
Abstract
Surgical resections of meningiomas, the most common intracranial tumor in adults, can only be curative if radical resection is achieved. Potentially, the extent of resection could be improved, especially in complex and/or high-grade meningiomas by fluorescence-guided surgery using 5-aminolevulinic acid (5-ALA), indocyanine green (ICG), or fluorescein. This review aims to summarize and evaluate these fluorescence-guided meningioma surgery techniques. PubMed and Embase were searched for relevant articles. Additionally, we checked reference lists for further studies. Forty-eight articles were included in the final analysis. 5-ALA fluoresced with varying sensitivity and selectivity in meningiomas and in invaded bone and dura mater. Although ICG was mainly applied for video angiography, one report shows tumor fluorescence 18–28 h post-ICG injection. Lastly, the use of fluorescein could aid in the identification of tumor remnants; however, detection of dural tail is highly questionable. Fluorescence-guided meningioma surgery should be a reliable, highly specific, and sensitive technique. Despite numerous studies reporting the use of fluorescent dyes, currently, there is no evidence that these tools improve the radical resection rate and long-term recurrence-free outcome in meningioma surgery without neurological deficits. Evidence regarding the effectiveness and increased safety of resection after the application of these fluorophores is currently lacking. Future research should focus on the development of a meningioma-targeted, highly sensitive, and specific fluorophore.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Meningiomas are the most frequently occurring intracranial tumors in adults, accounting for one third of cases [1]. They are classified into three separate World Health Organization (WHO) grades based on histology, mitotic index, and the presence of brain invasion [2]. Although meningiomas are mostly benign and slow growing, they compress surrounding brain tissue and nerves. Depending on location and time course, symptoms such as seizures, focal neurological deficits (e.g., extremity weakness or visual changes), or (severe) mental status changes can arise. Treatment is most effective when complete surgical radical resection is achieved aiming to remove the complete tumor while preserving neurological function. Incomplete resection is a major risk factor for recurrence [2]. Currently, differentiation between meningioma tumor invasion in the dura mater or adjacent bone and reactive tissue is limited. Chances of safe gross total resection without compromising neurological outcome may decrease due to location (such as the cerebellopontine angle), invasion of dura and/or bone, and involvement of neurovascular structures. Fluorescence-guided meningioma surgery may be a helpful tool to increase the extent of resection, especially in patients with complex meningiomas.
Introduced in 1948 by Moore et al, fluorescein was applied to visualize brain tumors [3]. Later, 5-aminolevulinic acid (5-ALA) has been implemented in the field of neurosurgery, mainly in glioblastoma surgery [4]. Indocyanine green (ICG) has been utilized for video angiography mainly for neurovascular neurosurgery (aneurysms, arteriovenous malformation, and fistulas) [5]. More recently, these dyes have been applied in meningioma resections.
This review aims to give a descriptive overview of the most frequently applied intra-operative dyes (5-ALA, ICG, and fluorescein) in meningioma surgery and evaluate their role in terms of efficacy, additional extent of resection, and complication rate.
Material and methods
PubMed and Embase were searched (search strategy in Supplemental Table 1). There were no restrictions regarding publication date; however, only full-text articles in English were assessed. The latest search update was on the 10th of July, 2018. No quality assessment was performed because the quality of the reports appeared insufficient during full-text screening of the articles.
Results
Literature search
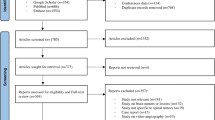
The literature search revealed 427 articles. After duplicate removal, each abstract (n = 314) was screened independently by two authors (BMD and RJMG) and reference lists were evaluated to identify additional relevant articles. In total, 88 full-text articles were assessed for eligibility. Of these, 48 articles were included in the final analysis. We excluded review articles, editorials, letters to editors containing no new experimental data, author replies, and comments (Fig. 1).

Study flow diagram
Below, we will consecutively describe the reported use of 5-ALA, ICG, and fluorescein in meningioma surgery. More specifically, the application of these fluorophores will be reviewed separately in imaging of the tumor, adjacent (invaded) dura mater, and bone. Additionally, other applications of these dyes will be summarized.
5-Aminolevulinic acid
After oral administration, 5-aminolevulinic acid (5-ALA) causes the induction of protoporphyrin IX (PpIX), a natural precursor of hemoglobin, which is normally converted to heme by ferrochelatase. In tumor cells, ferrochelatase activity is lower compared to normal tissue, and thus, PpIX accumulates mostly in tumor cells. It is excited by wavelengths of 400 nm and emits wavelengths at 620–710 nm [6]. In neurosurgery, it has been approved for glioma surgery, where it increased both the extent of resection and survival [6]. In meningioma surgery, 5-ALA has been used off-label to detect intracranial and spinal meningiomas. Its application has been described in the detection of invasion of the dural tail and bone as well (Tables 1 and 2).
Tumor imaging
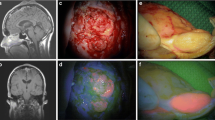
Most publications report cases or case series evaluating fluorescence status (intensity, homogeneity) in intracranial meningioma [7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23]. In a recent review [33] and meta-analysis [34], it appeared difficult to draw conclusions regarding the role of 5-ALA in meningioma surgery due to the experimental nature of 5-ALA-guided meningioma surgery. Most importantly, sensitivity and specificity rates were inconsistent between studies, although remaining high with an overall sensitivity of 92–98% and specificity of 95%. No correlation between fluorescent intensity and WHO grade or histological subtype became apparent and fluorescence was often heterogenic [7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23, 33, 34]. These findings are similar to our own experience. By way of illustration, a 50-year-old male patient underwent 5-ALA-assisted surgery of a recurrent grade I (meningotheliomatous) meningioma. Bright violet homogeneous fluorescence was observed intraoperatively with an inhomogeneous fluorescence pattern (Fig. 2).

Top panel shows gadolinium contrast-enhanced MRI scans of a recurrent grade I meningioma in a 50-year-old male. Bottom panel depicts intraoperative images after preoperative oral administration of 5-ALA. MRI scans revealed a recurrent parietal meningioma (a, b). Intraoperatively, the meningioma became visible using white light (c) and after excitation with blue light, the meningioma showed bright violet, inhomogeneous fluorescence (d)
Although 5-ALA has primarily been applied in intracranial meningiomas, its use in spinal meningiomas has been of interest as well. In two separate case reports, it allowed for the discrimination between tumor tissue and scar tissue [24] or normal tissue and residual tumor [25]. In another case series, fluorescence was homogenous in ten patients (83%) and heterogeneous in two patients (17%) [26].
Dural imaging
Fluorescence status in the dural tail was observed in 103 samples. Only 30 samples (29%) were histologically analyzed. Of these, six patients with histologically confirmed meningioma invasion showed fluorescence in the dural tail (20%) [7, 19]. Unaffected dura mater did not fluoresce in 17 cases (57%) [7,8,9, 12, 20]. Additionally, six affected dural tails (20%) did not fluoresce [20, 23]. Lastly, Brokinkel et al [23] showed PpIX formation of a non-fluorescent-invaded tail, using mass spectrometry.
Bone imaging
Fluorescence status in bone flaps was determined in 129 samples in total [7, 8, 10, 14, 15, 20,21,22, 27, 28] with subsequent histological evaluation in 114 samples (88%). Of these, 69 samples (61%) fluoresced and showed meningioma invasion upon histological examination [7, 10, 14, 20, 22, 28]. Both bright and weak fluorescence have been noted. In one report, fluorescent hyperostotic bone showed involvement in all samples (n = 36) and non-fluorescent non-hyperostotic bone was unaffected in all samples (n = 5) [28]. Invaded bone did not fluoresce in eight samples (7%) [14, 28]. Lastly, in 36 samples (32%), absence of tumor cells in non-fluorescent bone was confirmed [8, 27, 28].
Other applications
A handheld probe (minispectrometer) could detect fluorescence with 100% sensitivity in a spatial resolution of 1 mm2 in one patient harboring a skull base meningioma [11]. In another report, sensitivity of the minispectrometer was 93% (versus only 53% of surgical microscope), probably due to close proximity of the light source to the tumor [31]. Additionally, the authors reported that they could better distinguish invaded dural tail from normal dura mater using the probe [18, 29] and others claimed that they were able to differentiate glioblastomas from meningiomas based on fluorescence intensity [30].
Red light excitation of PpIX increased penetration depth up to 5 mm. Compared to blue light excitation, specificity and sensitivity were lower, and fluorescence was weaker using red light excitation. Additionally, in order to generate overlay images, this technique was not real-time. One meningioma fluoresced using blue light excitation, but did not with red light excitation [32].
Indocyanine green
ICG was first approved for assessing hepatic and cardiac functioning, and later in ophthalmology. The use of ICG in meningioma surgery has only recently been explored, most frequently using ICG video angiography (ICG VA), visualizing the vasculature and not the tumor itself. A summary of included applications and articles has been listed in Tables 1 and 3.
Tumor imaging
One publication reported the “second window technique” where ICG was administered 18–28 h preoperatively. Seventy-eight percent of cases showed tumor fluorescence. Patients injected > 22 h prior to surgery demonstrated an inverse fluorescence pattern, i.e., healthy brain fluoresced stronger than tumor. Sensitivity was high (96%), but specificity was low (39%), possibly due to camera exposure settings [35].
Dural imaging
No reports have established the application of ICG for the identification of meningioma invasion of the dural tail.
Bone imaging
No reports have established the application of ICG for the identification of meningioma bone invasion.
Other applications
Transdural video angiography applies ICG VA to visualize cortical veins, dural venous sinuses, and/or tumor boundaries prior to dural opening in 46 patients [39,40,41,42, 45, 46]. It allowed for a tailored dural opening without damaging underlying vasculature and the possibility of assessing vessel patency and blood flow (direction) [40,41,42, 45]. One group described the “Eclipse sign” [43, 44], which occurs after coagulating feeding arteries, dura mater, and middle meningeal arteries. It can be observed transdurally: the meningioma appears as a shadow after ICG injection due to reduced or absent blood flow, in contrast to dura and adjacent normal brain. This sign was observed in eight patients (40%) [43, 44]. According to the authors, absent (52%) or reduced (8%) “Eclipse sign” was suggestive of intracranial arterial supply to the tumor [43, 44].
Using arterial video angiography, patency of arteries after manipulation for tumor resection was confirmed in three patients [36]. Moreover, collateral arterial circulation was demonstrated, with subsequent sacrifice of arteries improving surgical resection without post-operative ischemia in 17 patients [36,37,38]. In total, 43% of 23 patients in total showed benefit from ICG VA arterial imaging, as judged by the surgeons through additional resection without ischemia.
Venous video angiography has been applied in 97 patients. According to the authors, the rate of resection was occasionally increased by confirming occlusion of veins using ICG VA in thrombosed veins [36, 40, 45, 47], identifying collateral venous drainage with [36, 39, 48] or without [39] subsequent venous sacrifice, and determining the relation of veins with the tumor (draining versus collateral veins) [39, 42, 45].
Fluorescein
Fluorescein was first applied in 1948 for the identification of several types of brain tumor types [3]. Later it was used in ophthalmology for retinal imaging and more recently in neurosurgery, mostly in glioblastoma surgery [49]. It has a peak excitation at 490 nm and emission between 500 and 550 nm. Fluorescein has been tried in meningioma surgery with and without yellow 560 nm filter, and as a contrast agent in confocal microscopy. Reports show fluorescein imaging without appropriate controls or histological confirmation, making the evaluation of this technique extremely difficult. A summary of fluorescein intraoperative imaging is given below and an overview is listed in Tables 1 and 4.
Tumor imaging
The use of fluorescein-guided surgery without a microscope filter has been described in skull base [50,51,52] and convexity meningiomas [53]. Overlap of patients between these studies occurs. Fluorescent signal appeared in the meningioma 10 min after injection using a standard white light microscope, with heightened contrast between meningiomas and cranial nerves. Digitally quantified pre- and post-resection fluorescence showed statistical significant difference [50,51,52]. Using a yellow 560 nm microscope filter in 30 patients, homogeneous fluorescence occurred in 88% of meningiomas and 12% showed heterogeneous tumor fluorescence [54]. Furthermore, the authors reported that the application of fluorescein did not significantly change the surgical plan [54].
Dural imaging
One case series reported the identification of meningioma-positive dural tail in five patients (100%) by fluorescein fluorescence using a standard white light microscope [53]. Adjacent dura mater fluoresced in all cases (n = 25) applying a yellow-560 nm filtered microscope in another study, although this was not histologically confirmed [54].
Bone imaging
Bone involvement has not been described using fluorescein-guided standard white light surgical microscopy. However, it could be identified in five patients (20%) using filtered microscopy: bone fluorescence was observed in three bone flaps and in two skull base meningiomas [54].
Other applications
Confocal microscopy could reveal histopathological details, such as dense sheets, psammoma bodies, microscopic margin between tumor and brain parenchyma, and dural invasion [55, 56]. Furthermore, WHO grade and meningioma subtype could be determined correctly with high sensitivity and specificity [56, 57]. A high number of images were uninterpretable due to blood or motion artifacts and histology was vaguer compared to H&E sections [55,56,57].
Fluorescein video angiography at the end of resection was successfully applied to evaluate vessel patency and feeding and en passage vessels. The authors claim it was useful in vessel preservation and prevention of morbidity; however, no long-term follow-up was available [54].
Discussion
The main risk factor for meningioma recurrence is an incomplete resection. In order to improve extent of resection, the ability to adequately identify tumor to normal tissue borders should be enhanced. This may be possible through the application of intraoperative fluorescence-guided surgery. In this review, we evaluated the literature and summarized the intra-operative use of 5-ALA, ICG, and fluorescein aiming to determine the benefit of fluorescent guidance during meningioma surgery in striving for a radical resection.
Current reports have major limitations. In this review, the majority of included studies are case reports or series with low level of evidence. Only a few report large(r) patient cohorts. To date, most studies are only anecdotal without an adequate study design: they cannot provide strong evidence and merely reflect the surgeon’s observations, e.g., extent of resection or additional safe resection. Only few reports are based on (partially) standardized protocols, for example, noting fluorescence status of tumor, bone, dura mater, and adjacent healthy tissue with at least documentation of neurological deficits and post-operative MRIs determining rate of resection. Indeed, few of the included studies followed a structured sampling approach. Thus, these outcome measures are often biased by the investigator(s) and not readily comparable between patients, even within the same study. Moreover, most studies are retrospective and no randomized controlled trials have been reported. Most reports lack reliable patient data, such as basic patient characteristics, histopathological data, and (long term) follow-up. Consequently, currently, the level of evidence for the use of fluorescence is low due to selection bias.
Reported follow-up time was mostly very limited (“post-operative days,” “post-operatively”) without long-term outcome. Short-term outcomes were mostly positive: transient or no neurological deficit and (in only a few reports) complete resection on post-operative MRI. Long-term confirmation of radical resection without neurological deficits could not be determined, e.g., in terms of progression-free survival or recurrence rates. These outcome variables are essential for the evaluation of fluorescent techniques.
Furthermore, most studies used a dichotomous scoring system to assess quality of fluorescence signal. Although this system is easily reproducible, it is not applicable for all clinical and/or experimental issues [58] and quantification of fluorescence intensity is flawed. A three- or five-level grading score would be more appropriate for the objective recording of fluorescence quality. Due to clinical applicability, the three-level system would be the first choice [58], e.g., non-fluorescent (1), minimal/moderate fluorescent (2), and highly fluorescent (3). Additionally, quantifying fluorescence using an intraoperative spectrometer enables the comparison of fluorescence intensity in a more standardized fashion by measuring absolute fluorescence levels. Although some studies applied in vivo spectrometry with quantitative analysis using an intraoperative probe, the majority only performed a qualitative analysis.
Numerous drawbacks of presently applied dyes became apparent in this review. Currently, no compelling evidence is available regarding the benefit of fluorescence-guided meningioma surgery. It might aid surgical resection in select cases through detection of meningioma remnants or invasion or by aiding in safe vascular sacrifice. Additionally, the investigated fluorophores severely lack sensitivity and specificity to distinguish meningioma (infiltration) from healthy brain tissue. Multiple studies applying 5-ALA show heterogenic meningioma fluorescent patterns [12, 33] and emphasize the role of homogenic fluorescence in complete surgical resection. However, fluorescence homogeneity was not discussed in most reports investigating any of the three investigated fluorophores. Tumor margin determination was unreliable, reducing the value of using these fluorophores. Moreover, histological analysis of individual samples was almost never or only partially reported, which diminishes the ability to correlate fluorescence (intensity) with presence of meningioma cells and severely limits the possibility of calculating sensitivity and specificity rates.
In tumor imaging, 5-ALA has high sensitivity and specificity for meningioma tissue. However, fluorescence heterogeneity and the absence of correlation between fluorescence and mitotic index remain relevant issues. Sensitivity is low(er) in dural and bone invasion compared to the fluorescence results obtained in the tumor itself. Recently, PpIX formation in a non-fluorescent-invaded dural tail was confirmed using mass spectrometry. Although emphasizing the need for a more accurate technique in fluorescence-guided meningioma surgery, this technique is highly inefficient in clinical practice. Only one study described imaging of the meningioma tumor using ICG [54]. The imaging protocol should be improved to increase sensitivity rates and tumor-to-background ratio. Other reports apply video angiography for transdural, arterial, and/or venous imaging, claiming the benefit for half of the patients, determined by surgeons personal (subjective) judgment without standardized techniques. The benefit of transdural ICG VA remains highly questionable, as established techniques such as intraoperative neuronavigation already offer accurate transdural visualization of the meningioma. In total, 75% of all investigated cases benefitted from transdural imaging following ICG VA: in the authors opinions, it increased the feeling of safety during dural opening and assessing vessel patency. Data regarding objective long-term follow-up of these “positive” cases is lacking. Authors claim arterial and venous imaging could address the uncertainty of patency, anastomotic flow, and the distinction between tumor draining veins and collateral ones. Its benefit has been described in the minority of patients, without objectifying criteria to determine superiority of this application above surgery without this tool. Fluorescein fluorescence has been performed with filter (filtered surgical microscopy) and without (standard white light microscopy). Despite the convenience and affordability of white light fluorescein surgical microscopy, contrast between tumor and surrounding tissue is markedly less evident compared to filtered surgical microscopy. Additionally, one group [54] reported that the intraoperative fluorescein-induced meningioma fluorescence did not significantly alter the surgical strategy, emphasizing the questionability of this fluorophore in meningioma surgery.
Differentiation between meningioma invasion and reactive tissue is limited at present. Pre-operatively, changes of dura mater and bone can be observed as a “dural tail sign” or bone hypertrophy. The dural tail sign is often observed on MRI scans as dural thickening adjacent to the meningioma, and is either caused by meningioma invasion or by vascular congestion, both accounting for approximately 50% of cases [59]. 5-ALA fluorescence was observed in invaded and normal dura mater, reducing sensitivity (50%). Reports describing ICG fluorescence did not determine fluorescence status of adjacent dura mater or histologically investigated dural invasion [35]. Lastly, the dura mater always fluoresces after fluorescein administration, thus making the ability to differentiate between healthy dura mater and meningioma infiltration highly questionable. This emphasizes the need for highly sensitive and specific fluorescent dyes in meningioma surgery.
Similarly, distinction between (reactive) hyperostosis and tumor invasion cannot always be readily made. Bone invasion has been reported in 20–68% meningioma patients, primarily in the presence of hyperostosis. Regardless, invasion has been described in non-hyperostotic bone as well, in 10–40% of cases [60, 61]. Indeed, all fluorescent (n = 21) and none of the non-fluorescent (n = 18) bone presented meningioma invasion in one study [28] applying 5-ALA. The only other dye showing bone fluorescence was fluorescein; however, histological results were not provided [54]. ICG bone fluorescence was not observed. In addition to location, local invasion of bone and soft tissues makes it a technical challenge to determine the tumor margin using available surgical tools. Fluorescence-guided meningioma surgery may be a helpful tool to increase the rate of resection, especially in patients with complex meningiomas.
In summary, we reviewed the current experience of 5-ALA, ICG, and fluorescein in meningioma surgery. In our opinion, fluorescence-guided meningioma surgery should be a reliable, highly specific, and sensitive technique. Despite numerous studies reporting the use of fluorescent dyes, currently there is no evidence that these tools improve the radical resection rate and long-term recurrence-free outcome in meningioma surgery and no evidence exists that safety of surgery increased due to application of these fluorescence techniques.
Future perspectives
Failure of currently available fluorescence techniques clearly show the need for a highly meningioma-specific probe clearly distinguishing the tumor margin from healthy tissue has become apparent after analyzing current data in this review. We propose the development and intraoperative use of targeted tracers, which could be achieved by binding a meningioma-specific peptide to a fluorescent dye, preferably near-infrared due to increased penetration depth. First, this should be confirmed in in vitro cultures and subsequently in in vivo studies with mice and human subjects. As meningiomas are usually of dural origin, passage of the tracer through the blood-brain-barrier should not be an issue. The use of molecular fluorescent-guided surgery (MFGS) has been successful for various tumor types, e.g., in ovarian carcinoma [62] and peritoneal metastases of colorectal carcinomas [63] targeting αvβ3-integrin or folate receptor α and vascular endothelial growth factor α, respectively. The use of MFGS seems feasible for the optimization of meningioma surgery, which is currently a high priority in our ongoing research.
Next to this, improving and validating existing fluorescence-guided techniques could be an alternative. Current evidence is mostly based on case reports and case series and therefore an organized trial could be another next step. The organization of such a trial could improve the quality of evidence tremendously and is a necessary step in the further development of this MFGS technique. Outcome measures to be considered are among others extent of resection, fluorescence status and homogeneity, and correlation between fluorescence and WHO grade, along with long-term follow-up.
References
Ostrom QT, Gittleman H, Fulop J, Liu M, Blanda R, Kromer C, Wolinsky Y, Kruchko C, Barnholtz-Sloan JS (2015) CBTRUS statistical report: primary brain and central nervous system tumors diagnosed in the United States in 2008-2012. Neuro-Oncology 17:iv1–iv62. https://doi.org/10.1093/neuonc/nov189
Campbell BA, Jhamb A, Maguire JA, Toyota B, Ma R (2009) Meningiomas in 2009. Controversies and future challenges. Am J Clin Oncol Cancer Clin Trials 32:73–85. https://doi.org/10.1097/COC.0b013e31816fc920
Moore GE, Peyton WT, French LA, Walker WW (1948) The clinical use of fluorescein in neurosurgery. J Neurosurg 5:392–398. https://doi.org/10.3171/jns.1948.5.4.0392
Li Y, Rey-Dios R, Roberts DW, Valdés PA, Cohen-Gadol AA (2014) Intraoperative fluorescence-guided resection of high-grade gliomas: a comparison of the present techniques and evolution of future strategies. World Neurosurg 82:175–185. https://doi.org/10.1016/j.wneu.2013.06.014
Reinhart MB, Huntington CR, Blair LJ, Heniford BT, Augenstein VA (2016) Indocyanine green :historical context, current applications, and future considerations. Surg Innov 23:166–175. https://doi.org/10.1177/1553350615604053
Stummer W, Pichlmeier U, Meinel T, Wiestler OD, Zanella F, Reulen HJ (2006) Fluorescence-guided surgery with 5-aminolevulinic acid for resection of malignant glioma: a randomised controlled multicentre phase III trial. Lancet Oncol 7:392–401. https://doi.org/10.1016/S1470-2045(06)70665-9
Kajimoto Y, Kuroiwa T, Miyatake S-I, Ichioka T, Miyashita M, Tanaka H, Tsuji M (2007) Use of 5-aminolevulinic acid in fluorescence-guided resection of meningioma with high risk of recurrence. J Neurosurg 106:1070–1074. https://doi.org/10.3171/jns.2007.106.6.1070
Morofuji Y, Matsuo T, Hayashi Y, Suyama K, Nagata I (2008) Usefulness of intraoperative photodynamic diagnosis using 5-aminolevulinic acid for meningiomas with cranial invasion: technical case report. Neurosurgery 62:102–103. https://doi.org/10.1227/01.neu.0000317378.22820.46
Eljamel S (2009) Which intracranial lesions would be suitable for 5-aminolevulenic acid-induced fluorescence-guided identification, localization, or resection? A prospective study of 114 consecutive intracranial lesions. Clin Neurosurg 56:93–97. https://doi.org/10.1080/02688690903032491
Coluccia D, Fandino J, Fujioka M, Cordovi S, Muroi C, Landolt H (2010) Intraoperative 5-aminolevulinic-acid-induced fluorescence in meningiomas. Acta Neurochir 152:1711–1719. https://doi.org/10.1007/s00701-010-0708-4
Bekelis K, Valdés PA, Erkmen K, Leblond F, Kim A, Wilson BC, Harris BT, Paulsen KD, Roberts DW (2011) Quantitative and qualitative 5-aminolevulinic acid–induced protoporphyrin IX fluorescence in skull base meningiomas. Neurosurg Focus 30:E8. https://doi.org/10.3171/2011.2.FOCUS1112
Whitson WJ, Valdes PA, Harris BT, Paulsen KD, Roberts DW (2011) Confocal microscopy for the histological fluorescence pattern of a recurrent atypical meningioma: case report. Neurosurgery 68:E1768–E1772. https://doi.org/10.1227/NEU.0b013e318217163c
Chae MP, Song SW, Park SH, Park CK (2012) Experience with 5-aminolevulinic acid in fluorescence-guided resection of a deep sylvian meningioma. J Korean Neurosurg Soc 52:558–560. https://doi.org/10.3340/jkns.2012.52.6.558
Della Puppa A, Scienza R (2013) Letter to the editor: 5-aminolevulinic acid–guided resection of bone-invasive meningiomas. Neurosurg Focus 35:E6. https://doi.org/10.3171/2012.6.FOCUS12236
Moriuchi S, Yamada K, Dehara M, Teramoto Y, Soda T, Imakita M, Taneda M (2013) Use of 5-aminolevulinic acid to detect residual meningioma and ensure total removal while avoiding neurological deficits. J Neurol Neurophysiol 4:iii217–iii225. https://doi.org/10.1093/neuonc/not191
Cornelius JF, Slotty PJ, Kamp MA, Schneiderhan TM, Steiger HJ, El-Khatib M (2014) Impact of 5-aminolevulinic acid fluorescence-guided surgery on the extent of resection of meningiomas - with special regard to high-grade tumors. Photodiagn Photodyn Ther 11:481–490. https://doi.org/10.1016/j.pdpdt.2014.07.008
Marbacher S, Klinger E, Schwyzer L, Fischer I, Nevzati E, Diepers M, Roelcke U, Fathi A-R, Coluccia D, Fandino J (2014) Use of fluorescence to guide resection or biopsy of primary brain tumors and brain metastases. Neurosurg Focus 36:E10. https://doi.org/10.3171/2013.12.FOCUS13464
Valdes PA, Bekelis K, Harris BT, Wilson BC, Leblond F, Kim A, Simmons NE, Erkmen K, Paulsen KD, Roberts DW (2014) 5-Aminolevulinic acid-induced protoporphyrin IX fluorescence in meningioma: qualitative and quantitative measurements in vivo. Neurosurgery 10:74–82. https://doi.org/10.1227/NEU.0000000000000117
Wilbers E, Hargus G, Wölfer J, Stummer W (2014) Usefulness of 5-ALA (Gliolan®)-derived PPX fluorescence for demonstrating the extent of infiltration in atypical meningiomas. Acta Neurochir 156:1853–1854. https://doi.org/10.1007/s00701-014-2148-z
Millesi M, Kiesel B, Mischkulnig M, Martínez-Moreno M, Wöhrer A, Wolfsberger S, Knosp E, Widhalm G (2016) Analysis of the surgical benefits of 5-ALA–induced fluorescence in intracranial meningiomas: experience in 204 meningiomas. J Neurosurg 125:1408–1419. https://doi.org/10.3171/2015.12.JNS151513
Potapov AA, Goryaynov SA, Okhlopkov VA, Shishkina LV, Loschenov VB, Savelieva TA, Golbin DA, Chumakova AP, Goldberg MF, Varyukhina MD, Spallone A (2016) Laser biospectroscopy and 5-ALA fluorescence navigation as a helpful tool in the meningioma resection. Neurosurg Rev 39:437–447. https://doi.org/10.1007/s10143-015-0697-0
Scheichel F, Ungersboeck K, Kitzwoegerer M, Marhold F (2017) Fluorescence-guided resection of extracranial soft tissue tumour infiltration in atypical meningioma. Acta Neurochir 159:1027–1031. https://doi.org/10.1007/s00701-017-3166-4
Brokinkel B, Kröger S, Senner V, Jeibmann A, Karst U, Stummer W (2018) Visualizing protoporphyrin IX formation in the dura tail of meningiomas by mass spectrometry imaging. Acta Neurochir 160:1–5. https://doi.org/10.1007/s00701-018-3488-x
Eicker SO, Floeth FW, Kamp MA, Steiger HJ, Hänggi D (2013) The impact of fluorescence guidance on spinal intradural tumour surgery. Eur Spine J 22:1394–1401. https://doi.org/10.1007/s00586-013-2657-0
Muroi C, Fandino J, Coluccia D, Berkmann S, Fathi A-R, Landolt H (2013) 5-Aminolevulinic acid fluorescence-guided surgery for spinal meningioma. World Neurosurg 80:223e1–222e3. https://doi.org/10.1016/j.wneu.2012.12.017
Millesi M, Kiesel B, Woehrer A, Hainfellner JA, Novak K, Martínez-Moreno M, Wolfsberger S, Knosp E, Widhalm G (2014) Analysis of 5-aminolevulinic acid–induced fluorescence in 55 different spinal tumors. Neurosurg Focus 36:E11. https://doi.org/10.3171/2013.12.FOCUS13485
Cornelius JF, Slotty PJ, Stoffels G, Galldiks N, Langen KJ, Steiger HJ (2013) 5-aminolevulinic acid and 18F-FET-PET as metabolic imaging tools for surgery of a recurrent skull base meningioma. J Neurol Surgery, Part B Skull Base 74:211–216. https://doi.org/10.1055/s-0033-1342918
Della Puppa A, Rustemi O, Gioffrè G, Troncon I, Lombardi G, Rolma G, Sergi M, Munari M, Cecchin D, Gardiman MP, Scienza R (2014) Predictive value of intraoperative 5-aminolevulinic acid–induced fluorescence for detecting bone invasion in meningioma surgery. J Neurosurg 120:840–845. https://doi.org/10.3171/2013.12.JNS131642
Valdés PA, Leblond F, Kim A, Harris BT, Wilson BC, Fan X, Tosteson TD, Hartov A, Ji S, Erkmen K, Simmons NE, Paulsen KD, Roberts DW (2011) Quantitative fluorescence in intracranial tumor: implications for ALA-induced PpIX as an intraoperative biomarker. J Neurosurg 115:115:11–115:17. https://doi.org/10.3171/2011.2.JNS101451
Cornelius JF, Placke JM, Knipps J, Fischer I, Kamp MA, Steiger HJ (2017) Minispectrometer with handheld probe for 5-ALA based fluorescence-guided surgery of brain tumors: preliminary study for clinical applications. Photodiagn Photodyn Ther 17:147–153. https://doi.org/10.1016/j.pdpdt.2016.12.007
Knipps J, Beseoglu K, Kamp MA, Fischer I, Felsberg J, Neumann LM, Steiger HJ, Cornelius JF (2017) Fluorescence behavior and dural infiltration of meningioma analyzed by 5-aminolevulinic acid–based fluorescence: operating microscope versus mini-spectrometer. World Neurosurg 108:118–127. https://doi.org/10.1016/j.wneu.2017.08.140
Roberts DW, Olson JD, Evans LT, Kolste KK, Kanick SC, Fan X, Bravo JJ, Wilson BC, Leblond F, Marois M, Paulsen KD (2017) Red-light excitation of protoporphyrin IX fluorescence for subsurface tumor detection. J Neurosurg 128:1–8. https://doi.org/10.3171/2017.1.JNS162061
Motekallemi A, Jeltema JR, Metzemaekers JDM, van Dam GM, Crane LMA, Groen RJM (2015) The current status of 5-ALA fluorescence-guided resection of intracranial meningiomas—a critical review. Neurosurg Rev 38:619–628. https://doi.org/10.1007/s10143-015-0615-5
Foster N, Eljamel S (2016) ALA-induced fluorescence image guided surgery of meningiomas: a meta-analyses. Photodiagn Photodyn Ther 15:73–78. https://doi.org/10.1016/j.pdpdt.2016.05.006
Lee JYK, Pierce JT, Thawani JP, Zeh R, Nie S, Martinez-Lage M, Singhal S (2017) Near-infrared fluorescent image-guided surgery for intracranial meningioma. J Neurosurg 128:1–11. https://doi.org/10.3171/2016.10.JNS161636
Ferroli P, Acerbi F, Albanese E, Tringali G, Broggi M, Franzini A, Broggi G (2011) Application of intraoperative indocyanine green angiography for CNS tumors: results on the first 100 cases. In: Acta neurochirurgica. Supplement, Austria, pp 251–257
Kim DL, Cohen-Gadol AA (2013) Indocyanine-green videoangiogram to assess collateral circulation before arterial sacrifice for management of complex vascular and neoplastic lesions: technical note. World Neurosurg 79:404.e1–404.e6. https://doi.org/10.1016/j.wneu.2012.07.028
Rustemi O, Scienza R, Della Puppa A (2016) Intra-operative devascularization of petroclival meningiomas by ICG-VA-guided Bernasconi & Cassinari artery identification. Acta Neurochir 158:427–428. https://doi.org/10.1007/s00701-016-2704-9
Acerbi F, Vetrano IG, Sattin T, de Laurentis C, Bosio L, Rossini Z, Broggi M, Schiariti M, Ferroli P (2018) The role of indocyanine green videoangiography with FLOW 800 analysis for the surgical management of central nervous system tumors: an update. Neurosurg Focus 44:E6. doi: https://doi.org/10.3171/2018.3.FOCUS1862
Kim EH, Cho JM, Chang JH, Kim SH, Lee KS (2011) Application of intraoperative indocyanine green videoangiography to brain tumor surgery. Acta Neurochir 153:1487–1494. https://doi.org/10.1007/s00701-011-1046-x
Nussbaum ES, Defillo A, Nussbaum L (2012) The use of indocyanine green videoangiography to optimize the dural opening for intracranial parasagittal lesions. Oper Neurosurg 70:ons61–ons64. https://doi.org/10.1227/NEU.0b013e31822ecfeb
D’Avella E, Volpin F, Manara R, Scienza R, Della Puppa A (2013) Indocyanine green videoangiography (ICGV)-guided surgery of parasagittal meningiomas occluding the superior sagittal sinus (SSS). Acta Neurochir 155:415–420. https://doi.org/10.1007/s00701-012-1617-5
Ueba T, Abe H, Higashi T, Inoue T (2013) Transdural imaging of meningiomas by indocyanine green videography: the eclipse sign. J Neurol Surgery, Part A Cent Eur Neurosurg 74:51–53. https://doi.org/10.1055/s-0032-1325634
Ueba T, Okawa M, Abe H, Nonaka M, Iwaasa M, Higashi T, Inoue T, Takano K (2013) Identification of venous sinus, tumor location, and pial supply during meningioma surgery by transdural indocyanine green videography. J Neurosurg 118:632–636. https://doi.org/10.3171/2012.11.JNS121113
Della Puppa A, Rustemi O, Gioffrè G, Rolma G, Grandis M, Munari M, Scienza R (2014) Application of indocyanine green video angiography in parasagittal meningioma surgery. Neurosurg Focus 36:E13. https://doi.org/10.3171/2013.12.FOCUS13385
Hide T, Yano S, Shinojima N, Kuratsu J (2015) Usefulness of the indocyanine green fluorescence endoscope in endonasal transsphenoidal surgery. J Neurosurg 122:1185–1192. https://doi.org/10.3171/2014.9.JNS14599
Khurana VG, Seow K, Duke D (2010) Intuitiveness, quality and utility of intraoperative fluorescence videoangiography: Australian Neurosurgical Experience. Br J Neurosurg 24:163–172. https://doi.org/10.3109/02688690903518247
Ferroli P, Nakaji P, Acerbi F, Albanese E, Broggi G (2011) Indocyanine green (ICG) temporary clipping test to assess collateral circulation before venous sacrifice. World Neurosurg 75:122–125. https://doi.org/10.1016/j.wneu.2010.09.011
Shinoda J, Yano H, Yoshimura S-I, Okumura A, Kaku Y, Iwama T, Sakai N (2003) Fluorescence-guided resection of glioblastoma multiforme by using high-dose fluorescein sodium. J Neurosurg 99:597–603. https://doi.org/10.3171/jns.2003.99.3.0597
Da Silva CE, Da Silva JLB, Da Silva VD (2010) Use of sodium fluorescein in skull base tumors. Surg Neurol Int 1:70. https://doi.org/10.4103/2152-7806.72247
Da Silva CE, Da Silva VD, Da Silva JLB (2014) Sodium fluorescein in skull base meningiomas: a technical note. Clin Neurol Neurosurg 120:32–35. https://doi.org/10.1016/j.clineuro.2014.02.015
Da Silva CE, Da Silva VD, Da Silva JLB (2014) Skull base meningiomas and cranial nerves contrast using sodium fluorescein: a new application of an old tool. J Neurol Surgery, Part B Skull Base 75:255–260. https://doi.org/10.1055/s-0034-1372466
Da Silva CE, Da Silva VD, Da Silva JLB (2014) Convexity meningiomas enhanced by sodium fluorescein. Surg Neurol Int 5:3. https://doi.org/10.4103/2152-7806.124978
Akçakaya MO, Göker B, Kasımcan MÖ, Hamamcıoğlu MK, Kırış T (2017) Use of sodium fluorescein in meningioma surgery performed under the YELLOW-560 nm surgical microscope filter: feasibility and preliminary results. World Neurosurg 107:966–973. https://doi.org/10.1016/j.wneu.2017.07.103
Sanai N, Eschbacher JM, Hattendorf G, Coons SW, Preul MC, Smith KA, Nakaji P, Spetzler RF (2011) Intraoperative confocal microscopy for brain tumors: a feasibility analysis in humans. Neurosurgery 68:282–289. https://doi.org/10.1227/NEU.0b013e318212464e
Eschbacher JM, Martirosyan NL, Nakaji P, Sanai N, Preul MC, Smith KA, Coons SW, Spetzler RF (2012) In vivo intraoperative confocal microscopy for real-time histopathological imaging of brain tumors. J Neurosurg 116:854–860. https://doi.org/10.3171/2011.12.JNS11696
Martirosyan NL, Eschbacher JM, Kalani MYS, Turner JD, Belykh E, Spetzler RF, Nakaji P, Preul MC (2016) Prospective evaluation of the utility of intraoperative confocal laser endomicroscopy in patients with brain neoplasms using fluorescein sodium: experience with 74 cases. Neurosurg Focus 40:E11. https://doi.org/10.3171/2016.1.FOCUS15559
Kamp MA, Krause Molle Z, Munoz-Bendix C, Rapp M, Sabel M, Steiger HJ, Cornelius JF (2018) Various shades of red—a systematic analysis of qualitative estimation of ALA-derived fluorescence in neurosurgery. Neurosurg Rev 41:3–18. https://doi.org/10.1007/s10143-016-0745-4
Sotoudeh H (2010) A review on dural tail sign. World J Radiol 2:188–192. https://doi.org/10.4329/wjr.v2.i5.188
Agrawal D, Goyal N, Kakkar A, Sarkar C (2012) Does bony hyperostosis in intracranial meningioma signify tumor invasion? A radio-pathologic study. Neurol India 60:50. https://doi.org/10.4103/0028-3886.93589
Pieper DR, Al-Mefty O, Hanada Y, Buechner D (1999) Hyperostosis associated with meningioma of the cranial base: secondary changes or tumor invasion. Neurosurgery 44:742–747
Van Dam GM, Themelis G, Crane LMA, Harlaar NJ, Pleijhuis RG, Kelder W, Sarantopoulos A, De Jong JS, Arts HJG, Van Der Zee AGJ, Bart J, Low PS, Ntziachristos V (2011) Intraoperative tumor-specific fluorescence imaging in ovarian cancer by folate receptor-α targeting: first in-human results. Nat Med 17:1315–1319. https://doi.org/10.1038/nm.2472
Harlaar NJ, Kelder W, Sarantopoulos A, Bart J, Themelis G, van Dam GM, Ntziachristos V (2013) Real-time near infrared fluorescence (NIRF) intra-operative imaging in ovarian cancer using an αvβ3-integrin targeted agent. Gynecol Oncol 128:590–595. https://doi.org/10.1016/j.ygyno.2012.12.011
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
For this type of study, formal consent is not required.
Animal experiments
This article does not contain any studies with human participants or animals performed by any of the authors.
Electronic supplementary material
ESM 1
(DOCX 13 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Dijkstra, B.M., Jeltema, HR., Kruijff, S. et al. The application of fluorescence techniques in meningioma surgery—a review. Neurosurg Rev 42, 799–809 (2019). https://doi.org/10.1007/s10143-018-01062-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10143-018-01062-4