
Abstract
A rare case of acute avulsion of both posterior meniscal roots concomitant with an acute anterior cruciate ligament (ACL) tear in a professional soccer player is described. While avulsion of the lateral meniscal root has been extensively reported in association with ACL injuries, medial root avulsion has never been reported in association with acute ACL. A review of the video documentation of the match accident revealed the exact mechanism of injury was a forceful external rotation of the standing limb.
Similar content being viewed by others

Introduction
Root tears are a subset of meniscal injuries, which have become increasingly recognized as a cause of pain and impaired mobility. The root serves as the anchor point for the menisci. Occurring on either the medial or lateral meniscus, root tears refer to a radial tear or avulsion at the posterior horn attachment to the bone. Both radial tear and posterior horn avulsion defunction the menisci as load-bearing structures, with increasing local contact pressure and premature onset of knee arthritis [9]. Because the medial and lateral menisci differ in anatomy and biomechanics, the pathogenesis of posterior root avulsions is also different. Tearing of the lateral posterior meniscal root is traumatic and always associated with anterior cruciate ligament (ACL) injury [1, 22], while the medial posterior root [2, 8, 10, 19] is prone to chronic degenerative meniscal disease.
To date, only one case [15] has been reported of radial tear of both roots detected two years after an ACL injury. The authors hypothesised a traumatic origin for avulsion of the lateral meniscus and a degenerative origin for the medial meniscus.
Here, we describe a rare case of avulsion of both posterior roots in association with an acute ACL tear in a professional soccer player. A review of the video documentation of the match accident revealed the exact mechanism of injury.
Case report
A 20-year-old professional soccer player reported sustaining a forceful rotatory left knee injury during an official match of the Italian Second Division. The dynamics of the accident could be clearly followed on the video recording of the match. While the player was standing with one foot fixed on the field and the contralateral limb elevated for shooting the ball, a player from the opponent team collided into the elevated limb, causing a forceful external rotation of the standing limb.
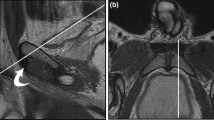
At presentation two days after the injury, physical examination revealed signs of acute anterior laxity and pain was elicited over both lateral and medial joint lines. Full flexion was painful and restricted by knee swelling. Manual knee laxity tests, including the Lachman test, anterior drawer test and pivot shift test, were positive, as was the McMurray test. Measurement using a KT-2000 arthrometer (MEDmetric Corporation, San Diego, CA, USA) demonstrated a 5-mm side-to-side difference. Preoperative radiographic evaluation was normal. Magnetic resonance imaging (MRI) disclosed acute rupture of the ACL and tears in the roots of the posterior horns of both lateral and medial menisci (Fig. 1). Arthroscopic evaluation under regional anesthesia revealed an acute tear of the ACL at its midsubstance. Avulsion of the posterior root of the lateral meniscus was present in addition to acute avulsion at the posterior root of the medial meniscus with posterior displacement (Figs. 2, 3). No other intra-articular lesions were detected.

a Preoperative coronal TSE-fat saturated MR image shows the ACL tear and an area of heterogeneous intrameniscal signal intensity of both meniscal roots with a void at the posterior attachment site of both menisci (arrow). b Preoperative coronal oblique 30° MR image. The arrow shows absence of tibial insertion of posterior lateral root. The asterisk shows hyperintensity signal at femoral ACL insertion

Arthroscopic view of acute medial posterior root avulsion

Arthroscopic view of acute lateral posterior root avulsion
Treatment consisted of arthroscopic pullout suturing of both menisci and ACL reconstruction with an autologous bone-patellar tendon-bone graft. A transeptal approach was used for the medial meniscus root suture. The flat tip of an ACL guide (Arthrex, Naples, FL, USA) was introduced through the anterolateral portal at the footprint of the posterior root of the previously abraded medial meniscus. A tibial tunnel was made using a 2.9-mm guide pin from the anterolateral cortex of the proximal tibia to the footprint of the posterior root of the medial meniscus. Two nonabsorbable sutures were placed at the posterior root using a crescent-shaped suture hook. Both sutures ends were pulled out through the anterolateral cortex of the proximal tibia. The lateral meniscus was sutured in the same manner. The suture material for the lateral meniscus was pulled through the anteromedial cortex of the proximal tibia. The lateral and medial sutures were tied over two buttons after confirming sufficient reduction and tension.
Postoperatively, the knee was kept in full extension in a brace locked at 0° for four weeks. Passive motion was allowed after the first two weeks and active motion was restricted to 90° during the first four weeks. Partial weight bearing was permitted at four weeks postoperatively, followed by full weight bearing at six weeks. After six weeks closed-chain strengthening was begun, and full flexion exercises were allowed. During the second and the third month, strengthening exercises and hydrokinetic therapy were implemented. Running on a treadmill was started after two months and training on the field was permitted after four months. Six months postoperatively, the patient was able to return to play in an official match with full range of knee motion. At the last follow-up of one year, no meniscal signs and symptoms were present. Manual knee laxity tests, including the Lachman test, anterior drawer test and pivot shift test, were negative. The side-to-side difference was 0.4 mm, as measured by the KT-2000 manual maximal test. The postoperative MRI showed a good healing process of both roots (Fig. 4).

At MRI follow-up at three months, the coronal T1-TSE view (a) shows the tibial tunnel for ACL reconstruction and the tunnels for the medial root (white arrow) and for the lateral root (dashed arrow). b The coronal TSE-fat saturated MR image shows both medial and lateral roots healed
Discussion
The unusual finding in this case was avulsion of both posterior meniscal roots with a concomitant acute ACL tear. Medial posterior root avulsion usually results from chronic degenerative meniscal tears [2, 8, 10, 19] and is seldom associated with posterior cruciate ligament tears [14]. According to the radiological literature, the incidence of meniscal root tear is 8–9.8 % [3, 6, 20], whereas the orthopaedic literature reports a wider range between 6.7 % and 12.4 % [1, 9, 10]. This discrepancy stems from difficulties in radiographic diagnosis and in defining meniscal root tear. Two subcategories of meniscal root tear can be distinguished: root avulsion from the tibial plateau and meniscal posterior horn tear within 1 cm from the root. These tears are biomechanically similar because they can disrupt the circumferential fibers of the meniscus resulting in failure of the hoop strain mechanism [9, 11, 12]. Following rupture, the ability to resist extrusion under axial loading is definitely lost [4, 13].
In the only case described to date of a radial tear in both roots [15] concurrent with a chronic ACL tear, Lee et al. [15] postulated that the mechanism of injury was involvement of the posterior lateral root together with an ACL injury. The medial radial tear in the posterior root was caused by forceful mechanical stress secondary to instability. In the present case, avulsion of both meniscal roots was associated with an acute ACL tear. From a review of the video recording, the mechanism of injury was seen to be clearly due to forceful rotatory stress. As postulated by Park et al. [20], anterior tibial translation in an ACL injury may pull the lateral meniscus forward, stripping the meniscofemoral ligament away the meniscus attachment. The mechanism of medial meniscus root injury is more difficult to explain. Due to external rotation, for stress associated with compression axial load, the posterior horn is impinged by the femoral condyle. Markolf et al. [16] have shown that the anterior tibial force and the external tibial torque during knee loading produce relatively high posterior horn attachment forces, presumably by impinging the medial femoral condyle against the posterior meniscal rim.
In our patient, both meniscal roots were refixed with a transtibial technique. The sequelae of a medial root avulsion left in situ or misdiagnosed is functionally equivalent to total meniscectomy with meniscal extrusion and rapid progression to knee arthritis [17, 18]; however, there is no consensus on the treatment of lateral meniscal root tear. The fewer lateral meniscal tears in chronic versus acute ACL tears have led to conservative treatment of such lesions [5]. There are several reasons justifying this approach: concomitant ACL reconstruction creates blood clots and joint stability, increased blood supply to the posterior horn in comparison to the lateral meniscal pars intermedia, and absence of definitive clinical complaints when a lateral meniscus tear is left in situ. So, a radial or complex (radial and longitudinal) tear that occurs within 1 cm of the meniscal attachment may be more likely to heal spontaneously [7, 22]. Spontaneous healing after avulsion of the lateral root is less probable. The lateral meniscal root has two distinct insertions: one is anterior and attached to the posterior aspect of the tibial intercondylar eminence, and the other is posterior to and confluent with the meniscofemoral ligament. When root avulsion occurs, the latter insertion probably inhibits spontaneous healing because of continuous traction by the meniscofemoral ligament during knee movements. Recently, Schillamer et al. [21] demonstrated that posterior horn avulsion of the lateral meniscus causes peak tibiofemoral contact pressure to increase from 2.8 to 4.2 MPa, but that the peak pressure returns to normal after repair to bone via a transtibial tunnel.
In this rare case of tears in the roots of the posterior horns of both menisci, concomitant with an acute ACL tear, radiological and clinical outcome after surgery confirmed good healing. Both the lateral posterior horn and the medial posterior horn need to be considered when planning ACL reconstruction.
References
Ahn JH, Lee YS, Chang JY, Chang MJ, Eun SS, Kim SM (2009) Arthroscopic all inside repair of the lateral meniscus tear. Knee 16:77–80
Bin SI, Kim JM, Shin SJ (2004) Radial tears of the posterior horn of the medial meniscus. Arthroscopy 20:373–378
Brody JM, Lin HM, Hulstyn MJ, Tung GA (2006) Lateral meniscus root tear and meniscus extrusion with anterior cruciate ligament tear. Radiology 239:805–810
Choi C-J, Choi Y-J, Lee J-J, Choi C-H (2010) Magnetic resonance imaging evidence of meniscal extrusion in medial meniscus posterior root tear. Arthroscopy 26:1602–1606
Cipolla M, Scala A, Giannì E, Puddu G (1995) Different patterns of meniscal tears in acute anterior cruciate ligament (ACL) ruptures and in chronic ACL-deficient knees. Classification, staging and timing of treatment. Knee Surg Sports Traumatol Arthosc 3:130–134
De Smet AA, Blankenbaker DG, Kijowski R, Graf BK, Shinki K (2008) MR diagnosis of posterior root tears of the lateral meniscus using arthroscopy as the reference standard. Am J Radiol 192:480–486
Fitzgibbons RE, Shelbourne KD (1995) “Aggressive” nontreatment of lateral meniscal tears seen during anterior cruciate ligament reconstruction. Am J Sports Med 28:156–159
Habata T, Uematsu K, Hattori K, Takakura Y (2004) Clinical features of the posterior horn tear in the medial meniscus. Arch Orthop Trauma Surg 124:642–645
Han SB, Shetty GM, Lee DH, Chae DJ et al (2010) Unfavorable results of partial meniscectomy for complete posterior medial meniscus root tear with early osteoarthritis: a 5 to 8 year follow-up study. Arthroscopy 26:1326–1332
Hwang BY, Kim SL, Lee SW, Lee HE, Lee CK, Hunter DJ, Jung KA (2012) Risk factors for medial meniscus posterior root tear. Am J Sports Med. doi:10.1177/0363546512447792
Johannsen AM, Civitarese DM, Padalecki JR, Goldsmith MT, Wijdicks CA, LaPrade RF (2012) Qualitative and quantitative anatomic analysis of the posterior root attachments of the medial and lateral menisci. Am J Sports Med 40:2342–2347
Johnson DL, Swenson TM, Livesay GA, Fu FH, Harner CD (1995) Insertion-site anatomy of the human menisci: gross, arthroscopic, and topographical anatomy as a basis for meniscal transplantation. Arthroscopy 11:495–498
Jones RS, Keane GC, Learmonth DJ (1996) Direct measurement of hoop strains in the intact and torn human medial meniscus. Clin Biomech 11:295–300
Kim YJ, Kim JG, Chang SH, Shim JC, Kim JC, Lee MY (2010) Posterior root tear of the medial meniscus in multiple knee ligament injuries. Knee 17:324–328
Lee JH, Hwang BY, Lim YJ, Kim KH, Song JH (2009) Radial tears in the roots of the posterior horns of both the medial and lateral menisci combined with anterior cruciate ligament tear: a case report. Knee Surg Sport Traumatol Arthosc 17:1340–1343
Markolf KL, Jackson SR, McAllister DR (2012) Force measurements in the medial meniscus posterior horn attachment: effects on anterior cruciate removal. Am J Sports Med 40:332–338
Marzo JM, Gruske-De Perio J (2009) Effects of medial meniscus posterior avulsion and repair on tibiofemoral contact area and peak contact pressure with clinical implications. Am J Sports Med 37:124–129
Neogi DS, Kumar A, Rijal L, Yadav CS, Jaiman A, Nag HL (2013) Role of nonoperative treatment in managing degenerative tears of the medial meniscus posterior root. J Orthop Traumatol 14(3):193–199
Ozkoc G, Circi E, Gonc U, Irgit K, Pourbagher A, Tandogan R (2008) Radial tears in the root of the posterior horn of the medial meniscus. Knee Surg Sports Traumatol Arthosc 16:849–854
Park LS, Jacobson JA, Jamadar DA, Caoili E, Kalume M, Wojtys E (2007) Posterior horn lateral meniscus tear simulating meniscofemoral ligament attachment in the setting of ACL tear: MRI findings. Skelet Radiol 36:399–403
Schillamer CK, Werner FW, Scuderi MG, Cannizzaro JP (2012) Repair of lateral meniscus posterior horn detachment lesion. A biomechanical evaluation. Am J Sports Med 40:2604–2609
Shelbourne KD, Heinrich J (2004) The long term evaluation of lateral meniscus tears left in situ at the time of anterior cruciate ligament reconstruction. Arthroscopy 20:346–351
Conflict of interest
None.
Ethical standards
The patient provided his consent to the publication of this case report.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
About this article

Cite this article
Mariani, P.P., Iannella, G., Cerullo, G. et al. Avulsion of both posterior meniscal roots associated with acute rupture of the anterior cruciate ligament. J Orthopaed Traumatol 16, 259–262 (2015). https://doi.org/10.1007/s10195-014-0302-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10195-014-0302-2