
Abstract
Background
Radical esophagectomy for esophageal cancer is associated with high morbidity, especially with pulmonary complications. Mediastinoscopic esophagectomy via a small left neck incision combined with the esophageal hiatus, without using transthoracic approach, has been reported to reduce pulmonary complication; however, from technical point of view, this approach using non-articulating, straight, long forceps is extremely challenging, especially in the middle mediastinal area. Its technical difficulties may be attenuated using da Vinci Surgical System. The aim of this study was to evaluate the feasibility and safety of robot-assisted mediastinoscopic esophagectomy.
Methods
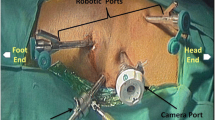
Robot-assisted mediastinoscopic esophagectomy was performed in six patients between October 2016 and May 2017. Robotic esophageal mobilization with upper and middle mediastinal lymphadenectomy was performed via the three da Vinci Xi (Intuitive Surgical, Inc. Sunnyvale, CA) trocars placed on the 5-cm left cervical incision. Thereafter, the remaining part of radical esophagectomy was completed via a transhiatal approach.
Results
Upper and middle mediastinal lymphadenectomy was robotically completed via the transcervical approach in all cases without conversion to transthoracic approach. No postoperative complications (Clavien–Dindo classification grade ≥ III) were observed.
Conclusions
Robot-assisted mediastinoscopic esophagectomy was technically feasible and safe. Use of da Vinci Surgical System may help attenuate technical difficulties in transcervical middle mediastinal lymph node dissection.




Similar content being viewed by others


References
Fujita H, Sueyoshi S, Tanaka T, et al. Three-field dissection for squamous cell carcinoma in the thoracic esophagus. Ann Thorac Cardiovasc Surg. 2002;8:328–35.
Kato K, Muro K, Minashi K, et al. Gastrointestinal oncology study group of the Japan clinical oncology. Phase II study of chemoradiotherapy with 5-fluorouracil and cisplatin for stage II–III esophageal squamous cell carcinoma: JCOG trial (JCOG 9906). Int J Radiat Oncol Biol Phys. 2011;81:684–90.
Gockel I, Heckhoff S, Messow CM, et al. Transhiatal and transthoracic resection in adenocarcinoma of the esophagus: does the operative approach have an influence on the long-term prognosis? World J Surg Oncol. 2005;3:40.
Bakhos CT, Fabian T, Oyasiji TO, et al. Impact of the surgical technique on pulmonary morbidity after esophagectomy. Ann Thorac Surg. 2012;93:221–6.
Akaishi T, Kaneda I, Higuchi N, et al. Thoracoscopic en bloc total esophagectomy with radical mediastinal lymphadenectomy. J Thorac Cardiovasc Surg. 1996;112:1533–40.
Luketich JD, Alvelo-Rivera M, Buenaventura PO, et al. Minimally invasive esophagectomy: outcomes in 222 patients. Ann Surg. 2003;238:486–94.
Biere SS, van Berge Henegouwen MI, et al. Minimally invasive versus open oesophagectomy for patients with oesophageal cancer: a multicentre, open-label, randomised controlled trial. Lancet. 2012;379:1887–92.
Suda K, Ishida Y, Kawamura Y, et al. Robot-assisted thoracoscopic lymphadenectomy along the left recurrent laryngeal nerve for esophageal squamous cell carcinoma in the prone position: technical report and short-term outcomes. World J Surg. 2012;36:1608–16.
Parker M, Bowers SP, Goldberg RF, et al. Transcervical videoscopic esophageal dissection during two-field minimally invasive esophagectomy: early patient experience. Surg Endosc. 2011;25:3865–9.
Watanabe M, Yoshida N, Karashima R, et al. Transcervical superior mediastinal lymph node dissection combined with transhiatal lower esophageal dissection before transthoracic esophagectomy: a safe approach for salvage esophagectomy. J Am Coll Surg. 2009;208:e7–9.
Horgan S, Berger RA, Elli EF, et al. Robotic-assisted minimally invasive transhiatal esophagectomy. Am Surg. 2003;69:624–6.
Pop D, Venissac N, Mouroux J. Video-assisted mediastinoscopy improved radical resection for cancer in transhiatal esophagectomy. J Thorac Cardiovasc Surg. 2007;133:267–8.
Mori K, Yamagata Y, Wada I, et al. Robotic-assisted totally transhiatal lymphadenectomy in the middle mediastinum for esophageal cancer. J Robot Surg. 2013;7:385–7.
Fujiwara H, Shiozaki A, Konishi H, et al. Single-port mediastinoscopic lymphadenectomy along the left recurrent laryngeal nerve. Ann Thorac Surg. 2015;100:1115–7.
Fujiwara H, Shiozaki A, Konishi H, et al. Hand-assisted laparoscopic transhiatal esophagectomy with a systematic procedure for en bloc infracarinal lymph node dissection. Dis Esophagus. 2016;29:113–31.
Fujiwara H, Shiozaki A, Konishi H, et al. Perioperative outcomes of single-port mediastinoscope-assisted transhiatal esophagectomy for thoracic esophageal cancer. Dis Esophagus. 2017;30:1–8.
Suda K, Man IM, Ishida Y, et al. Potential advantages of robotic radical gastrectomy for gastric adenocarcinoma in comparison with conventional laparoscopic approach: a single institutional retrospective comparative cohort study. Surg Endosc. 2015;29:673–85.
Mori K, Yamagata Y, Aikou S, et al. Short-term outcomes of robotic radical esophagectomy for esophageal cancer by a nontransthoracic approach compared with conventional transthoracic surgery. Dis Esophagus. 2016;29:429–34.
Boone J, Borel Rinkes IH, van Hillegersberg R. Transhiatal robot-assisted esophagectomy. Surg Endosc. 2008;22:1139–40.
Mori K, Yoshimura S, Yamagata Y, et al. Preclinical study of transcervical upper mediastinal dissection for esophageal malignancy by robot-assisted surgery. Int J Med Robot. 2017;13:e1750.
Rice TW, Blackstone EH, Rusch VW. 7th edition of the AJCC Cancer Staging Manual: esophagus and esophagogastric junction. Ann Surg Oncol. 2010;17:1721–4.
Clavien PA, Barkun J, de Oliveira ML, et al. The Clavien-Dindo classification of surgical complications: 5-year experience. Ann Surg. 2009;250:187–96.
Japan Esophageal Society. Japanese classification of esophageal cancer: part I. Esophagus. 2017;14:1–36.
Japan Esophageal Society. Japanese classification of esophageal cancer: part II and III. Esophagus. 2017;14:37–65.
Kurokawa Y, Sasako M, Sano T, Japan Clinical Oncology Group, et al. Ten-year follow-up results of a randomized clinical trial comparing left thoracoabdominal and abdominal transhiatal approaches to total gastrectomy for adenocarcinoma of the oesophagogastric junction or gastric cardia. Br J Surg. 2015;102:341–8.
Hulscher JB, van Sandick JW, de Boer AG, et al. Extended transthoracic resection compared with limited transhiatal resection for adenocarcinoma of the esophagus. N Engl J Med. 2002;347:1662–9.
Junginger T, Gockel I, Heckhoff S. A comparison of transhiatal and transthoracic resections on the prognosis in patients with squamous cell carcinoma of the esophagus. Eur J Surg Oncol. 2006;32:749–55.
Ruurda JP, van der Sluis PC, van der Horst S, et al. Robot-assisted minimally invasive esophagectomy for esophageal cancer: a systematic review. J Surg Oncol. 2015;112:257–65.
Park SY, Kim DJ, Jung HS. Robot-assisted thoracoscopic esophagectomy with extensive mediastinal lymphadenectomy: experience with 114 consecutive patients with intrathoracic esophageal cancer. Dis Esophagus. 2016;29:326–32.
Gockel I, Kneist W, Keilmann A, et al. Recurrent laryngeal nerve paralysis (RLNP) following esophagectomy for carcinoma. Eur J Surg Oncol. 2005;31:277–81.
Swanson SJ, Batirel HF, Bueno R, et al. Transthoracic esophagectomy with radical mediastinal and abdominal lymph node dissection and cervical esophagogastrostomy for esophageal carcinoma. Ann Thorac Surg. 2001;72:1918–24.
Scholtemeijer MG, Seesing MFJ, Brenkman HJF, et al. Recurrent laryngeal nerve injury after esophagectomy for esophageal cancer: incidence, management, and impact on short- and long-term outcomes. J Thorac Dis. 2017;9:S868–78.
Acknowledgements
The authors are indebted to Maruzen CO., LTD. (Tokyo, Japan) for their native English speaker’s review of this manuscript. Intuitive Surgical, Inc. provided the necessary laboratory support in the preclinical cadaver study.
Funding
This work was not supported by any grants or funding. All authors have no commercial association or financial involvement that might pose a conflict of interest in connection with the submitted article.
Author information
Authors and Affiliations
Contributions
MN: assistant of surgeon, acquisition of data, drafting of manuscript. IU: operating surgeon, drafting and revision of manuscript. KS: drafting and revision of manuscript. SS: assistant of surgeon, drafting of manuscript. KK: assistant of surgeon, drafting of manuscript. SK: assistant of surgeon, drafting of manuscript. YI: drafting and revision of manuscript. KI: assistant of surgeon, drafting and revision of manuscript.
Corresponding author
Ethics declarations
Ethical statement
This study was approved by the institutional review board of Fujita Health University. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions.
Conflict of interest
This work was not supported by any grants or funding. Masaya Nakauchi, Ichiro Uyama, Koichi Suda, Susumu Shibasaki, Kenji Kikuchi, Shinichi Kadoya, Yoshinori Ishida, and Kazuki Inaba have no conflicts of interest or financial ties to disclose.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Nakauchi, M., Uyama, I., Suda, K. et al. Robot-assisted mediastinoscopic esophagectomy for esophageal cancer: the first clinical series. Esophagus 16, 85–92 (2019). https://doi.org/10.1007/s10388-018-0634-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10388-018-0634-8