [42, 43].
The study also found that physical functioning exhibited an indirectly negative association with PTSD symptoms. This finding is consistent with prior studies indicating that psychological illnesses such as PTSD are associated with worse physical health outcomes [16, 18, 44]. One possible interpretation is that among PLHA, physical functioning is highly correlated with social functioning that may play a role in mediating the relationship between PTSD symptoms and physical health. Among the participants who were in relatively poor physical health, only the one who also had poor social functioning may have experienced particularly higher level of PTSD symptoms. The SEM result in the study did provide evidence to the mediation role hypothesis. In addition, the study demonstrated that participants with older age or higher family income had relatively lower level of PTSD symptoms as mediated by social functioning. This finding indicates that such individuals may have stronger social connections and better abilities to handle and recover from traumatic life events [45, 46].
Several limitations should be noted when interpreting the study results. First, this investigation used a cross-sectional study design to examine factors associated with PTSD symptoms. Therefore, causal inferences could not be drawn. Future study to better understand the mechanisms of PTSD among PLHA in China is needed. Second, our study design did not include diagnosing participants with PTSD; such diagnosis should be established via thorough clinical assessment and based on the judgment of trained clinicians [9]. Nonetheless, the self-report measures used in this study may be useful tools for screening and assessing PTSD symptoms [47]. In addition, exposure to other traumatic event that could potentially exacerbate HIV-diagnosis related PTSD symptoms was not measured in this study. Last but not least, HIV epidemics in China have changed dramatically over time. Thus, given that half of our study participants were infected with HIV prior to 2003, our results cannot necessarily be generalized to all PLHA in rural China. Further study is suggested to investigate the issue of PTSD among PLHA infected through other routes.
Despite aforementioned limitation, this study has important implications for future practices and research. In current China, with the continuous increase in the reported HIV-positive individuals, to engage and retain PLHA in the continuum of care become one of the major challenges [21]. To overcome this challenge, it is urgent to fully address the problem of co-occurrence of HIV and PTSD as well as other mental health disorders, since the psychiatric illnesses would hinder improvement of treatment outcomes and quality of life of PLHA. It is highly recommended that future intervention programs and policies underscore the mental and social aspects of PLHA, and provide adequate training for health professionals in low-resource settings [48].
References
Neigh GN, Rhodes ST, Valdez A, Jovanovic T. PTSD co-morbid with HIV: separate but equal, or two parts of a whole? Neurobiol Dis. 2016;92:116–23.
UNAIDS. Fact sheet 2015. http://www.unaids.org/en/resources/campaigns/HowAIDSchangedeverything/factsheet. Accessed 27 June 2016.
Applebaum AJ, Bedoya CA, Hendriksen ES, Wilkinson JL, Safren SA, O’cleirigh C. Future directions for interventions targeting PTSD in HIV-infected adults. J Assoc Nurses AIDS Care. 2015;26(2):127–38.
Beckerman NL, Auerbach C. Post-traumatic stress disorder and HIV: a snapshot of co-occurrence. Soc Work Health Care. 2010;49(8):687–702.
Machtinger EL, Wilson TC, Haberer JE, Weiss DS. Psychological trauma and PTSD in HIV-positive women: a meta-analysis. AIDS Behav. 2012;16(8):2091–100.
Martin L, Kagee A. Lifetime and HIV-related PTSD among persons recently diagnosed with HIV. AIDS Behav. 2008;15(1):125–31.
Theuninck AC, Lake N, Gibson S. HIV-related posttraumatic stress disorder: investigating the traumatic events. AIDS Patient Care STDS. 2010;24(8):485–91.
Tsao J, Dobalian A, Moreau C, Dobalian K. Stability of anxiety and depression in a national sample of adults with human immunodeficiency virus. J Nerv Ment Dis. 2004;192(2):111–8.
American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Washington, DC: American Psychiatric Association; 2013.
Sherr L, Nagra N, Kulubya G, Catalan J, Clucas C, Harding R. HIV infection associated post-traumatic stress disorder and post-traumatic growth: a systematic review. Psychol Health Med. 2011;16(5):612–29.
Brief DJ, Bollinger AR, Vielhauer MJ, et al. Understanding the interface of HIV, trauma, post-traumatic stress disorder, and substance use and its implications for health outcomes. AIDS Care. 2004;16(Suppl 1):S97–120.
Leserman J. Role of depression, stress, and trauma in HIV disease progression. Psychosom Med. 2008;70(5):539–45.
Bogart L, Wagner G, Galvan F, Landrine H, Klein D, Sticklor L. Perceived discrimination and mental health symptoms among black men with HIV. Cult Divers Ethn Minor Psychol. 2011;17(3):295–302.
Gard TL, Hoover DR, Shi Q, et al. The impact of HIV status, HIV disease progression, and post-traumatic stress symptoms on the health-related quality of life of Rwandan women genocide survivors. Qual Life Res. 2012;22(8):2073–84.
Rzeszutek M, Oniszczenko W, Żebrowska M, Firląg-Burkacka E. HIV infection duration, social support and the level of trauma symptoms in a sample of HIV-positive Polish individuals. AIDS Care. 2014;27(3):363–9.
Pence BW, Shirey K, Whetten K, et al. Prevalence of psychological trauma and association with current health and functioning in a sample of HIV-infected and HIV-uninfected Tanzanian adults. PLoS ONE. 2012;7(5):e36304.
Pacella M, Armelie A, Boarts J, et al. The impact of prolonged exposure on PTSD symptoms and associated psychopathology in people living with HIV: a randomized test of concept. AIDS Behav. 2012;16(5):1327–40.
Seedat S. Interventions to improve psychological functioning and health outcomes of HIV-infected individuals with a history of trauma or PTSD. Curr HIV/AIDS Rep. 2012;9(4):344–50.
Wagner GJ, Bogart LM, Galvan FH, Banks D, Klein DJ. Discrimination as a key mediator of the relationship between posttraumatic stress and HIV treatment adherence among African American men. J Behav Med. 2012;35(1):8–18.
Weinstein TL, Li X. The relationship between stress and clinical outcomes for persons living with HIV/AIDS: a systematic review of the global literature. AIDS Care. 2015;28(2):160–9.
National Health and Family Planning Commission of the People’s Republic of China. 2015 China AIDS response progress report. http://www.unaids.org/sites/default/files/country/documents/CHN_narrative_report_2015.pdf. Accessed 27 June 2016.
Wu Z, Rou K, Cui H. The HIV/AIDS epidemic in China: history, current strategies and future challenges. AIDS Educ Prev. 2004;16(Supplement A):7–17.
Zhang L, Chow EP, Jing J, et al. HIV prevalence in China: integration of surveillance data and a systematic review. Lancet Infect Dis. 2013;13(11):955–63.
He N, Detels R. The HIV epidemic in China: history, response, and challenge. Cell Res. 2005;15(11–12):825–32.
World Health Organization (WHO). Prevalence of PTSD. http://www.ptsd.va.gov/professional/PTSD-overview/epidemiological-facts-ptsd.asp. Accessed 27 June 2016.
Ji G, Detels R, Wu Z, Yin Y. Correlates of HIV infection among former blood/plasma donors in rural China. AIDS. 2006;20(4):585–91.
Pynoos RS, Rodriguez N, Steinberg AS, Frederick C. The UCLA PTSD reaction index for DSM IV (Revision 1). Los Angeles: UCLA Trauma Psychiatry Program; 1998.
American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th ed. Washington, DC: American Psychiatric Association; 1994.
Wang X, Gao L, Shinfuku N, Zhang H, Zhao C, Shen Y. Longitudinal study of earthquake-related PTSD in a randomly selected community sample in north China. Am J Psychiatry. 2000;157(8):1260–6.
Wu AW, Revicki DA, Jacobson D, Malitz FE. Evidence for reliability, validity and usefulness of the Medical Outcomes Study HIV Health Survey (MOS-HIV). Qual Life Res. 1997;6(6):481–93.
Li L, Lee SJ, Wen Y, Lin C, Wan D, Jiraphongsa C. Antiretroviral therapy adherence among patients living with HIV/AIDS in Thailand. Nurs Health Sci. 2010;12(2):212–20.
Bosc M, Dubini A, Polin V. Development and validation of a social functioning scale, the Social Adaptation Self-evaluation Scale. Eur Neuropsychopharmacol. 1997;7(Suppl 1):S57–70 (discussion S71-3).
O’Rourke N, Hatcher L. A step-by-step approach to using SAS for factor analysis and structural equation modeling. 2nd ed. Cary: Sas Institute; 2013.
Ma Z, Huang H, Chen Q, et al. Mental health services in rural China: a qualitative study of primary health care providers. Biomed Res Int. 2015;2015:151053.
Cui G, Li H, Yao M. A mental health training programme for Chinese rural general practitioners. Med Educ. 2015;49(5):538–9.
Jin H, Atkinson JH, Yu X, et al. Depression and suicidality in HIV/AIDS in China. J Affect Disord. 2006;94(1):269–75.
Gu J, Lau JT, Li M, Li H, et al. Socio-ecological factors associated with depression, suicidal ideation and suicidal attempt among female injection drug users who are sex workers in China. Drug Alcohol Depend. 2014;144:102–10.
National Institute of Mental Health. Chronic Illness & Mental Health. http://www.nimh.nih.gov/health/publications/chronic-illness-mental-health-2015/index.shtml. Accessed 27 June 2016.
Bennett DS, Hersh J, Herres J, Foster J. HIV-related stigma, shame, and avoidant coping: risk factors for internalizing symptoms among youth living with HIV? Child Psychiatry Hum Dev. 2016;47(4):657–64.
Breet E, Kagee A, Seedat S. HIV-related stigma and symptoms of post-traumatic stress disorder and depression in HIV-infected individuals: does social support play a mediating or moderating role? AIDS Care. 2014;26(8):947–51.
Haslam SA. Making good theory practical: five lessons for an Applied Social Identity Approach to challenges of organizational, health, and clinical psychology. Br J Soc Psychol. 2014;53(1):1–20.
Li L, Lin C, Wu Z, et al. Stigmatization and shame: consequences of caring for HIV/AIDS patients in China. AIDS Care. 2007;19(2):258–63.
Zang C, Guida J, Sun Y, Liu H. Collectivism culture, HIV stigma and social network support in Anhui, China: a path analytic model. AIDS Patient Care STDS. 2014;28(8):452–8.
Reif SS, Pence BW, Legrand S, et al. In-home mental health treatment for individuals with HIV. AIDS Patient Care STDS. 2012;26(11):655–61.
Dévieux JG, Malow RM, Attonito JM, et al. Post-traumatic stress disorder symptomatology and alcohol use among HIV-seropositive adults in Haiti. AIDS Care. 2013;25(10):1210–8.
Mutabazi-Mwesigire D, Katamba A, Martin F, Seeley J, Wu AW. Factors that affect quality of life among people living with HIV attending an urban clinic in Uganda: a cohort study. PLoS ONE. 2015;10(6):e0126810.
Barlow DH. Clinical handbook of psychological disorders: a step-by-step treatment manual. New York: The Guilford Press; 2008.
Yang JP, Leu J, Simoni JM, Chen WT, Shiu CS, Zhao H. “Please Don’t Make Me Ask for Help”: implicit social support and mental health in chinese individuals living with HIV. AIDS Behav. 2015;19(8):1501–9.
Acknowledgement
This study was funded by National Institute of Child Health & Human Development/NIH (Grant Number R01HD068165). We would like to thank our project team members in Anhui, China for their contributions to this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All the authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Luo, S., Lin, C., Ji, G. et al. Post-traumatic Stress Disorder Symptoms Among People Living with HIV/AIDS in Rural China. AIDS Behav 21, 3202–3208 (2017). https://doi.org/10.1007/s10461-016-1641-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-016-1641-1