
Abstract
Spinal dural arteriovenous fistulas (SDAVFs) are rare pathologies with a yearly incidence of 5–10 new cases/million, constituting 60–80 % of spinal arteriovenous malformations. Clinical symptoms include progressive paraparesis, paresthesias, bladder, and bowel disturbances. The pathophysiology of SDAVFs is not well elucidated. Microneurosurgery and endovascular techniques are established treatment modalities for permanent fistula occlusion, which are oftentimes accompanied by an amelioration of neurological deficits in the long run. Here, we report our interdisciplinary neurosurgical/neuroradiological management strategy of SDAVFs in 32 patients who were evaluated retrospectively. We focused on clinical presentation, microneurosurgical and interventional technique, early, and late neurological results. Quality of life (QoL) was additionally assessed in 12 patients at last follow-up. We discuss the results against the background of the current literature. Our series and the literature indicate that clinical outcome after treatment of SDAVF is favorable in general. Both neurosurgical and neurointerventional therapies appear to be safe and effective, but short-term neurological deterioration after the intervention constitutes an as-of-yet unsolved problem. Beyond age and preoperative neurological state, presence of comorbidities had a significant influence on neurological outcome in our study sample. Self-assessed physical and mental QoL at long-term follow-up was reduced in quite a number of patients and was associated with a poorer neurological result as well as presence of comorbidities. The patients’ perspective in terms of QoL was first investigated in this study, but further research on QoL and psychosocial impairment of SDAVF patients is needed to enable individualized counseling and rehabilitation strategies.





Similar content being viewed by others

References
Afshar JK, Doppman JL, Oldfield EH (1995) Surgical interruption of intradural draining vein as curative treatment of spinal dural arteriovenous fistulas. J Neurosurg 82(2):196–200
Aminoff MJ, Logue V (1974) Clinical features of spinal vascular malformations. Brain J Neurol 97(1):197–210
Aminoff MJ, Logue V (1974) The prognosis of patients with spinal vascular malformations. Brain J Neurol 97(1):211–218
Aminoff MJ, Barnard RO, Logue V (1974) The pathophysiology of spinal vascular malformations. J Neurol Sci 23(2):255–263
Andres RH, Barth A, Guzman R, Remonda L, El-Koussy M, Seiler RW, Widmer HR, Schroth G (2008) Endovascular and surgical treatment of spinal dural arteriovenous fistulas. Neuroradiology 50(10):869–876
Asakuno K, Kim P, Kawamoto T, Ogino M (2002) Dural arteriovenous fistula and progressive conus medullaris syndrome as complications of lumbar discectomy. Case report. J Neurosurg 97(3 Suppl):375–379
Bullinger M (1996) Assessment of health related quality of life with the SF-36 health survey. Die Rehabil 35(3):XVII–XXVII, quiz XXVII–XXIX
Bullinger M, Morfeld M, Kohlmann T, Nantke J, van den Bussche H, Dodt B, Dunkelberg S, Kirchberger I, Kruger-Bodecker A, Lachmann A, Lang K, Mathis C, Mittag O, Peters A, Raspe HH, Schulz H (2003) SF-36 health survey in rehabilitation research. Findings from the North German network for rehabilitation research, NVRF, within the rehabilitation research funding program. Die Rehabil 42(4):218–225
Cenzato M, Debernardi A, Stefini R, D’Aliberti G, Piparo M, Talamonti G, Coppini M, Versari P (2012) Spinal dural arteriovenous fistulas: outcome and prognostic factors. Neurosurg Focus 32(5), E11
Dhandapani S, Gupta A, Singh J, Sharma BS, Mahapatra AK, Mehta VS (2013) Spinal dural arterio-venous fistula: clinico-radiological profile and outcome following surgical occlusion in an Indian neurosurgical center. Neurol India 61(4):406–410
Eide PK, Sorteberg AG, Meling TR, Sorteberg W (2013) Directional intraoperative Doppler ultrasonography during surgery on cranial dural arteriovenous fistulas. Neurosurgery 73(2 Suppl Operative):ons211–ons222, discussion ons222-213
Fugate JE, Lanzino G, Rabinstein AA (2012) Clinical presentation and prognostic factors of spinal dural arteriovenous fistulas: an overview. Neurosurg Focus 32(5), E17
Gemmete JJ, Chaudhary N, Elias AE, Toma AK, Pandey AS, Parker RA, Davagnanam I, Maher CO, Brew S, Robertson F (2013) Spinal dural arteriovenous fistulas: clinical experience with endovascular treatment as a primary therapy at 2 academic referral centers. AJNR Am J Neuroradiol 34(10):1974–1979
Gokhale S, Khan SA, McDonagh DL, Britz G (2014) Comparison of surgical and endovascular approach in management of spinal dural arteriovenous fistulas: a single center experience of 27 patients. Surg Neurol Int 5:7
Hacein-Bey L, Konstas AA, Pile-Spellman J (2014) Natural history, current concepts, classification, factors impacting endovascular therapy, and pathophysiology of cerebral and spinal dural arteriovenous fistulas. Clin Neurol Neurosurg 121:64–75
Hanel RA, Nakaji P, Spetzler RF (2010) Use of microscope-integrated near-infrared indocyanine green videoangiography in the surgical treatment of spinal dural arteriovenous fistulae. Neurosurgery 66(5):978–984, discussion 984–975
Hassler W, Thron A (1994) Flow velocity and pressure measurements in spinal dural arteriovenous fistulas. Neurosurg Rev 17(1):29–36
Hassler W, Thron A, Grote EH (1989) Hemodynamics of spinal dural arteriovenous fistulas. An intraoperative study. J Neurosurg 70(3):360–370
Inagawa S, Yamashita S, Hiramatsu H, Kamiya M, Tanaka T, Sakahara H, Aoyama H (2013) Clinical results after the multidisciplinary treatment of spinal arteriovenous fistulas. Jpn J Radiol 31(7):455–464
Jellema K, Tijssen CC, Sluzewski M, van Asbeck FW, Koudstaal PJ, van Gijn J (2006) Spinal dural arteriovenous fistulas—an underdiagnosed disease. A review of patients admitted to the spinal unit of a rehabilitation center. J Neurol 253(2):159–162
Kang JW, Koo JH, Kim DK, Joo YJ, Kim TH, Song SH (2011) Myelopathy caused by spinal dural arterio-venous fistula after first lumbar vertebral body fracture—a case report. Ann Rehabil Med 35(5):729–732
Kataoka H, Miyamoto S, Nagata I, Ueno Y, Hashimoto N (1999) Intraoperative microdoppler monitoring for spinal dural arteriovenous fistulae. Surg Neurol 52(5):466–472
Kirsch M, Berg-Dammer E, Musahl C, Bazner H, Kuhne D, Henkes H (2013) Endovascular management of spinal dural arteriovenous fistulas in 78 patients. Neuroradiology 55(3):337–343
Krings T, Geibprasert S (2009) Spinal dural arteriovenous fistulas. AJNR Am J Neuroradiol 30(4):639–648
Lawton MT, Jacobowitz R, Spetzler RF (1997) Redefined role of angiogenesis in the pathogenesis of dural arteriovenous malformations. J Neurosurg 87(2):267–274
Meisel K, Yee A, Stout C, Kim W, Cooke D, Halbach V (2013) Arteriovenous fistula after ventriculostomy in aneurysmal subarachnoid hemorrhage. Neurology 80(23):2168
Merland JJ, Assouline E, Rufenacht D. (1985/1986) Dural spinal arteriovenous fistulae draining into medullary veins: clinical and radiological results of treatment (embolization and surgery) in 56 cases. Neuroradiology :283–289
Miyachi E, Izumi T, Matsubara N, Naito T, Haraguchi K, Wakabayashi T (2011) Mechanism of the formation of dural arteriovenous fistula: the role of the emissary vein. Interv Neuroradiol J Perither Neurorad Surg Proced Relat Neurosci 17(2):195–202
Narvid J, Hetts SW, Larsen D, Neuhaus J, Singh TP, McSwain H, Lawton MT, Dowd CF, Higashida RT, Halbach VV (2008) Spinal dural arteriovenous fistulae: clinical features and long-term results. Neurosurgery 62(1):159–166, discussion 166–157
Nishimura Y, Natsume A, Ginsberg HJ (2014) Spinal dural arteriovenous fistula associated with L-4 isthmic spondylolisthesis. J Neurosurg Spine 20:670–674
Nishiyama Y, Kanemaru K, Yoshioka H, Hanihara M, Horikoshi T, Kniouchi H (2013) Intracranial pial arteriovenous fistula caused by dural tenting: case report. Neurologia Medico-Chirurgica
Ofran Y, Yovchev I, Hiller N, Cohen J, Rubin SA, Schwartz I, Meiner Z (2013) Correlation between time to diagnosis and rehabilitation outcomes in patients with spinal dural arteriovenous fistula. J Spinal Cord Med 36(3):200–206
Oldfield EH, Di Chiro G, Quindlen EA, Rieth KG, Doppman JL (1983) Successful treatment of a group of spinal cord arteriovenous malformations by interruption of dural fistula. J Neurosurg 59(6):1019–1030
Ropper AE, Gross BA, Du R (2012) Surgical treatment of type I spinal dural arteriovenous fistulas. Neurosurg Focus 32(5), E3
Ruiz-Juretschke F, Perez-Calvo JM, Castro E, Garcia-Leal R, Mateo-Sierra O, Fortea F, Iza B, Garbizu JM, Villoria F (2011) A single-center, long-term study of spinal dural arteriovenous fistulas with multidisciplinary treatment. J Clin Neurosci Off J Neurosurg Soc Australas 18(12):1662–1666
Saladino A, Atkinson JL, Rabinstein AA, Piepgras DG, Marsh WR, Krauss WE, Kaufmann TJ, Lanzino G (2010) Surgical treatment of spinal dural arteriovenous fistulae: a consecutive series of 154 patients. Neurosurgery 67(5):1350–1357, discussion 1357–1358
Santiago R, Guenther E, Carroll K, Junkins EP Jr (2006) The clinical presentation of pediatric thoracolumbar fractures. J Trauma 60(1):187–192
Sasaki O, Yajima N, Ichikawa A, Yamashita S, Nakamura K (2012) Deterioration after surgical treatment of spinal dural arteriovenous fistula associated with spinal perimedullary fistula. Neurol Med Chir 52(7):516–520
Sherif C, Gruber A, Bavinzski G, Standhardt H, Widhalm G, Gibson D, Richling B, Knosp E (2008) Long-term outcome of a multidisciplinary concept of spinal dural arteriovenous fistulae treatment. Neuroradiology 50(1):67–74
Symon L, Kuyama H, Kendall B (1984) Dural arteriovenous malformations of the spine. Clinical features and surgical results in 55 cases. J Neurosurg 60(2):238–247
Tacconi L, Lopez Izquierdo BC, Symon L (1997) Outcome and prognostic factors in the surgical treatment of spinal dural arteriovenous fistulas. A long-term study. Br J Neurosurg 11(4):298–305
Terada T, Higashida RT, Halbach VV, Dowd CF, Tsuura M, Komai N, Wilson CB, Hieshima GB (1994) Development of acquired arteriovenous fistulas in rats due to venous hypertension. J Neurosurg 80(5):884–889
Thron A (2001) Spinal dural arteriovenous fistulas. Radiologe 41(11):955–960
Ushikoshi S, Hida K, Kikuchi Y, Miyasaka K, Iwasaki T, Abe H (1999) Functional prognosis after treatment of spinal dural arteriovenous fistulas. Neurol Med Chir 39(3):206–212, discussion 212–203
Wachter D, Hans F, Psychogios MN, Knauth M, Rohde V (2011) Microsurgery can cure most intracranial dural arteriovenous fistulae of the sinus and non-sinus type. Neurosurg Rev 34(3):337–345, discussion 345
Wakao N, Imagama S, Ito Z, Ando K, Hirano K, Tauchi R, Muramoto A, Matsui H, Matsumoto T, Matsuyama Y, Ishiguro N (2012) Clinical outcome of treatments for spinal dural arteriovenous fistulas: results of multivariate analysis and review of the literature. Spine 37(6):482–488
Westphal M, Koch C (1999) Management of spinal dural arteriovenous fistulae using an interdisciplinary neuroradiological/neurosurgical approach: experience with 47 cases. Neurosurgery 45(3):451–457, discussion 457–458
Yoshino O, Matsui H, Hirano N, Tsuji H (1998) Acquired dural arteriovenous malformations of the lumbar spine: case report. Neurosurgery 42(6):1387–1389
Disclosure
The authors have no personal financial or institutional interest in any of the drugs, materials, or devices described in this article.
Author information
Authors and Affiliations
Corresponding author
Additional information
Comments
Torstein R. Meling, Oslo, Norway
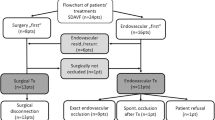
In this issue of NSR, Özkan et al. present their interdisciplinary neurosurgical/neuroradiological management strategy of spinal dural arteriovenous fistulas (SDAVFs) in 32 patients. The article is a retrospective clinical report. Although somewhat difficult to decipher as the table with patient characteristics is incomplete, from the text it seems that the treatments were endovascular in 5/32 (two of whom were later operated due to residual SDAVFs), microsurgical in 25/32 and another 2/32 patients of whom we only learn about due to their retreatments (endovascular and microsurgical, respectively). Follow-up was 100 % at 3 months. Outcome parameters were obliteration rates, modified Aminoff-Logue (AL) myelopathy scale and quality of life (QoL). The obliteration rates after primary therapy is not stated, but a complete fistula obliteration was eventually achieved and documented by angiography in all patients. The AL-score at the 3-month follow-up did not improve significantly (p = 0.13). Three patients (9 %) deteriorated neurologically after surgery, caused by an epidural hematoma in one and persistent intramedullary edema in two patients. With respect to clinical outcome at 3 months, 30/32 patients improved and only two (6.3 %) patients worsened neurologically after surgery. Of the 32 patients treated, only 12 patients filled in the SF-36 QoL questionnaires, making firm conclusions impossible, although the authors use a German standard population as a reference. Not surprisingly, there is a negative correlation between the AL-scores and QoL as measured by the SF-36 questionnaire, but the statistics are not shown, only the p values. The authors conclude that clinical outcome after treatment of SDAVF is good and that microneurosurgery was the treatment of choice in most cases since it provides direct access to the fistula point. It could preferably have been backed up by their own data showing that retreatment was far more frequent after endovascular than microsurgical treatment in their hands.
Rights and permissions
About this article

Cite this article
Özkan, N., Kreitschmann-Andermahr, I., Goerike, S.L. et al. Single center experience with treatment of spinal dural arteriovenous fistulas. Neurosurg Rev 38, 683–692 (2015). https://doi.org/10.1007/s10143-015-0645-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10143-015-0645-z