
Abstract
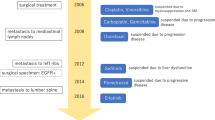
A 52-year-old Japanese female was admitted to our hospital for microhematuria, proteinuria and progressive renal dysfunction. Two years prior to admission, she was diagnosed with lung adenocarcinoma and multiple bone and brain metastases, and was treated with gefitinib (250 mg/day). Treatment for 6 months induced partial response with 30% regression of the primary lung tumor, and resolution of metastatic tumors. After confirmation of the partial remission state, we performed percutaneous renal biopsy. Glomeruli showed mild to moderate mesangial proliferation, segmental endocapillary proliferation and occasional fibrocellular crescent formation. In addition, severe interstitial fibrosis and tubular atrophy relative to the degree of glomerular sclerosis were noted. Immunofluorescence microscopy showed predominant IgA deposition in the mesangial area. Electron microscopy revealed subepithelial and paramesangial electron-dense deposits. In consideration of the prognosis of lung cancer and complication of immunosuppressive treatment, we continued gefitinib only and closely followed-up the clinical course in the outpatient clinic. Sixteen months later, she continued to have proteinuria and microhematuria, and the severity of renal dysfunction was still the same. However, the lung cancer started to increase in size. This is quite an unusual case presenting histologically with tubulointerstitial nephritis and IgA nephropathy in a patient on long-term treatment with gefitinib.




Similar content being viewed by others


References
Ranson M, Hammond LA, Ferry D, Kris M, Tullo A, Murray PI, et al. ZD1839, a selective oral epidermal growth factor receptor-tyrosine kinase inhibitor is well tolerated and active in patients with solid, malignant tumors: results of a phase I trial. J Clin Oncol. 2002;20:2240–50.
Inoue A, Saijo Y, Maemondo M, Gomi K, Tokue Y, Kimura Y, et al. Severe acute interstitial pneumonia and gefitinib. Lancet. 2003;361:137–9.
Truell JS, Fishbein MC, Figlin R. Myocarditis temporally related to the use of gefitinib. Arch Pathol Lab Med. 2005;129:1044–6.
Kumasaka R, Nakamura N, Shirato K, Osawa H, Takanashi S, Hasegawa Y, et al. Side effects of therapy: case 1. Nephrotic syndrome associated with gefitinib therapy. J Clin Oncol. 2004;22:2504–5.
Lau KK, Santos NMD. Post-infectious acute glomerulonephritis with predominant mesangial deposition of IgA. Clin Exp Nephrol. 2005;9:262–3.
Francois H, Placier S, Flamant M, Tharaux PL, Chansel D, Dussaule JC, et al. Prevention of renal vascular and glomerular fibrosis by epidermal growth factor receptor inhibition. FASEB J. 2004;18:926–8.
Suzuki H, Aoshiba K, Yokohori N, Nagai A. Epidermal growth factor receptor tyrosine kinase inhibition augments a murine model of pulmonary fibrosis. Cancer Res. 2003;63:5054–9.
Ando M, Okamoto I, Yamamoto N, Takeda K, Tamura K, Seto T, et al. Predictive factors for interstitial lung disease, antitumor response, and survival in non-small-cell lung cancer patients treated with gefitinib. J Clin Oncol. 2006;24:2549–56.
Miya T, Ono Y, Tanaka H, Koshiishi Y, Goya T. Radiation recall pneumonitis induced by Gefitinib (Iressa): a case report. Nihon Kokyuki Gakkai Zasshi. 2003;41:565–8. (Japanese).
Goodyear PR, Kachra Z, Bell C, Rozen R. Renal tubular cells are potential targets for epidermal growth factor. Am J Physiol. 1988;255:F1191–6.
Gibson S, Tu S, Oyer R, Anderson SM, Johnson GL. Epidermal growth factor protects epithelial cell against Fas-induced apoptosis. Requirement for Akt activation. J Biol Chem. 1999;274:17612–8.
Wassef L, Kelly D, Gilbert RE. Epidermal growth factor receptor inhibition attenuates early kidney enlargement in experimental diabetes. Kidney Int. 2004;66:1805–14.
Torres VE, Sweeney WE Jr, Wang X, Qian Q, Harris PC, Frost P, et al. EGF receptor tyrosine kinase inhibition attenuates the development of PKD in Han:SRPD rats. Kidney Int. 2003;64:1573–9.
Chan LYY, Leung JCK, Lai KN. Novel mechanisms of tubulointerstitial injury in IgA nephropathy: a new therapeutic paradigm in the prevention of progressive renal failure. Clin Exp Nephrol. 2004;8:297–303.
Acknowledgments
We thank Ms. H. Noguchi (Kyushu University Hospital) and M. Munakata (Fukuoka Red Cross Hospital) for the excellent technical assistance. We also thank Dr. F.G. Issa (http://www.word-medex.com.au) for the careful reading and editing of our manuscript.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Masutani, K., Fujisaki, K., Maeda, H. et al. Tubulointerstitial nephritis and IgA nephropathy in a patient with advanced lung cancer treated with long-term gefitinib. Clin Exp Nephrol 12, 398–402 (2008). https://doi.org/10.1007/s10157-008-0066-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10157-008-0066-1