
Abstract
Objective
During the coronavirus pandemic lockdowns, general medical complications have received the most attention, and few studies have examined the association between the COVID-19 lockdown and eating disorders (ED). This study aimed to investigate the impact of the coronavirus lockdowns on ED symptoms severity and summarize factors associated with lockdowns that led to changes in eating disorders.
Method
PubMed, Scopus, and Cochrane Library databases were searched for studies measuring the impact of coronavirus lockdowns on ED symptoms.
Results
A total of 132 studies were retrieved, after abstract screening and removal of duplicates, 21 papers were full-text screened, and 11 eligible papers were identified. Factors associated with symptomatic deterioration in ED patients during COVID-19 lockdowns included disruption of lifestyle routine, social isolation, reduced access to usual support networks, limited or no access to healthcare and mental care services, and social anxiety.
Discussion
Overall, the pandemic lockdowns were associated with worsening of eating disorders.
This triggering environment can lead to increased anxiety and depression symptoms, change in dietary habits, and eventually result in worsening eating disorder symptoms.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
The novel coronavirus disease 2019 (COVID-19) was first reported in Wuhan, China (Temsah et al. 2020). The World Health Organization (WHO) declared that the outbreak was considered a global pandemic on 11 March 2020 (Anand et al. 2020). The rapid increase of confirmed cases and the death rate led to implementing public health measures to prevent transmission. Some important measures included lockdown, travel restrictions, and physical distancing. Apart from the growing financial loss in industries (Nicola et al. 2020), the economic downturn resulted in an increased unemployment rate and had an adverse impact on the quality of life (Roca et al. 2013). Unlike other infectious diseases, the pandemic influenced both physical and mental wellbeing (Hasan and Bao 2020). Fear of uncertain prognoses, shortage of testing and treatment resources, unexpected lockdowns, and social isolation may precipitate psychological distress and mental illness across the population (Mamun and Ullah 2020; Wang et al. 2020a, b), especially in people with pre-existing mental health difficulties (Holmes et al. 2020). With increased feelings of isolation and loneliness during the coronavirus pandemic and lockdown, patients with eating disorders may face an even greater challenge for recovery. A study by Touyz et al. (2020) concluded that eating disorders involve a problematic and unhealthy relationship with food, and the symptoms may be enhanced during the disease outbreak due to food insecurity and panic buying.
Countries and territories worldwide have put public health measure in place (e.g., lockdown, mandatory face coverings) to decrease the spread of the coronavirus across communities (Graell et al. 2020; Orgilés et al. 2020). The COVID-19 lockdowns might trigger eating disorder symptomatology in four aspects. First is the disruption of the living situation. Travel restrictions, limited access to healthcare services, and grocery stores might cause sudden lifestyle changes and social isolation in people suffering from eating disorders. Naja & Hamadeh’s (2020) study concluded that the lockdown measures might induce irregular eating habits and sedentary behaviors. Several countries have issued the recommendation to limit grocery trips during the pandemic to promote social distancing in public places (Ruth et al. 2020), and this might encourage patients with eating disorders to purchase excess quantities of food. Eating disorder patients experienced limited access to their usual support networks during the enforced lockdown, which led to a reduced motivation for recovery and worsened eating disorder symptoms. Second is the increasing consumption of social media. Technology is vital during this pivotal time, as physical associations and outdoor activities are limited and people tend to rely on the internet. However, media can influence disordered eating in many ways. Eating disorder levels might worsen through exposure to unrealistic body image, negative stories, and stressful news (Rodgers et al. 2020). Anxiety during quarantine and weight stigma can contribute to raising body shame and disordered eating (Robertson et al. 2021), particularly in those with a current or historic eating disorder. In addition, accessibility to food can exacerbate irregular eating behaviors. According to a UK household food security survey, 16.2% of participants have experienced food insecurity since the lockdown, while 21.6% worried about the availability of food (Loopstra 2020). Population with a higher level of food insecurity are more likely to endorse binge eating and obesity (Becker et al. 2017; Rasmusson et al. 2018). A food frequency questionnaire in Denmark discovered that people tended to change their food-related habits during the pandemic, and showed an increasing preference for food high in sugar and fat (Janssen 2020). In general, the average sales of frozen food, cakes, snacks, and other shelf-stable foods have increased since the start of the pandemic, while the consumption of fresh fruit and vegetables has decreased. Lastly is the negative emotions related to the coronavirus and the unexpected lockdown, which might lead to an increasing level of stress and changes in appetite for patients with eating disorders (ED) (Rodgers et al. 2020). Therefore, it is critical to analyze the impact of the COVID-19 pandemic-related lockdowns on disordered eating behaviors, and there is an urgent need for interventions to support these vulnerable populations.
The impact of lockdown measures is interrelated with the coronavirus pandemic, and this research work focused on the association between the COVID-19 pandemic-related lockdown and eating disorders. This study aimed to systematically review the evidence on eating disorders and the coronavirus lockdowns, investigate factors impacting changes in ED levels due to the COVID-19 lockdowns, and generate an overview of the association between ED symptom severity and the global pandemic. The specific objectives of the study were:
-
1.
To examine if eating disorder symptoms worsened during the COVID-19 lockdown?
-
2.
To describe what factors of the coronavirus lockdowns impacted eating disorder symptoms (e.g., social isolation, food insecurity)?
Methodology
Literature search
The literature review was carried out in the following databases: PubMed, Scopus, and Cochrane Library. Reference lists of relevant articles were also searched. The following search terms were used: “coronavirus” OR “COVID-19” OR “SARS-CoV-2” AND “lockdown” AND “eating disorders”. Searches were conducted up to April 2021, all relevant articles published between the start of the pandemic in 2019 through April 2021 were considered for inclusion.
Eligibility criteria
The inclusion criteria incldued epidemiological studies on patients with diagnosed eating disorders and reported changes in ED symptoms severity (either self-reported or through medical records) before and after COVID-19 lockdown. Exclusion criteria included study populations without a primary diagnosis of eating disorders or did not contain a comparison of ED symptoms before and during the lockdown. For studies that included both healthy individuals and ED patients, we only focused on the outcome for the ED group. Review articles, editorials, and opinions were excluded. No restrictions on the region of publication, publishing language, gender, or the age of the patients were imposed.
Study selection and data collection procedure
First duplicate articles were excluded, then titles and abstracts, followed by full-text article screening were applied to identify articles that met our inclusion criteria. Data were extracted by the main author and search outcomes were imported to Endnote for review. The following data were extracted from the studies: author name, year of publication, demographic and methodological characteristics (e.g., mean age and gender of the study participants, sample size, study design), diagnosis (anorexia nervosa, bulimia nervosa, binge eating disorder, and other specified eating disorder), and description of the outcomes.
Quality assessment
The main author did the quality assessment of all studies (n=11) using the Newcastle-Ottawa Scale (Wells et al. 2000). There are three domains considered in the scale: selection, comparability, and outcome. All 11 studies satisfy the minimum ratings for the review, with 4 having a fair quality rating, and 7 a good quality rating.
Results
Study selection
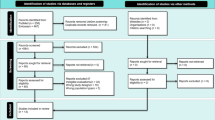
The systematic search identified 132 articles presenting outcomes for individuals with eating disorder symptoms during the COVID-19 pandemic lockdowns. After the removal of duplicates, 107 studies remained. Eighty-six studies did not meet the inclusion criteria and were discarded after reviewing the title and abstract. The remaining 21 studies were full-text screened, and 11 studies were considered eligible for the systematic review. Two studies, Graell et al. (2020) and Castellini et al. (2020) included both individuals with and without EDs, hence only data on ED patients were extracted from these studies.
Eleven papers report the association between the COVID-lockdown measures and ED symptoms, participants’ information was collected online or via telephone surveys, video conferences, and face-to-face interviews. Nine out of 11 studies were cohort studies and compared participants’ ED symptoms before and during the COVID-19 lockdown. The survey includes questions on levels of quarantine and changes in eating behavior during the lockdown. Two cross-sectional studies examined participants’ ED patterns during the coronavirus confinement period. Figure 1 presents a flow chart for study inclusion and exclusion, and the details of studies included are summarized in Table 1.

Flow chart for study inclusion and exclusion
Impact of COVID-19 lockdown on eating disorders
Most papers (n=7, 63%) adapted screening measures and questionnaires to determine eating disorder symptomology. Trott et al. (2021) used the Eating Attitudes Test 26 (EAT-26) to examine the change in ED during the lockdown, and the cut-off score is greater or equal to 20 (Garner 1991). Trott et al. (2021) compared the eating and exercise behavior pre-COVID-19 and post the first lockdown. The average score for the eating attitude test is significantly higher post-COVID-19, which suggests lockdown and quarantines might trigger higher levels of morbid eating behaviors. Cecchetto et al. (2021) measured eating disorder psychopathology by the 7-Item Binge-Eating Disorder Screener (Herman et al. 2016) and applied the Dutch Eating Behaviour Questionnaire to investigate emotional eating during the pandemic lockdown (Dakanalis et al. 2013). Machado et al. (2020) applied the Eating Disorder Examination-Questionnaire to measure ED symptoms and included specific questions for degrees of lockdown. Similarly, Robertson et al. (2021) requested that participants self-report their mental disorder history. The changes in eating behavior and attitudes during the lockdown were assessed by 5-point Likert Scale survey questions. Branley-Bell and Talbot (2020) adapted the Rumination Response Scale in an online survey, containing both closed and open-ended questions on eating disorders and the COVID-19 pandemic.
Some studies (n=4, 36%) gathered participants’ data by reviewing their medical records. ED patients were diagnosed according to the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5) (Baenas et al. 2020; Monteleone et al. 2021a, b; Leenaerts et al. 2021). Monteleone et al. (2021a, b) classified the study into three-time points, which included before coronavirus restrictions, during the pandemic restrictions, and transition from lockdown to reopening. Survey questions related to eating disorders were adapted from the Eating Disorders Inventory (Garner 1991). Graell et al. (2020) and compared patients in day hospitals with those receiving treatment in an outpatient clinic to investigate the impact of therapy cancellation on eating disorders. Anorexia nervosa and restrictive food intake disorder were the more common diseases among adolescent and school-age patients, 41.9% of participants experienced reactivation of ED symptoms during the lockdown period (Graell et al. 2020).
Several of the studies suggested that confinement was closely related to increased eating disorders and anxiety symptoms among the general population (Graell et al. 2020; Termorshuizen et al. 2020; Fernández-Aranda et al. 2020a, b; Herle et al. 2021; Loth et al. 2008). Leenaerts et al. (2021) concluded that participants spent more time at home with their families or housemates due to the nature of enforced lockdowns. The lockdown and quarantine measures led to changes in daily routine, surroundings, and social context, especially for patients with eating disorders. Patients who experienced extreme changes were more vulnerable to negative effects, including increased binge eating frequency (Cecchetto et al. 2021; Leenaerts et al. 2021). The outcome was supported by Machado et al. (2020), the vast majority of participants considered that their daily life were moderately to extremely impacted by the lockdown, which led to emotion regulation problems, limited or no access to healthcare services, and worsened eating disorder symptoms.
Interestingly, several studies reported symptom relief for some participants. In Branley-Bell and Talbot’s (2020) study, the overwhelming majority (86.7%) reported increasing ED symptoms, but two patients reported their symptoms had slightly improved during the lockdown. Baenas et al. (2020) determined that 25.7% of patients reported symptoms worsened during the lockdown, while 51.4% reported their symptoms became less dominant. Patients with AN showed a progressive weight gain and improvement of ED symptoms during lockdown (Castellini et al. 2020). In line with this, a study by Graell et al. (2020) found that approximately 80% of child and adolescent participants report their family relationship has improved during the 8-week confinement period, which is associated with alleviating anorexia nervosa symptoms.
Discussion
Summary of the results
Eleven papers examined changes in ED symptom pre vs post-COVID-19 lockdowns, and one study included a following re-opening period. Women and young people had greater concern about their body image and appearance (Williamson et al. 2004; Robertson et al. 2021), faced more difficulties in regulating eating (Robertson et al. 2021), and had a greater risk of worsening eating disorder symptoms during the COVID-19 lockdown (Pierce et al. 2020). In general, all studies concluded that the pandemic lockdown was associated with a worsening of eating disorders, and it led to higher levels of anxiety and depressive symptoms in ED patients. The severity of ED symptoms decreased to normal levels during the transition from lock-down to re-opening (Monteleone et al. 2021a, b). However, some participants reported relieving symptoms during the confinement period, especially for anorexia nervosa patients. The possible explanation is that patients continue to receive e-therapy during COVID-19 lockdown (Weissman et al. 2020), stable family relationships, and fewer social stressors might contribute to reducing symptoms of anorexia nervosa (Walsh and McNicholas 2020).
Interpretation of the results
COVID-19 lockdown has placed restrictions on movement, which reduced access to usual supporting systems and healthcare services (Graell et al. 2020; Weissman et al. 2020), limited access to food, and negative emotions in people who suffer from eating disorder conditions.
Social isolation and loneliness
Lockdown and the stay-at-home orders exacerbated social isolation and loneliness among this population (Smith and Lim 2020), especially for people who live alone. Most participants, except essential workers, were forced to work from home or were unemployed during the confinement period. People had limited interactions with anyone outside due to home isolation during the lockdown. Branley-Bell and Talbot (2020) highlighted that spending time with friends and relatives can be an important factor and motivation in the recovery process for ED patients. The alterations in the living situation during the confinement period increased social isolation and limited access to their usual support networks (Branley-Bell and Talbot 2020) and eventually led to worsened ED symptoms (Conceição et al. 2021).
Limited access to healthcare
One of the major problems for ED patients during lockdown was reduced access to face-to-face treatment (Graell et al. 2020). Although some patients received online treatment (e.g., teletherapy and videoconferencing) during the confinement period, they stated that online support was an alternative but could not replace the traditional support mechanisms (Branley-Bell and Talbot 2020). During the COVID-19 pandemic peak, some psychiatric wards were downsized, closed, or converted into wards for coronavirus patients (Graell et al. 2020). ED patients experienced treatment suspension, cancellation of non-urgent treatment, and a reduction in hospital bed availability (Touyz et al. 2020; Branley-Bell and Talbot 2020).
Dietary Changes & Food Restrictions
The lockdown measures placed restrictions on people’s movement and influenced the accessibility of food. Robertson et al. (2021) outlined that lockdown can impact people’s eating patterns and body image. The majority of participants have irregular eating patterns and experienced worsened ED symptoms during the COVID-19 outbreak (Chan and Chiu 2021; Alamrawy et al. 2021), which align with a previous study demonstrating the association between dietary changes and increasing eating disorders symptoms (Jacobi et al. 2004). Simone et al. (2021) highlights the common changes in eating behavior during the pandemic are mindless eating, increased or decreased appetite, and exposure to unhealthy food. The sudden change in eating habits can be one of the warning signs for ED symptomatology (Chan and Chiu 2021). COVID-19 lockdown measures can lead to a reduction in dietary intake, including dietary restrictions and loss of appetite as a coping strategy to stress levels (Simone et al. 2021; Polivy and Herman 2002). The finding is supported by Graell et al. (2020) and Rodgers et al. (2020) who noted that AN patients’ intolerance of uncertainty during the pandemic lockdown associated with the drive for thinness and body dissatisfaction can lead to weight-control behaviors to compensate for the fear of losing control in their daily routine (Brown et al. 2017; Frank et al. 2012; Tiggemann and Raven 1998) and deterioration in ED symptoms. Furthermore, financial difficulties during the COVID-19 lockdown might lead to food restrictions, unhealthy eating habits, depression, and anxiety symptoms, and result in increasing disordered eating symptoms (Simone et al. 2021).
Psychosocial impact
Although lockdown restrictions were important to prevent the spread of COVID-19, it negatively impacted eating disorders and emotion control (Cecchetto et al. 2021). Monteleone et al. (2021a, b), Baenas et al. (2020), and Brooks et al. (2020) stated that COVID-19 and lockdown were characterized by fear of infection and uncertainty, boredom, social isolation, financial difficulties, and increasing mental health problems. Several studies mentioned anxiety and depressive symptoms were associated with increased odds of concurrent eating disorders (Simone et al. 2021; Chan and Chiu 2021; Meyer et al. 2011; Errisuriz et al. 2016). Negative emotions (e.g., sadness and fear) were important precursors for eating disorders patients (Naumann et al. 2014) and tend to have detrimental effects on restrictive eating and ED symptoms (Naumann et al. 2015). The risk of developing binge eating behaviors increased dramatically under negative emotions (Whiteside et al. 2005). Allison and Timmerman (2007) and Mason and Lewis (2017) concluded that context is vital in triggering eating disorder symptoms. Therefore, the combination of a health crisis (COVID-19 pandemic), social isolation (enforced lockdown), and negative emotions could lead to worsening ED symptoms and general psychopathology (anxiety and depression) in the population (Shanahan et al. 2020; Serafini et al. 2020).
Contradicting findings
Fernández-Aranda et al. (2020a, b) observed a significant decrease in ED symptoms in AN patients after the confinement period. A possible explanation for this phenomenon is that patients were able to access support from e-therapy or follow the previous treatment plan. Patients who lived with families might have received increased social support and strengthened family relationships during the lockdown (Termorshuizen et al. 2020), resulting in alleviating ED symptoms. Especially for children and adolescents, as their parents might supervise their dietary intake (Graell et al. 2020; Walsh and McNicholas 2020).
Limitations
The present study is limited by several factors. First, all identified studies were conducted in Europe (four in England, three in Italy, two in Spain, and one in Belgium and Portugal) and results may differ and not be generalizable to other settings. Second, the sample size was relatively small due to limited evidence on this topic. Lastly, lockdown measures have been different across countries, thus the impact on ED patients might differ.
Conclusions and further directions
In general, coronavirus and lockdown restrictions were closely associated with worsening eating behaviors, depression, and anxiety symptoms among ED patients. The COVID-19 pandemic lockdown led to disruption of the living situation, increasing social isolation and loneliness, financial difficulties, and an unhealthy pattern of food consumption in the general population, which is positively associated with worsened ED symptoms. The majority of studies reported lockdown restrictions had a moderate to an extreme level of impact on life routines and many people experienced difficulties accessing healthcare services and mental healthcare, this triggering environment can create additional challenges for ED patients. However, some studies report positive outcomes during confinement and showed a recovery of anorexia nervosa symptoms. This might relate to accessing online treatment (Branley-Bell and Talbot 2020; Castellini et al. 2020; Weissman et al. 2020) and receiving support from their families (Graell et al. 2020; Walsh and McNicholas 2020).
Future systematic review studies need to examine the impact of lockdowns on other continents (e.g., Asia, Africa, North and South America, and Australia). In this systematic review, only one study included a reopening period for ED patients and concluded the disordered eating symptoms showed slow recovery from the impact of the COVID-19 lockdown (Monteleone et al. 2021a, b). Further research can extend the study period and explore the eating disorder symptoms pre and post COVID-19 lockdown, and the following re-opening period.
Availability of data and material
All data supporting this systematic review are included in published articles.
Code availability
Not applicable.
References
Alamrawy RG, Fadl N, Khaled A (2021) Psychiatric morbidity and dietary habits during COVID-19 pandemic: a cross-sectional study among Egyptian Youth (14–24 years). Middle East Current Psychiat 28(6). https://doi.org/10.1186/s43045-021-00085-w
Allison S, Timmerman GM (2007) Anatomy of a binge: Food environment and characteristics of nonpurge binge episodes. Eating Behav 8(1):31–38. https://doi.org/10.1016/j.eatbeh.2005.01.004
Anand S, Montez-Rath M, Han J et al (2020) Prevalence of SARS-CoV-2 antibodies in a large nationwide sample of patients on dialysis in the USA: a cross-sectional study. Lancet. https://doi.org/10.1016/S0140-6736(20)32009-2
Baenas I, Caravaca-Sanz E, Granero R, Sanchez I, Riesco N, Testa G, Vintro-Alcaraz C, Treasure J, Jimenez-Murcia S, Fernandez-Aranda F (2020) COVID-19 and eating disorders during confinement: Analysis of factors associated with resilience and aggravation of symptoms. Eur Eat Disord Rev 28(6):855–863. https://doi.org/10.1002/erv.2771
Becker CB, Middlemass K, Taylor B, Johnson C, Gomez F (2017) Food insecurity and eating disorder pathology. Int J Eat Disord 50(9):1031–1040. https://doi.org/10.1002/eat.22735
Branley-Bell D, Talbot CV (2020) Exploring the impact of the COVID-19 pandemic and UK lockdown on individuals with experience of eating disorders. J Eat Disord 8:44. https://doi.org/10.1186/s40337-020-00319-y
Brown M, Robinson L, Campione GC, Wuensch K, Hildebrandt T, Micali N (2017) Intolerance of uncertainty in eating disorders: A systematic review and meta-analysis. Eur Eat Disord Rev 25:329–343. https://doi.org/10.1002/erv.2523
Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N (2020) The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet 395:912–920. https://doi.org/10.1016/S0140-6736(20)30460-8
Castellini G, Cassioli E, Rossi E, Innocenti M, Gironi V, Sanfilippo G, Felciai F, Monteleone AM, Ricca V (2020) The impact of COVID-19 epidemic on eating disorders: a longitudinal observation of pre versus post psychopathological features in a sample of patients with eating disorders and a group of healthy controls. Int J Eat Disord 53(11):1855–1862. https://doi.org/10.1002/eat.23368
Cecchetto C, Aiello M, Gentili C, Ionta S, Osimo SA (2021) Increased emotional eating during COVID-19 associated with lockdown, psychological and social distress. Appetite 160:105122. https://doi.org/10.1016/j.appet.2021.105122
Chan CY, Chiu CY (2021) Disordered eating behaviors and psychological health during the COVID-19 pandemic. Psychol Health Med 1-8. https://doi.org/10.1080/13548506.2021.1883687
Conceição E, de Lourdes M, Ramalho S, Felix S, Pinto-Bastos A, Vaz AR (2021) Eating behaviors and weight outcomes in bariatric surgery patients amidst COVID-19. Surg Obes Relat Dis. https://doi.org/10.1016/j.soard.2021.02.025
Dakanalis A, Zanetti MA, Clerici M, Madeddu F, Riva G, Caccialanza R (2013) Italian version of the Dutch Eating Behavior Questionnaire. Psychometric proprieties and measurement invariance across sex, BMI-status and age. Appetite 71:187–195
Errisuriz VL, Pasch KE, Perry CL (2016) Perceived stress and dietary choices: the moderating role of stress management. Eating Behaviors 22:211–216
Fernández-Aranda F, Casas M, Claes L, Bryan DC, Favaro A, Granero R, Treasure J (2020a) COVID-19 and implications for eating disorders. Eur Eat Disord Rev 28(3):239–245. https://doi.org/10.1002/erv.2738
Fernández-Aranda F, Munguía L, Mestre-Bach G et al (2020b) COVID Isolation Eating Scale (CIES): analysis of the impact of confinement in eating disorders and obesity—a collaborative international study. Eur Eat Disord Rev 28:871–833. https://doi.org/10.1002/erv.2784
Frank GK, Roblek T, Shott ME, Jappe LM, Rollin MD, Hagman JO, Pryor T (2012) Heightened fear of uncertainty in anorexia and bulimia nervosa. Int J Eat Disord 45(2):227–232. https://doi.org/10.1002/eat.20929
Garner D (1991) Eating disorder inventory-2. Retrieved from http://www.dottorgianfrancodelorenzis.it/doc/questionaripsicologici/EDI-2protocollo.pdf. Accessed 8 May 2021
Graell M, Moron-Nozaleda MG, Camarneiro R, Villasenor A, Yanez S, Munoz R, Martinez-Nunez B, Miguelez-Fernandez C, Munoz M, Faya M (2020) Children and adolescents with eating disorders during COVID-19 confinement: difficulties and future challenges. Eur Eat Disord Rev 28(6):864–870. https://doi.org/10.1002/erv.2763
Hasan N, Bao Y (2020) Impact of “e-Learning Crack-up” perception on psychological distress among college students during COVID-19 pandemic: a mediating role of “fear of academic year loss” Children Youth Serv Rev 118:105355. https://doi.org/10.1016/jchildyouth.2020.105355
Herle M, Smith AD, Bu F, Steptoe A, Fancourt D (2021) Trajectories of eating behavior during COVID-19 lockdown: Longitudinal analyses of 22,374 adults. Clin Nutr ESPEN 42:158–165. https://doi.org/10.1016/j.clnesp.2021.01.046
Herman BK, Deal LS, DiBenedetti DB, Nelson L, Fehnel SE, Brown TM (2016) Development of the 7-item binge-eating disorder screener (BEDS-7). Primary Care Compan CNS Disord 18(2). https://doi.org/10.4088/PCC.15m01896
Holmes EA, O’Connor RC, Perry VH, Tracey I, Wessely S, Arseneault L, Everall I (2020) Multidisciplinary research priorities for the COVID-19 pandemic: a call for action for mental health science. Lancet Psychiat. https://doi.org/10.1016/S2215-0366(20)30168-1
Jacobi C, Hayward C, de Zwaan M, Kraemer HC, Agras WS (2004) Coming to terms with risk factors for eating disorders: application of risk terminology and suggestions for a general taxonomy. Psychol Bull 130(1). https://doi.org/10.1037/0033-2909.130.1.19
Janssen M (2020) Has COVID-19 changed our relationship with food? Viewed 18 March 2021. http://www.bos-cbscsr.dk/2020/10/13/has-covid-19-changed-our-relationship-with-food/. Accessed 8 May 2021
Leenaerts N, Vaessen T, Ceccarini J, Vrieze E (2021) How COVID-19 lockdown measures could impact patients with bulimia nervosa: exploratory results from an ongoing experience sampling method study. Eat Behav 41:101505. https://doi.org/10.1016/j.eatbeh.2021.101505
Loth K, van den Berg P, Eisenberg ME, Neumark-Sztainer D (2008) Stressful life events and disordered eating behaviors: findings from Project EAT. J Adolescent Health 43(5):514–516. https://doi.org/10.1016/j.jadohealth.2008.03.007
Loopstra A (2020) Vulnerability to food insecurity since the COVID-19 lockdown. The Food Foundation
Machado PPP, Pinto-Bastos A, Ramos R, Rodrigues TF, Louro E, Goncalves S, Brandao I, Vaz A (2020) Impact of COVID-19 lockdown measures on a cohort of eating disorders patients. J Eat Disord 8(1):57. https://doi.org/10.1186/s40337-020-00340-1
Mamun MA, Ullah I (2020) COVID-19 suicides in Pakistan, dying off not COVID-19 fear but poverty?—The forthcoming economic challenges for a developing country. Brain Behav Immun. https://doi.org/10.1016/j.bbi.2020.05.028
Mason TB, Lewis RJ (2017) Examining social support, rumination, and optimism in relation to binge eating among Caucasian and African-American college women. Eating Weight Disord 22(4):693–698. https://doi.org/10.1007/s40519-016-0300-x
Meyer C, Taranis L, Goodwin H, Haycraft E (2011) Compulsive exercise and eating disorders. Eur Eat Disord Rev 19(3):174–189. https://doi.org/10.1002/erv.1122
Monteleone AM, Cascino G, Barone E et al (2021a) COVID-19 pandemic and eating disorders: What can we learn about psychopathology and treatment? A systematic review. Curr Psychiatry Rep 23:83. https://doi.org/10.1007/s11920-021-01294-0
Monteleone AM, Marciello F, Cascino G, Abbate-Daga G, Anselmetti S, Baiano M, Balestrieri M, Barone E, Bertelli S, Carpiniello B, Castellini G, Corrivetti G, de Giorgi S, Favaro A, Gramaglia C, Marzola E, Meneguzzo P, Monaco F, Oriani MG et al (2021b) The impact of COVID-19 lockdown and of the following “re-opening” period on specific and general psychopathology in people with eating disorders: the emergent role of internalizing symptoms. J Affect Disord 285:77–83. https://doi.org/10.1016/j.jad.2021.02.037
Naja F, Hamadeh R (2020) Nutrition amid the COVID-19 pandemic: a multi-level framework for action. Eur J Clin Nutr 74:1117–1121. https://doi.org/10.1038/s41430-020-0634-3
Naumann E, Tuschen-Caffier B, Voderholzer U, Svaldi J (2014) On the role of sadness in the psychopathology of anorexia nervosa. Psychiat Res 215(3):711–717. https://doi.org/10.1016/j.psychres
Naumann E, Tuschen-Caffier B, Voderholzer U, Caffier D, Svaldi J (2015) Rumination but not distraction increases eating-related symptoms in anorexia and bulimia nervosa. J Abnormal Psychol 124(2):412–420. https://doi.org/10.1037/abn0000046
Nicola M, O’Neill N, Sohrabi C, Khan M, Agha M, Agha R (2020) Evidence based management guideline for the COVID-19 andemic - review article. Int J Surg. https://doi.org/10.1016/j.ijsu.2020.04.001
Orgilés M, Morales A, Delvecchio E, Mazzeschi C, Espada J (2020) Immediate psychological effects of the COVID-19 quarantine in youth from Italy and Spain. https://doi.org/10.31234/osf.io/qaz9w
Pierce M, Hope H, Ford T, Hatch S, Hotopf M, John A, Kontopantelis E, Webb R, Wessely S, McManus S, Abel KM (2020) Mental health before and during the COVID-19 pandemic: a longitudinal probability sample survey of the UK population. Lancet Psychiat 7:883–892
Polivy J, Herman CP (2002) Causes of eating disorders. Annual Rev Psychol 53(1):187–213. https://doi.org/10.1146/annurev.psych.53.100901.135103
Rasmusson G, Lydecker J, Coffino J, White MA, Grilo CM (2018) Household food insecurity is associated with binge-eating dis- order and obesity. Int J Eat Disord 52(1):28–35. https://doi.org/10.1002/eat.22990
Robertson M, Duffy F, Newman E, Prieto Bravo C, Ates HH, Sharpe H (2021) Exploring changes in body image, eating and exercise during the COVID-19 lockdown: A UK survey. Appetite 159:105062. https://doi.org/10.1016/j.appet.2020.105062
Roca M, Gili M, Garcia-Campayo J, García-Toro M (2013) Economic crisis and mental health in Spain. Lancet 382:1977–1978
Rodgers RF, Lombardo C, Cerolini S, Franko DL, Omori M, Fuller-Tyszkiewicz M et al (2020) The impact of the COVID-19 pandemic on eating disorder risk and symptoms. Int J Eat Disord. https://doi.org/10.1002/eat.23318
Ruth SW, Stephanie B, Jennifer JT (2020) Access to evidence-based care for eating disorders during the COVID-19 crisis. Int J Eat Disord 53:639–646
Serafini G, Parmigiani B, Amerio A, Aguglia A, Sher L, Amore M (2020) The psychological impact of COVID-19 on the mental health in the general population. QJM An Int J Med. https://doi.org/10.1093/qjmed/hcaa201
Shanahan L, Steinhoff A, Bechtiger L, Murray AL, Nivette A, Hepp U, Ribeaud D, Eisner M (2020) Emotional distress in young adults during the COVID-19 pandemic: evidence of risk and resilience from a longitudinal cohort study. Psychol Med 1–32. https://doi.org/10.1017/s003329172000241x
Simone M, Emery RL, Hazzard VM, Eisenberg ME, Larson N, Neumark-Sztainer D (2021) Disordered eating in a population-based sample of young adults during the COVID-19 outbreak. Int J Eat Disord. https://doi.org/10.1002/eat.23505
Smith BJ, Lim MH (2020) How the COVID-19 pandemic is focusing attention on loneliness and social isolation. Public Health Res Pract 30(2):e3022008
Temsah MH, Al-Sohime F, Alamro N, Al-Eyadhy A, Al-Hasan K, Jamal A, Al-Maglouth I, Aljamaan F, Al Amri M, Barry M, Al-Subaie S, Somily AM (2020) The psychological impact of COVID-19 pandemic on health care workers in a MERS-CoV endemic country. J Infect Public Health 13(6):877–882. https://doi.org/10.1016/j.jiph.2020.05.021
Termorshuizen JD, Watson HJ, Thornton LM, Borg S, Flatt RE, MacDermod CM, Harper LE, van Furth EF, Peat CM, Bulik CM (2020) Early impact of COVID-19 on individuals with self-reported eating disorders: A survey of ~1,000 individuals in the United States and the Netherlands. Int J Eat Disord 53(11):1780–1790. https://doi.org/10.1002/eat.23353
Tiggemann M, Raven M (1998) Dimensions of control in bulimia and anorexia nervosa: internal control, desire for cotrol, or fear of losing self-control? Eat Disord 6(1):65–71. https://doi.org/10.1080/10640269808249248
Touyz S, Lacey H, Hay P (2020) Eating disorders in the time of COVID-19. J Eat Disord 8(19). https://doi.org/10.1186/s40337-020-00295-3
Trott M, Johnstone J, Pardhan S, Barnett Y, Smith L (2021) Changes in body dysmorphic disorder, eating disorder, and exercise addiction symptomology during the COVID-19 pandemic: a longitudinal study of 319 health club users. Psychiatry Res 298:113831. https://doi.org/10.1016/j.psychres.2021.113831
Walsh O, McNicholas F (2020) Assessment and management of anorexia nervosa during COVID-19. Irish J Psychol Med 37(3):187–191. https://doi.org/10.1017/ipm.2020.60
Wang C, Pan R, Wan X, Tan Y, Xu L, Ho CS et al (2020a) Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health 17(5):1729. https://doi.org/10.3390/ijerph17051729
Wang G, Zhang Y, Zhao J, Zhang J, Jiang F (2020b) Mitigate the effects of home confinement on children during the COVID-19 outbreak. Lancet 395(10228):945–947. https://doi.org/10.1016/S0140-6736(20)30547-X
Weissman RS, Bauer S, Thomas JJ (2020) Access to evidence- based care for eating disorders during the COVID-19 crisis. Int J Eat Disord 53(5):369–376. https://doi.org/10.1002/eat.23279
Wells G, Shea B, O’connell D et al (2000) The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Department of Epidemiology and Community Medicine, University of Ottawa, Canada. University of Ottawa, Canada
Whiteside SP, Lynam D, Miller J, Reynolds S (2005) Validation of the UPPS Impulsive Behavior Scale: a four factor model of impulsivity. Eur J Pers 19:559–574
Williamson DA, White MA, York-Crowe E, Stewart TM (2004) Cognitive- behavioral theories of eating disorders. Behavior Modific 28(6):711–738. https://doi.org/10.1177/0145445503259853
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions None of the authors have received funding for this study.
Author information
Authors and Affiliations
Contributions
Yunqi Gao contributed to data collection, analysis and interpretation of results, and wrote the draft manuscript. Nasser Bagheri and Luis Furuya-Kanamori were involved in planning and supervised the work. All authors reviewed the results and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare that they have no conflicts of interest.
Ethics approval
Not applicable.
Consent to participate
Not applicable.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gao, Y., Bagheri, N. & Furuya-Kanamori, L. Has the COVID-19 pandemic lockdown worsened eating disorders symptoms among patients with eating disorders? A systematic review. J Public Health (Berl.) 30, 2743–2752 (2022). https://doi.org/10.1007/s10389-022-01704-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10389-022-01704-4