
Abstract
Background
After kidney transplantation, fibroblast growth factor-23 (FGF-23) normally returns to baseline within 1 year whereas hyperparathyroidism persists in most kidney transplant (KT) recipients. As a result, serum phosphate remains relatively low in association with increased serum calcium and urinary phosphate excretion when compared to chronic kidney disease patients. The relationship between mineral metabolism and outcomes in long-term KT recipients has not been extensively studied. This study investigated whether the alteration in mineral metabolism influenced graft survival in long-term KT recipients.
Methods
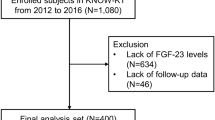
This study included 273 KT recipients after 1 year of transplantation. Mineral parameters were obtained at the time of enrolment and patients were followed prospectively for an average of 71 months.
Results
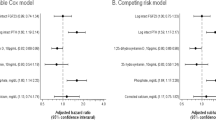
Graft loss (death-censored) occurred in 41 (15%) patients. In univariate analysis, deceased donor transplantation, decreased serum albumin and estimated glomerular filtration rate, increased serum phosphate, parathyroid hormone (PTH), FGF-23 and fractional excretion of phosphate (FePi) predicted future allograft loss. After adjustments for cardiovascular disease risk factors, donor type, dialysis vintage, serum albumin and allograft function, only increased PTH and FePi remained associated with the outcome. Relationships between increased serum phosphate and FGF-23 with graft survival were lost after adjustments. Adjusted survival curves revealed the association between PTH > 90 pg/mL and FePi > 20% with worse graft survival.
Conclusions
Hyperparathyroidism and increased FePi predicted allograft loss in long-term KT recipients.

Similar content being viewed by others

References
Bellasi A, Mandreoli M, Baldrati L, Corradini M, Di Nicolo P, Malmusi G, et al. Chronic kidney disease progression and outcome according to serum phosphorus in mild-to-moderate kidney dysfunction. Clin J Am Soc Nephrol. 2011;6(4):883–91. doi:10.2215/CJN.07810910.
Isakova T, Xie H, Yang W, Xie D, Anderson AH, Scialla J, et al. Fibroblast growth factor 23 and risks of mortality and end-stage renal disease in patients with chronic kidney disease. JAMA. 2011;305(23):2432–9. doi:10.1001/jama.2011.826.
Scialla JJ, Astor BC, Isakova T, Xie H, Appel LJ, Wolf M. Mineral metabolites and CKD progression in African Americans. J Am Soc Nephrol. 2013;24(1):125–35. doi:10.1681/ASN.2012070713.
Wolf M. Forging forward with 10 burning questions on FGF23 in kidney disease. J Am Soc Nephrol. 2010;21(9):1427–35. doi:10.1681/ASN.2009121293.
Evenepoel P, Naesens M, Claes K, Kuypers D, Vanrenterghem Y. Tertiary ‘hyperphosphatoninism’ accentuates hypophosphatemia and suppresses calcitriol levels in renal transplant recipients. Am J Transplant. 2007;7(5):1193–200. doi:10.1111/j.1600-6143.2007.01753.x.
Kawarazaki H, Shibagaki Y, Fukumoto S, Kido R, Ando K, Nakajima I, et al. Natural history of mineral and bone disorders after living-donor kidney transplantation: a one-year prospective observational study. Ther Apher Dial. 2011;15(5):481–7. doi:10.1111/j.1744-9987.2011.00932.x.
Wolf M, Weir MR, Kopyt N, Mannon RB, Von Visger J, Deng H, et al. A prospective cohort study of mineral metabolism after kidney transplantation. Transplantation. 2016;100(1):184–93. doi:10.1097/TP.0000000000000823.
Sirilak S, Chatsrisak K, Ingsathit A, Kantachuvesiri S, Sumethkul V, Stitchantrakul W, et al. Renal phosphate loss in long-term kidney transplantation. Clin J Am Soc Nephrol. 2012;7(2):323–31. doi:10.2215/CJN.06380611.
Tomida K, Hamano T, Ichimaru N, Fujii N, Matsui I, Nonomura N, et al. Dialysis vintage and parathyroid hormone level, not fibroblast growth factor-23, determines chronic-phase phosphate wasting after renal transplantation. Bone. 2012;51(4):729–36. doi:10.1016/j.bone.2012.06.027.
Praditpornsilpa K, Townamchai N, Chaiwatanarat T, Tiranathanagul K, Katawatin P, Susantitaphong P, et al. The need for robust validation for MDRD-based glomerular filtration rate estimation in various CKD populations. Nephrol Dial Transplant. 2011;26(9):2780–5. doi:10.1093/ndt/gfq815.
Evenepoel P, Meijers B, Viaene L, Bammens B, Claes K, Kuypers D, et al. Fibroblast growth factor-23 in early chronic kidney disease: additional support in favor of a phosphate-centric paradigm for the pathogenesis of secondary hyperparathyroidism. Clin J Am Soc Nephrol. 2010;5(7):1268–76. doi:10.2215/CJN.08241109.
Hirukawa T, Kakuta T, Nakamura M, Fukagawa M. Mineral and bone disorders in kidney transplant recipients: reversible, irreversible, and de novo abnormalities. Clin Exp Nephrol. 2015;19(4):543–55. doi:10.1007/s10157-015-1117-z.
Pihlstrom H, Dahle DO, Mjoen G, Pilz S, Marz W, Abedini S, et al. Increased risk of all-cause mortality and renal graft loss in stable renal transplant recipients with hyperparathyroidism. Transplantation. 2015;99(2):351–9. doi:10.1097/TP.0000000000000583.
Bleskestad IH, Bergrem H, Leivestad T, Hartmann A, Goransson LG. Parathyroid hormone and clinical outcome in kidney transplant patients with optimal transplant function. Clin Transplant. 2014;28(4):479–86. doi:10.1111/ctr.12341.
Hiemstra TF, Brown AJ, Chaudhry AN, Walsh M. Association of calcium, phosphate and parathyroid hormone with renal allograft function: a retrospective cohort study. Am J Nephrol. 2013;37(4):339–45. doi:10.1159/000348376.
Lou I, Foley D, Odorico SK, Leverson G, Schneider DF, Sippel R, et al. How well does renal transplantation cure hyperparathyroidism? Ann Surg. 2015;262(4):653–9. doi:10.1097/SLA.0000000000001431.
Schumock GT, Andress D, E Marx S, Sterz R, Joyce AT, Kalantar-Zadeh K. Impact of secondary hyperparathyroidism on disease progression, healthcare resource utilization and costs in pre-dialysis CKD patients. Curr Med Res Opin. 2008;24(11):3037–48. doi:10.1185/03007990802437943.
Chartsrisak K, Vipattawat K, Assanatham M, Nongnuch A, Ingsathit A, Domrongkitchaiporn S, et al. Mineral metabolism and outcomes in chronic kidney disease stage 2–4 patients. BMC Nephrol. 2013;14:14. doi:10.1186/1471-2369-14-14.
Fukagawa M, Kido R, Komaba H, Onishi Y, Yamaguchi T, Hasegawa T, et al. Abnormal mineral metabolism and mortality in hemodialysis patients with secondary hyperparathyroidism: evidence from marginal structural models used to adjust for time-dependent confounding. Am J Kidney Dis. 2013;. doi:10.1053/j.ajkd.2013.08.011.
Ritskes-Hoitinga J, Lemmens AG, Danse LH, Beynen AC. Phosphorus-induced nephrocalcinosis and kidney function in female rats. J Nutr. 1989;119(10):1423–31.
Gwinner W, Suppa S, Mengel M, Hoy L, Kreipe HH, Haller H, et al. Early calcification of renal allografts detected by protocol biopsies: causes and clinical implications. Am J Transplant. 2005;5(8):1934–41. doi:10.1111/j.1600-6143.2005.00938.x.
Matsuzaki H, Uehara M, Suzuki K, Liu QL, Sato S, Kanke Y, et al. High phosphorus diet rapidly induces nephrocalcinosis and proximal tubular injury in rats. J Nutr Sci Vitaminol (Tokyo). 1997;43(6):627–41.
Beyea A, Block C, Schned A. Acute phosphate nephropathy following oral sodium phosphate solution to cleanse the bowel for colonoscopy. Am J Kidney Dis. 2007;50(1):151–4. doi:10.1053/j.ajkd.2007.03.005.
Chang AR, Miller ER 3rd, Anderson CA, Juraschek SP, Moser M, White K, et al. Phosphorus additives and albuminuria in early stages of CKD: a randomized controlled trial. Am J Kidney Dis. 2016;. doi:10.1053/j.ajkd.2016.08.029.
Voormolen N, Noordzij M, Grootendorst DC, Beetz I, Sijpkens YW, van Manen JG, et al. High plasma phosphate as a risk factor for decline in renal function and mortality in pre-dialysis patients. Nephrol Dial Transplant. 2007;22(10):2909–16. doi:10.1093/ndt/gfm286.
Wolf M, Molnar MZ, Amaral AP, Czira ME, Rudas A, Ujszaszi A, et al. Elevated fibroblast growth factor 23 is a risk factor for kidney transplant loss and mortality. J Am Soc Nephrol. 2011;22(5):956–66. doi:10.1681/ASN.2010080894.
Schaeffner ES, Fodinger M, Kramar R, Sunder-Plassmann G, Winkelmayer WC. Prognostic associations of serum calcium, phosphate and calcium phosphate concentration product with outcomes in kidney transplant recipients. Transpl Int. 2007;20(3):247–55. doi:10.1111/j.1432-2277.2006.00436.x.
Moore J, Tomson CR, Tessa Savage M, Borrows R, Ferro CJ. Serum phosphate and calcium concentrations are associated with reduced patient survival following kidney transplantation. Clin Transplant. 2011;25(3):406–16. doi:10.1111/j.1399-0012.2010.01292.x.
Baia LC, Humalda JK, Vervloet MG, Navis G, Bakker SJ, de Borst MH, et al. Fibroblast growth factor 23 and cardiovascular mortality after kidney transplantation. Clin J Am Soc Nephrol. 2013;8(11):1968–78. doi:10.2215/CJN.01880213.
Acknowledgements
This study was supported by grants from Faculty of Medicine, Ramathibodi Hospital, Mahidol University and National Kidney Foundation of Thailand.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Honoraria: Sinee Disthabanchong (Fresenius Kabi, Sanofi and Kyowa Hakka Kirin).
Ethical statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee at which the studies were conducted (Approval Number MURA2009/1245) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
About this article

Cite this article
Prakobsuk, S., Sirilak, S., Vipattawat, K. et al. Hyperparathyroidism and increased fractional excretion of phosphate predict allograft loss in long-term kidney transplant recipients. Clin Exp Nephrol 21, 926–931 (2017). https://doi.org/10.1007/s10157-016-1370-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10157-016-1370-9