
Abstract
Background
Achieving a normal final adult height (FH) remains a challenge in the field of pediatric kidney transplantation (KTx). To examine the optimal approach to assuring normal FH following KTx, we retrospectively examined the post-transplant growth and FH of pediatric KTx recipients.
Methods
Since the relevant factors affecting the FH of children following KTx are multifactorial and notably complex, KTx recipients with persistent good graft function and successful steroid minimization until FH attainment were selected for this study.
Results
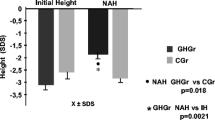
Thirteen patients were enrolled in this study. The mean estimated glomerular filtration rate was 72.1 ± 15.3 ml/min/1.73 m2, and the mean corticosteroid dose was 0.05 ± 0.05 mg/kg on alternate days at the time of FH attainment. Despite highly successful KTx, four (30.8 %) patients (one who underwent KTx before puberty and three during puberty) showed a decrease in the height standard deviation score (hSDS) from the time of KTx until FH attainment. Moreover, of these, two male patients had an FH with an SD <−2.
Conclusion
FH remained suboptimal despite highly successful KTx. Not only highly successful KTx but also further treatment such as steroid avoidance, early steroid withdrawal or using rhGH might be necessary to assure a normal FH in some pubertal patients.


Similar content being viewed by others

References
Harambat J, Cochat P. Growth after renal transplantation. Pediatr Nephrol. 2009;24:1297–306.
Broyer M, Le Bihan C, Charbit M, Guest G, Tête MJ, Gagnadoux MF, Niaudet P. Long-term social outcome of children after kidney transplantation. Transplantation. 2004;77:1033–7.
Fine RN. Management of growth retardation in pediatric recipients of renal allografts. Nat Clin Pract Nephrol. 2007;3:318–24.
Cochat P, Harambat J. Maximizing growth in children after renal transplantation. Transplantation. 2009;88:1321–2.
Hokken-Koelega AC, van Zaal MA, van Bergen W, de Ridder MA, Stijnen T, Wolff ED, de Jong RC, Donckerwolcke RA, de Muinck Keizer-Schrama SM, Drop SL. Final height and its predictive factors after renal transplantation in childhood. Pediatr Res. 1994;36:323–8.
Broyer M, Guest G, Gagnadoux MF. Growth rate in children receiving alternate day corticosteroid treatment after kidney transplantation. J Pediatr. 1992;120:721–5.
Fine RN, Martz K, Stablein D. What have 20 years of data from the North American Pediatric Renal Transplant Cooperative Study taught us about growth following renal transplantation in infants, children, and adolescents with end-stage renal disease? Pediatr Nephrol. 2010;25:739–46.
Nissel R, Brázda I, Feneberg R, Wigger M, Greiner C, Querfeld U, Haffner D. Effect of renal transplantation in childhood on longitudinal growth and adult height. Kidney Int. 2004;66:792–800.
Hattori M, Akioka Y, Chikamoto H, Kobayashi N, Tsuchiya K, Shimizu M, Kagami S, Tsukaguchi H. Increase of integrin-linked kinase activity in cultured podocytes upon stimulation with plasma from patients with recurrent FSGS. Am J Transplant. 2008;8:1550–6.
Suwa S, Tachibana K, Maesaka H, Tanaka T, Yokoya S. Longitudinal standards for height and height velocity for Japanese children from birth to maturity. Clin Pediatr Endocrinol. 1992;1:5–13.
Murata M. Japanese specific bone age standard on the TW 2. Clin Pediatr Endocrinol. 1993;2(Suppl 3):35–41.
Schwartz GJ, Brion LP, Spitzer A. The use of plasma creatinine concentration for estimating glomerular filtration rate in infants, children, and adolescents. Pediatr Clin North Am. 1987;34:571–90.
Fine RN. Etiology and treatment of growth retardation in children with chronic kidney disease and end-stage renal disease: a historical perspective. Pediatr Nephrol. 2010;25:725–32.
Englund MS, Tydén G, Wikstad I, Berg UB. Growth impairment at renal transplantation: a determinant of growth and final height. Pediatr Transplant. 2003;7:192–9.
Schaefer F, Seidel C, Binding A, Gasser T, Largo RH, Prader A, Schärer K. Pubertal growth in chronic renal failure. Pediatr Res. 1990;28:5–10.
Maxwell H, Haffner D, Rees L. Catch-up growth occurs after renal transplantation in children of pubertal age. J Pediatr. 1998;133:435–44.
Klare B, Montoya CR, Fisher DC, Stangl MJ, Haffner D. Normal adult height after steroid-withdrawal within 6 months of pediatric kidney transplantation: a 20 years single center experience. Transplant Int. 2012;25:276–82.
Delucchi Á, Valenzuela M, Lillo AM, Guerrero JL, Cano F, Azocar M, Zambrano P, Salas P, Pinto V, Ferrario M, Rodriguez J, Cavada G. Early steroid withdrawal in pediatric renal transplant: five years of follow-up. Pediatr Nephrol. 2011;26:2235–44.
Grenda R, Watoson A, Trompeter R, Tönshoff B, Jaray J, Fitzpatrick M, Murer L, Vondrak K, Maxwell H, van Damme -Lombaerts R, Loirat C, Mor E, Cochat P, Milford DV, Brown M, Webb NJ. A randomized trial to assess the impact of early steroid withdrawal on growth in pediatric renal transplantation: The TWIST study. Am J Transplant. 2010;10:828–36.
Li L, Chang A, Naesens M, Kambham N, Waskerwitz J, Martin J, Wong C, Alexander S, Grimm P, Concepcion W, Salvatierra O, Sarwal MM. Steroid-free immunosuppression since 1999: 129 pediatric renal transplants with sustained graft and patients benefits. Am J Transplant. 2009;9:1362–72.
Grenda R. Effects of steroid avoidance and novel protocols on growth in paediatric renal transplant patients. Pediatr Nephrol. 2010;25:747–52.
Höcker B, Weber LT, Feneberg R, Drube J, John U, Fehrenbach H, Pohl M, Zimmering M, Fründ S, Klaus G, Wühl E, Tönshoff B. Prospective, randomized trial on late steroid withdrawal in pediatric renal transplant recipients under cyclosporine micro emulsion and mycophenolate mofetil. Transplantation. 2009;87:934–41.
Motoyama O, Hasegawa A, Aikawa A, Shishido S, Honda M, Tsuzuki K, Kinukawa T, Hattori M, Ogawa O, Yanagihara T, Saito K, Takahashi K, Oshima S. Final height in a prospective trial of late steroid withdrawal after pediatric renal transplantation treated with cyclosporine and mizoribine. Pediatr Transplant. 2012;16:78–82.
Tainio J, Qvist E, Vehmas R, Jahnukainen K, Hölttä T, Valta H, Jahnukainen T, Jalanko H. Pubertal development is normal in adolescents after renal transplantation in childhood. Transplantation. 2011;92:404–9.
Hokken-Koelega AC, Stijnen T, de Ridder MA, de Muinck Keizer-Schrama SM, Wolff ED, de Jong MC, Donckerwolcke RA, Groothoff JW, Blum WF, Drop SL. Growth hormone treatment in growth-retarded adolescents after renal transplantation. Lancet. 1994;343:1313–7.
Acknowledgments
The authors gratefully acknowledge Drs. Masataka Hisano, Kiyonobu Ishizuka and Noriko Sugawara, Department of Pediatric Nephrology, Tokyo Women’s Medical University, for providing care for these patients.
Conflict of interest
The authors have declared that no conflict of interest exists.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Fujii, H., Chikamoto, H., Akioka, Y. et al. Final adult height in kidney recipients who underwent highly successful transplantation as children: a single-center experience. Clin Exp Nephrol 18, 515–520 (2014). https://doi.org/10.1007/s10157-013-0842-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10157-013-0842-4