
Abstract
Background
Esophagectomy is a highly invasive procedure for patients aged > 70 years. Here, we compared the actual nutritional status of older and younger patients who underwent esophagectomy.
Methods
A total of 118 patients who underwent radical esophagectomy between April 2013 and December 2016 were enrolled and divided into two groups based on age: group A (n = 41; ≥ 70 years) and group B (n = 77; < 70 years). Data pertaining to body mass index and nutritional variables (albumin; total cholesterol; cholinesterase; and prealbumin) were retrospectively analyzed preoperatively and at 3, 6, and 12 months postoperatively.
Results
Significant preoperative between-group differences were found in the cholinesterase, albumin, and prealbumin levels. The body mass index gradually decreased over the first 12 months after surgery in both groups, without significant between-group differences. Significant differences were observed in prealbumin and cholinesterase levels at 3 months postoperatively. 1 year postoperatively, both groups showed slight improvements; however, the between-group differences were not statistically significant. Group A had a significantly lower amount of the degree of decrement of BMI and chE than group B.
Conclusion
Thus, patients aged > 70 years can recover within 12 months of esophagectomy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Esophageal cancer predominantly affects elderly individuals, and its incidence peaks after 65 years of age. The number of elderly patients (age ≥ 70 years) undergoing esophagectomy has increased with the increasing global life expectancy. In a study involving 2315 patients who underwent esophagectomy, 30 and 5% were aged ≥ 70 and > 80 years, respectively [1].
Radical esophagectomy is a highly invasive procedure; it results in reduced dietary intake and poor nutritional status. It is associated with several complications occurring more frequently in patients aged > 70 years. After esophagectomy, feeding patients can be challenging. Previous studies have reported decreased nutritional intake and persistent weight loss, even over the long term, in patients who underwent esophagectomy [2, 3].
On average, patients who underwent esophagectomy have been reported to experience 10% loss in their body weight during the first year postoperatively [2], and the nutritional quality maintained by these patients is strongly linked to quality of life, response to future treatments, and survival [4,5,6,7,8,9]. Recently, surgical techniques and postoperative management have improved; hence, esophagectomy is becoming more acceptable for patients > 70 years. However, there is a lack of information on the long-term and specific nutritional status of late-elderly patients after esophagectomy. We compared the actual nutritional status of older (age ≥ 70 years) and younger (age < 70 years) patients after esophagectomy.
Materials and methods
This retrospective study was conducted at the Shizuoka Cancer Center, Japan. The independent medical ethics committee of the institute approved this study and waived off the need for informed consent because of the study’s retrospective and observational design.
Between April 2013 and December 2016, we examined the medical records of 118 patients who underwent esophagectomy with gastric replacement for long-term nutritional assessment. Patients with recurrent disease were excluded, and some patients were lost to follow-up. After esophagectomy, surgeons performed reconstruction that resulted in a completely vertical, tubularized stomach via the retrosternal route with an anastomosis at the cervical location. A jejunostomy tube was inserted from the gastric tube through the jejunum in patients with gastric tube reconstructions. Nutritional support provided via tube feeding with a semi-digested nutrition agent commenced on postoperative day 1. The dose was gradually increased. After discharge, the patients received injections of a semi-digested nutrition agent (250 mL/300 kcal/day) until 3 months postoperatively.
The patients were divided into two groups according to age: group A (n = 41; age, ≥ 70 years) and group B (n = 77; age, < 70 years). Data pertaining to body mass index (BMI) and the levels of nutritional variables (albumin, ALB; total cholesterol, TC; cholinesterase, chE; and preALB) were retrospectively collected preoperatively and at 3, 6, and 12 months postoperatively. The extent of changes in BMI and preALB levels at 3, 6, and 12 months postoperatively was also assessed.
We used medians and 25th percentile, 75th percentile as descriptive statistics, and statistical significance was considered with a p value less than 0.05. Data for our univariate analysis were tested using the Pearson’s Chi-square test, Fisher’s exact test, Mann–Whitney U test, and repeated-measure analysis of variance as appropriate.
Results
Baseline characteristics
Group A comprised 30 men and 11 women (median age, 72 years), whereas group B comprised 65 men and 12 women (median age, 62 years). The median preoperative BMIs were 20.7 (19.2, 22.3) kg/m2 and 21.6 (19.8, 23.6) kg/m2 for groups A and B, respectively, and these were not significantly different at baseline. Although both groups showed several pathological disease stages, we found no significant between-group differences. In both groups, thoracoscopy was more frequently performed than thoracotomy; however, there was no significant difference between the two groups with respect to frequency. Regarding preoperative therapy, 24 patients (58.5%) had chemo (radio)therapy in group A and 57 patients (74.0%) had the same in group B; however, there was no significant difference (Table 1, Fisher’s exact test and Pearson’s Chi-square test, Mann–Whitney U test).
Nutritional status
We found no significant between-group differences in the preoperative BMI levels. However, there were significant between-group differences in preoperative preALB and chE levels. BMIs declined gradually until 1 year postoperatively in both groups (group A, 19.0 (17.4, 19.8) kg/m2; group B, 18.9 (17.6, 20.4) kg/m2), without significant between-group differences. (Table 2, Fig. 1, Mann–Whitney U test).

Change in body mass index. This figure shows the median BMI. There were no significant between-group differences at any time point. BMI body mass index
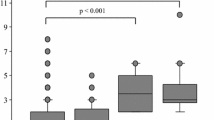
Regarding laboratory nutritional data, ALB and TC levels were almost normal pre- and postoperatively in both groups and no significant between-group differences were observed. There were significant between-group differences in preALB (group A, 18.2 (15.4, 20.9) mg/dL; group B, 21.3 (19.1, 24.2) mg/dL; p < 0.05) and chE (group A, 219 (214, 301) IU/L; group B, 241 (214, 300) IU/L; p < 0.05) levels at 3 months postoperatively. However, the values gradually improved in both groups, reaching normal levels by 1 year postoperatively. Furthermore, there were no significant between-group differences in preALB and chE levels at 6 and 12 months postoperatively (Table 2; Fig. 2, Mann–Whitney U test). In regard to the degree of decrement of BMI, preALB, and chE, group A had a significantly lower amount of decrement of BMI and chE than group B (BMI df = 1, F = 289, p < 0.05; chE df = 1, F = 35.6, p < 0.05), and there was no significant difference in the decrement of preALB between both groups (df = 1, F = 15.4, p = 0.06) (Table 3, repeated-measure analysis of variance).

Change in prealbumin. This figure depicts the median values before and after surgery. There is a significant difference preoperatively and at 3 months postoperatively. PreALB prealbumin. *p value < 0.05
Discussion
The global life expectancy is increasing; hence, we anticipate that by 2050 at least 16% of the world’s population will be aged ≥ 65 years [10]. According to the American Geriatrics Society, individuals aged ≥ 75 years are considered “elderly” [11]. In Japan, people aged ≥ 70 years constituted 18.7% of the entire population in 2016. Studies have reported on the rates of postoperative complications, hospital stay duration, short-term morbidity and mortality, and 5-year overall and disease-specific survival in elderly patients [12,13,14,15]. Wright et al. reported that compared with patients aged 55–74 years, those aged ≥ 75 years display worse outcomes [1]. Although esophagectomy can be justified in patients aged 70–79 years owing to low mortality in this age group, Luis et al. reported a significant increase in the major complications after esophagectomy in patients > 80 years [16].
On average, patients who underwent esophagectomy have been reported to experience 10% loss in their body weight during the first year postoperatively [2, 4]. Nutrition following upper gastrointestinal surgery is related to postoperative treatment, survival rate, and quality of life [5, 8, 17, 18]. In contrast, a study including some nutritional scores has reported nutritional status until 6 months postoperatively [19].
Here, we calculated the actual changes in the nutritional status of elderly patients. Patients’ BMIs decreased gradually until 1 year postoperatively, and preALB levels reached nadir at 3 months postoperatively; thus, the time points at which BMI and preALB values were at their minimum did not coincide. Total energy intake was the lowest at 3 months after a major upper gastrointestinal surgery [19]. preALB levels reflect recent dietary intake much more closely than the overall nutritional status [20], which explains the perceived gap.
There were no significant between-group differences in BMI preoperatively; however, preoperative preALB and chE levels were higher in group B than in group A. This might be so because there were more patients demonstrating slight nutritional excess in group B. The difference persisted for 3 months postoperatively, and the levels in both groups became similar at 6 and 12 months postoperatively. It is still possible that older patients are more affected by highly invasive operations, such as esophagectomy, in terms of food intake early after esophagectomy; however, the impact of those operations does not seem to be higher than that observed in younger patients over time.
chE levels were also nadir at 3 months postoperatively but remained at relatively normal levels at other times. TC and ALB levels were normal at all times and are, therefore, not suitable nutritional indices after esophagectomy.
BMI and preALB levels did not decrease as much as expected in patients aged > 70 years. This suggests that the semi-digestion nutrition agent on the enteral feeding tube, which was applied until 3 months postoperatively, led to a decline in the expected levels of reduction of these parameters.
1 year postoperatively, BMI and all nutritional variable levels were almost within normal ranges, even in patients aged > 70 years. Moreover, these patients had an even lower degree of decrement of BMI and chE than younger patients postoperatively. Of course, it is partly because younger patients had much higher BMI and chE levels preoperatively; however, this result indicates that even elder patients experience enough recovery after esophagectomy, within the first 12 months, which is beyond expectation.
There are some limitations to this study. First, this retrospective study was conducted at a single center and was limited to the Japanese population. Also, we have extensive experience and frequently perform esophagectomies due to the higher local incidence of esophageal cancer. Moreover, our outcomes may not be applicable to centers in other countries.
In conclusion, provided appropriate eligibility criteria are maintained, even patients aged > 70 years can overcome esophagectomy and regain significant strength within 12 months postoperatively.
References
Wright CD, Kucharczuk JC, O’Brien SM, et al. Society of thoracic surgeons general thoracic surgery database. Predictors of major morbidity and mortality after esophagectomy for esophageal cancer: a society of thoracic surgeons general thoracic surgery database risk adjustment model. J Thorac Cardiovasc Surg. 2009;137:587–95.
Martin L, Lagergren P. Long-term weight change after oesophageal cancer surgery. Br J Surg. 2009;96:1308–14.
Internullo E, Moons J, Nafteux P, et al. Outcome after esophagectomy for cancer of the esophagus and GEJ in patients over 75 years. Eur J Cardiothorac Surg. 2008;33:1096–104.
Carey S, Storey D, Biankin AV, et al. Long term nutritional status and quality of life following major upper gastrointestinal surgery: a cross-sectional study. Clin Nutr. 2011;30:774–9.
Bae J, Kim S, Kim Y, et al. Health-related quality of life among disease-free stomach cancer survivors in Korea. Qual Life Res. 2006;15:1587–96.
Conroy T, Uwer L, Deblock M. Health-related quality-of-life assessment in gastrointestinal cancer: are results relevant for clinical practice? Curr Opin Oncol. 2007;19:401–6.
Huang JJ, Yeo CJ, Sohn TA, et al. Quality of life and outcomes after pancreaticoduodenectomy. Ann Surg. 2000;231:890–8.
Senesse P, Assenat E, Schneider S, et al. Nutritional support during oncologic treatment of patients with gastrointestinal cancer: who could benefit? Cancer Treat Rev. 2008;34:568–75.
Yu W, Seo Y, Chung H. Postoperative body weight loss and survival after curative resection for gastric cancer. Br J Surg. 2002;89:467–70.
United Nations. Department of Economic and Social Affairs, Population Division. In: World Population to 2300. New York: United Nations. 2004. http://www.un.org/esa/population/publications/longrange2/WorldPop2300final.pdf. Accessed December 2012.
LoCicero J III, Shaw PJ. Thoracic surgery in the elderly: areas of future research studies. Thorac Surg Clin. 2009;19:409–13.
Cijs TM, Verhoef C, Steyerberg EW, et al. Outcome of esophagectomy for cancer in elderly patients. Ann Thorac Surg. 2010;90:900–7.
Morita M, Egashira A, Yoshida R, et al. Esophagectomy in patients 80 years of age and older with carcinoma of the thoracic esophagus. J Gastroenterol. 2008;43:345–51.
Pultrum BB, Bosch DJ, Nijsten MW, et al. Extended esophagectomy in elderly patients with esophageal cancer: minor effect of age alone in determining the postoperative course and survival. Ann Surg Oncol. 2010;17:1572–80.
Fang W, Igaki H, Tachimori Y, et al. Three field lymph node dissection for esophageal cancer in elderly patients over 70 years of age. Ann Thorac Surg. 2001;72:867–71.
Tapias LF, Muniappan A, Wright CD, et al. Short and long-term outcomes after esophagectomy for cancer in elderly patients. Ann Thorac Surg. 2013;95:1741–8.
Conroy T, Uwer L, Deblock M. Health-related quality-of-life assessment in gastrointestinal cancer: are results relevant for clinical practice? Curr Opin Oncol. 2007;19:401–6.
Huang JJ, Yeo CJ, Sohn TA, et al. Quality of life and outcomes after pancreaticoduodenectomy. Ann Surg. 2000;231:890–8.
Carey S, Ferrie S, Ryan R, et al. Long-term nutrition intervention following major upper gastrointestinal surgery: a prospective randomized controlled trial. Eur J Clin Nutr. 2013;67:324–9.
Devoto G, Gallo F, Marchello C, et al. Prealbumin serum concentrations as a useful tool in the assessment of malnutrition in hospitalized patients. Clin Chem. 2006;52:2281–5.
Funding
This research did not receive any specific funding from agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Statement
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions.
Conflict of interest
The authors declare that they have no conflicts of interest.
Informed consent
Informed consent or substitute for it was obtained from all patients for being included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Ishii, K., Tsubosa, Y., Niihara, M. et al. Changes in the nutritional status of elderly patients after esophagectomy. Esophagus 16, 408–412 (2019). https://doi.org/10.1007/s10388-019-00681-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10388-019-00681-0