
Abstract
Purpose
Completion rate is the most commonly used index of quality in colonoscopy, and yet a complete examination is not necessarily a good examination. The ability to detect and treat adenomas is an important component of endoscopic skill, because many colonoscopies are performed for this express purpose. Adenoma detection rate is rarely reported, although it seems to depend on the time taken for withdrawal. The literature suggests that adenomas should be detected in approximately 25 percent of men and 15 percent of women older than age 50 years. We have reviewed the adenoma detection rates of six colorectal surgeons to provide insight into the range of adenoma detection rates and the factors that influence them.
Methods
A prospective departmental colonoscopy database was queried. Colonoscopy completion rates, adenoma detection rates, and times of insertion and withdrawal were noted and stratified by the six staff colonoscopists. Adenoma detection rates were tabulated for the four common indications for colonoscopy.
Results
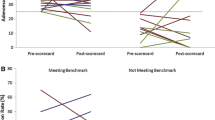
Each staff endoscopist performed >250 examinations per year and had performed >1,000 total examinations. Although completion rates are fairly uniform (mean, 96.5 (range, 94.8–97.9) percent), there is a wide range of ADR, especially when adenomas are common (polyp or cancer surveillance; range, 14.2–27.4 percent). With the exclusion of one outlier staff, regression of withdrawal time against adenoma detection rate produced an r2 of 0.975 (P = 0.0016).
Conclusions
Adenoma detection rate is independent of completion rate as a colonoscopy quality indicator. There is a wide range of adenoma detection rates among experienced colorectal surgeons. Colonoscopists need to be aware of their adenoma detection rate.

Similar content being viewed by others


References
Rex DK, Johnson DA, Lieberman DA, et al. Colorectal cancer prevention 2000: screening recommendations of the American College of Gastroenterology. Am J Gastroenterol 2000;95:868–77.
Rex DK, Petrini JL, Baron TH, et al. ASGE/ACG Taskforce on Quality in Endoscopy. Quality indicators for colonoscopy. Am J Gastroenterol 2006;101:873–85.
Rex DK, Bond JH, Winawer S, et al. Quality in the technical performance of colonoscopy and the continuous improvement process for colonoscopy: recommendations of the US Multi-Society Task Force on Colorectal Cancer. Am J Gastroenterol 2002;97:1297–308.
Wietlisbach V, Burnand B, Vader JP, et al. Variations in technical performance and quality of use of colonoscopy throughout Europe: the EPAGE multicenter study. Gastrointest Endosc 2002;55:AB82–2.
Aslinia F, Uradomo L, Steele A, et al. Quality assessment of colonoscopic cecal intubation: an analysis of 6 years of continuous practice at a university hospital. Am J Gastroenterol 2006;101:721–31.
Rex DK. Quality in colonoscopy: cecal intubation first, then what? Am J Gastroenterol 2006;101:732–4.
Rex DK, Lehman GA, Ulbright TM, et al. Colonic neoplasia in asymptomatic persons with negative fecal occult blood tests: influence of age, gender, and family history. Am J Gastroenterol 1993;88:825–31.
Johnson DA, Gurnery MS, Vople RJ, et al. A prospective study of the prevalence of colonic neoplasms in asymptomatic patients with an age-related risk. Am J Gastroenterol 1990;85:969–74.
Lieberman DA, Weiss DG, Bond JH, et al. Use of colonoscopy to screen asymptomatic adults for colorectal cancer. N Engl J Med 2000;343:162–8.
Rex DK. Colonoscopic withdrawal technique is associated with adenoma miss rates. Gastrointest Endosc 2000;51:33–6.
Atkin W, Rogers P, Cardwell C, et al. Wide variation in adenoma detection rates at screening flexible sigmoidoscopy. Gastroenterology 2004;126:1247–56.
Sanchez W, Harewood GC, Petersen BT. Evaluation of polyp detection in relation to procedure time of screening or surveillance colonoscopy. Am J Gastroenterol 2004;99:1941–5.
Barclay RL, Vicari JJ, Doughty AS, Johanson JF, Greenlaw RL. Colonoscopic withdrawal times and adenoma detection during screening colonoscopy. N Engl J Med 2006;355:2533–41.
Lieberman DA, Smith FW. Screening for colon malignancy with colonoscopy. Am J Gastroenterol 1991;86:946–51.
Lieberman DA, Weiss DG, Bond JH, et al. Use of colonoscopy to screen asymptomatic adults for colorectal cancer: Veterans Affairs Cooperative Study Group 380. N Engl J Med 2000;343:162–8.
Imperiale T, Wagner D, Lin C, et al. Risk of advanced proximal neoplasms in asymptomatic adults according to the distal colorectal findings. N Engl J Med 2000;343:169–74.
Schoenfeld P, Cash B, Flood A, et al. Colonoscopic screening of average-risk women for colorectal neoplasia. N Engl J Med 2005;352:2061–8.
Chen S, Rex DK. Endoscopist is comparable to age and gender as predictor of adenomas at colonoscopy. Am J Gastroenterol 2005;100(Suppl):S393.
Rex D, Cutler CS, Lemmel GT, et al. Colonoscopic miss rates of adenomas determined by back-to-back colonoscopies. Gastroenterology 1997;112:24–8.
Author information
Authors and Affiliations
Corresponding author
Additional information
Read at the meeting of The American Society of Colon and Rectal Surgeons, Seattle, Washington, June 3 to 7, 2006.
Reprints are not available.
About this article
Cite this article
Millan, M.S., Gross, P., Manilich, E. et al. Adenoma Detection Rate: The Real Indicator of Quality in Colonoscopy. Dis Colon Rectum 51, 1217–1220 (2008). https://doi.org/10.1007/s10350-008-9315-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10350-008-9315-3