
Abstract
Background
Treatment of IgA nephropathy (IgAN) in Japan has recently changed, from oral prednisolone (oPSL) to tonsillectomy plus steroid pulse (TSP) therapy. However, a few studies have compared their efficacy and safety.
Methods
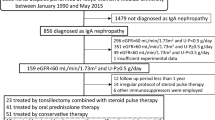
IgAN patients diagnosed in our institution between 1991 and 2013, treated with TSP or oPSL, aged ≥16 years, with ≥1 g/day proteinuria, and estimated glomerular filtration rate (eGFR) ≥30 ml/min/1.73 m2, and no other renal disease were selected. Baseline clinical and histological findings, clinical outcomes, and adverse events were compared. Clinical remission (CR) was defined as <0.3 g/day proteinuria and <5 urinary red blood cells per high-powered field.
Results
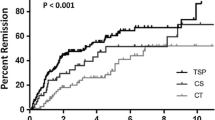
Sixty-six patients were identified; after propensity score adjustment, 26 patients were selected in each group. CR rates were significantly higher at 12 (30.8 % vs. 3.9 %), 36 (47.3 % vs. 7.9 %), and 72 (57.8 % vs. 20.1 %) months (p < 0.01), and the renal survival rate, defined as the development of a 25 % reduction from baseline eGFR, was significantly higher at 12 (96.2 % vs. 69.2 %), 36 (96.2 % vs. 61.5 %), and 72 (96.2 % vs. 41.0 %) months in the TSP than the oPSL group (p < 0.001). Multivariate analysis showed that TSP was the only independent factor associated with CR (hazard ratio, 3.58; 95 % confidence interval, 1.32–10.91, p = 0.01). The number of patients with adverse events was significant lower in TSP group than in oPSL group (11.5 % vs. 34.6 %, p = 0.04).
Conclusions
CR rates are higher; protection of renal function and prevention from adverse events were superior with TSP than with oPSL in patients with IgAN and moderate-to-severe proteinuria.


Similar content being viewed by others

References
Donadio JV, Grande JP. IgA nephropathy. N Engl J Med. 2002;347:738–48.
Kobayashi Y, Fujii K, Hiki Y, Tateno S. Steroid therapy in IgA nephropathy: prospective pilot study in moderate proteinuric cases. QJMed. 1986;61:935–43.
Kobayashi Y, Hiki Y, Kokubo T, Horii A, Tateno S. Steroid therapy during the early stage of progressive IgA nephropathy. A 10-year follow-up study. Nephron. 1996;72:237–42.
Pozzi C, Bolasco PG, Fogazzi GB, Andrulli S, Altieri P, Ponticelli C, Locatelli F. Corticosteroids in IgA nephropathy: a randomized controlled trial. Lancet. 1999;353:883–7.
Pozzi C, Andrulli S, Del Vecchio L, Melis P, Fogazzi GB, Altieri P, Ponticelli C, Locatelli F. Corticosteroid effectiveness in IgA nephropathy: long-term results of a randomized, controlled trial. J Am Soc Nephrol. 2004;15:157–63.
Hotta O, Miyazaki M, Furuta T, Tomioka S, Chiba S, Horigome I, Abe K, Taguma Y. Tonsillectomy and steroid pulse therapy significantly impact on clinical remission in patients with IgA nephropathy. Am J Kidney Dis. 2001;38:736–43.
Miura N, Imai H, Kikuchi S, Hayashi S, Endoh M, Kawamura T, Tomino Y, Moriwaki K, Kiyomoto H, Kohagura K, Nakazawa E, Kusano E, Mochizuki T, Nomura S, Sasaki T, Kashihara N, Soma J, Tomo T, Nakabayashi I, Yoshida M, Watanabe T. Tonsillectomy and steroid pulse (TSP) therapy for patients with IgA nephropathy: a nationwide survey of TSP therapy in Japan and an analysis of the predictive factors for resistance to TSP therapy. Clin Exp Nephrol. 2009;13:460–6.
Matsuzaki K, Suzuki Y, Nakata J, Sakamoto N, Horikoshi S, Kawamura T, Matsuo S, Tomino Y. Nationwide survey on current treatments for IgA nephropathy in Japan. Clin Exp Nephrol. 2013;17:827–33.
Ochi A, Moriyama Y, Takei T, Uchida K, Nitta K. Comparison between steroid pulse therapy alone and in combination with tonsillectomy for IgA nephropathy. Int Urol Nephrol. 2013;45:469–76.
Kamei D, Moriyama T, Takei T, Wakai S, Nitta K. Comparison between consecutive and intermittent steroid pulse therapy combined with tonsillectomy for clinical remission of IgA nephropathy. Clin Exp Nephrol. 2014;18:320–8.
Kawamura T, Joh K, Okonogi H, Koike K, Utsunomiya Y, Miyazaki Y, Matsushima M, Yoshimura M, Horikoshi S, Suzuki Y, Furusu A, Yasuda T, Shirai S, Shibata T, Endoh M, Hattori M, Katafuchi R, Hashiguchi A, Kimura K, Matsuo S, Tomino Y. Study group special IgA nephropathy a histologic classification of IgA nephropathy for predicting long-term prognosis: emphasis on end-stage renal disease. J Nephrol. 2013;26:350–7.
Matsuo S, Imai E, Horio M, et al. Collaborators developing the Japanese equation for estimated GFR.Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis. 2009;53:982–92.
Suzuki Y, Matsuzaki K, Suzuki H, Sakamoto N, Joh K, Kawamura T, Tomino Y, Matsuo S. Proposal of remission criteria for IgA nephropathy. Clin Exp Nephrol. 2014;18:481–6.
Sato M, Hotta O, Tomioka S, Horigome I, Chiba S, Miyazaki M, Noshiro H, Taguma Y. Cohort study of advanced IgA nephropathy: efficacy and limitations of corticosteroids with tonsillectomy. Nephron Clin Pract. 2003;93:c137–45.
Komatsu H, Sato Y, Miyamoto T, Tamura M, Nakata T, Tomo T, Nishino T, Miyazaki M, Fujimoto S. Significance of tonsillectomy combined with steroid pulse therapy for IgA nephropathy with mild proteinuria. Clin Exp Nephrol. 2016;20:94–102.
Takechi H, Oda T, Hotta O, Yamamoto K, Oshima N, Matsunobu T, Shiotani A, Nagura H, Shimazaki H, Tamai S, Sakurai Y, Kumagai H. Clinical and immunological implications of increase in CD208 + dendritic cells in tonsils of patients with immunoglobulin A nephropathy. Nephrol Dial Transpl. 2013;28:3004–13.
Bene MC, Faure G, Hurault de Ligny B, Kessler M, Duheille J. Immunoglobulin A nephropathy. Quantitative immunohistomorphometry of the tonsillar plasma cells evidences an inversion of the immunoglobulin A versus immunoglobulin G secreting cell balance. J Clin Invest. 1983;71:1342–7.
Migita K, Eguchi K, Kawabe Y, Nakamura T, Shirabe S, Tsukada T, Ichinose Y, Nakamura H, Nagataki S. Apoptosis of induction in human peripheral blood T lymphocytes by high-dose steroid therapy. Transplantation. 1997;64:583–7.
Hotta O. Use of corticosteroids, other immunosuppressive therapies, and tonsillectomy in the treatment of IgA nephropathy. Semin Nephrol. 2004;24:244–55.
Chen Y, Tang Z, Wang Q, Yu Y, Zeng C, Chen H, Liu ZH, Li LS. Long-term efficacy of tonsillectomy in Chinese patients with IgA nephropathy. Am J Nephrol. 2007;27:170–5.
Akagi H, Kosaka M, Hattori K, Doi A, Fukushima K, Okano M, Kariya S, Nishizaki K, Sugiyama N, Shikata K, Makino H, Masuda Y. Long-term results of tonsillectomy as a treatment for IgA nephropathy. Acta Otolaryngol. 2004;555:38–42.
Wang Y, Chen J, Wang Y, Chen Y, Wang L, Lv Y. A meta-analysis of the clinical remission rate and long-term efficacy of tonsillectomy in patients with IgA nephropathy. Nephrol Dial Transplant. 2011;26:1923–31.
Moriyama T, Tanaka K, Iwasaki C, Oshima Y, Ochi A, Kataoka H, Itabashi M, Takei T, Uchida K, Nitta K. Prognosis in IgA nephropathy: 30-year analysis of 1,012 patients at a single center in Japan. PLoS One. 2014;9:e91756.
Kawasaki Y, Suyama K, Abe Y, Ushijima Y, Sakai N, Takano K, Ito M, Hashimoto K, Hosoya M. Tonsillectomy with methylprednisolone pulse therapy as rescue treatment for steroid resistant IgA nephropathy in children. Tohoku J Exp Med. 2009;218:11–6.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors report no disclosures or conflicts of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee at which the studies were conducted (IRB approval number #3738) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
“Informed consent for renal biopsy was obtained from all individual participants included in the study.”
About this article

Cite this article
Hoshino, Y., Moriyama, T., Uchida, K. et al. Comparison of oral steroids with tonsillectomy plus steroid pulse therapy in patients with IgA nephropathy. Clin Exp Nephrol 21, 617–623 (2017). https://doi.org/10.1007/s10157-016-1324-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10157-016-1324-2