
Abstract
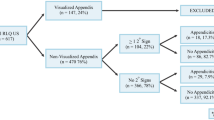
This study aims to retrospectively evaluate the right lower quadrant ultrasounds in women presenting during the second or third trimester of pregnancy for the frequency of appendix visualization and accuracy in diagnosing appendicitis. Institutional Review Board approval was obtained for this Health Insurance Portability and Accountability Act-compliant study. We reviewed imaging records from 99 consecutive pregnant women from 2001 to 2011 who presented during the second (≥14 weeks gestation) or third trimester for right lower quadrant ultrasound to evaluate the appendix. Visualization of the appendix as well as the size and compressibility, if identified, were recorded. The medical records and labs related to the initial patient presentation, subsequent management, and follow-up were reviewed for surgical and clinical outcomes. Pathology records were reviewed to determine if appendicitis was present when appendectomy was performed. Patients who underwent appendectomy were considered to have appendicitis based on pathology results, and patients managed non-operatively with symptom improvement and those with a normal appendix at pathology were considered to not have appendicitis. During the study period, 99 women meeting inclusion criteria presented to our institution for right lower quadrant ultrasound to evaluate the appendix during the second or third trimester of pregnancy. The mean gestational age at presentation was 23 weeks (±7 weeks). The mean maternal age was 28 years (±6.6 years). The appendix was not visualized in 97% (96/99) of right lower quadrant ultrasound examinations. Of the three studies in which the appendix was visualized, two were considered positive for appendicitis and one was considered negative. Eight patients in this group ultimately underwent appendectomy, including the two patients with positive right lower quadrant ultrasounds, and appendicitis confirmed at pathology in seven of these cases (87.5%). Right lower quadrant ultrasound successfully demonstrated an abnormal appendix in 28.7% (two of seven) of surgically confirmed cases; however, this technique did not detect appendicitis in 71% (five of seven) of patients with surgically proven disease due to nonvisualization of the appendix. Retrospective review of right lower quadrant ultrasounds performed during the second and third trimester of pregnancy suggests that this modality has limited utility for diagnosing appendicitis due to infrequent visualization of the appendix.



Similar content being viewed by others


References
Kort B, Katz VL, Watson WJ (1993) The effect of nonobstetric operation during pregnancy. Surg Gynecol Obstet 177:371–376
Kammerer WS (1979) Nonobstetric surgery during pregnancy. Med Clin North Am 63:1157–1164
Kammerer WS (1987) Nonobstetric surgery in pregnancy. Med Clin North Am 71:551–560
Andersen B, Nielsen TF (1999) Appendicitis in pregnancy: diagnosis, management and complications. Acta Obstet Gynecol Scand 78:758–762
Mourad J, Elliott JP, Erickson L, Lisboa L (2000) Appendicitis in pregnancy: new information that contradicts long-held clinical beliefs. Am J Obstet Gynecol 182:1027–1029
Stone K (2002) Acute abdominal emergencies associated with pregnancy. Clin Obstet Gynecol 45:553–561
Bailey LE, Finley RK, Miller SF, Jones LM (1986) Acute appendicitis during pregnancy. Am Surg 52:218–221
Yilmaz HG, Akgun Y, Bac B, Celik Y (2007) Acute appendicitis in pregnancy—risk factors associated with principal outcomes: a case control study. Int J Surg 5:192–197
Berry J, Malt RA (1984) Appendicitis near its centenary. Ann Surg 200:567–575
Andersson RE, Hugander A, Thulin AJ (1992) Diagnostic accuracy and perforation rate in appendicitis: association with age and sex of the patient and with appendicectomy rate. Eur J Surg 158:37–41
Körner H, Söndenaa K, Söreide JA et al (1997) Incidence of acute nonperforated and perforated appendicitis: age-specific and sex-specific analysis. World J Surg 21:313–317
Hale DA, Molloy M, Pearl RH, Schutt DC, Jaques DP (1997) Appendectomy: a contemporary appraisal. Ann Surg 225:252–261
Temple CL, Huchcroft SA, Temple WJ (1995) The natural history of appendicitis in adults. A prospective study. Ann Surg 221:278–281
Balthazar EJ, Rofsky NM, Zucker R (1998) Appendicitis: the impact of computed tomography imaging on negative appendectomy and perforation rates. Am J Gastroenterol 93:768–771
Bendeck SE, Nino-Murcia M, Berry GJ, Jeffrey RB (2002) Imaging for suspected appendicitis: negative appendectomy and perforation rates. Radiology 225:131–136
McGee TM (1989) Acute appendicitis in pregnancy. Aust N Z J Obstet Gynaecol 29:378–385
McGory ML, Zingmond DS, Tillou A, Hiatt JR, Ko CY, Cryer HM (2007) Negative appendectomy in pregnant women is associated with a substantial risk of fetal loss. J Am Coll Surg 205:534–540
Ueberrueck T, Koch A, Meyer L, Hinkel M, Gastinger I (2004) Ninety-four appendectomies for suspected acute appendicitis during pregnancy. World J Surg 28:508–511
Mazze RI, Källén B (1991) Appendectomy during pregnancy: a Swedish registry study of 778 cases. Obstet Gynecol 77:835–840
Coursey CA, Nelson RC, Patel MB et al (2010) Making the diagnosis of acute appendicitis: do more preoperative CT scans mean fewer negative appendectomies? A 10-year study. Radiology 254:460–468
Basaran A, Basaran M (2009) Diagnosis of acute appendicitis during pregnancy: a systematic review. Obstet Gynecol Surv 64:481–488, quiz 499
Chen MM, Coakley FV, Kaimal A, Laros RK (2008) Guidelines for computed tomography and magnetic resonance imaging use during pregnancy and lactation. Obstet Gynecol 112:333–340
Rosen MP, Ding A, Blake MA et al (2011) ACR Appropriateness Criteria(®) right lower quadrant pain-suspected appendicitis. J Am Coll Radiol 8:749–755
Puylaert JB (1986) Acute appendicitis: US evaluation using graded compression. Radiology 158:355–360
Puylaert JB, Rutgers PH, Lalisang RI et al (1987) A prospective study of ultrasonography in the diagnosis of appendicitis. N Engl J Med 317:666–669
Balthazar EJ, Birnbaum BA, Yee J, Megibow AJ, Roshkow J, Gray C (1994) Acute appendicitis: CT and US correlation in 100 patients. Radiology 190:31–35
Lim HK, Bae SH, Seo GS (1992) Diagnosis of acute appendicitis in pregnant women: value of sonography. AJR Am J Roentgenol 159:539–542
Israel GM, Malguria N, McCarthy S, Copel J, Weinreb J (2008) MRI vs. ultrasound for suspected appendicitis during pregnancy. J Magn Reson Imaging 28:428–433
Oto A, Srinivasan PN, Ernst RD et al (2006) Revisiting MRI for appendix location during pregnancy. AJR Am J Roentgenol 186:883–887
Baer JL, Reis RA, Arens RA (1932) Appendicitis in pregnancy with changes in position and axis of the normal appendix in pregnancy. JAMA 98:1359–1364
Barloon TJ, Brown BP, Abu-Yousef MM, Warnock N, Berbaum KS (1995) Sonography of acute appendicitis in pregnancy. Abdom Imaging 20:149–151
Pedrosa I, Levine D, Eyvazzadeh AD, Siewert B, Ngo L, Rofsky NM (2006) MR imaging evaluation of acute appendicitis in pregnancy. Radiology 238:891–899
Cobben LP, Groot I, Haans L, Blickman JG, Puylaert J (2004) MRI for clinically suspected appendicitis during pregnancy. AJR Am J Roentgenol 183:671–675
Phillips B, Ball C, Sackett D, et al (2009) Levels of evidence. Centre for Evidence-based Medicine, Oxford
Andersson RE, Lambe M (2001) Incidence of appendicitis during pregnancy. Int J Epidemiol 30:1281–1285
Andersson RE (2007) The natural history and traditional management of appendicitis revisited: spontaneous resolution and predominance of prehospital perforations imply that a correct diagnosis is more important than an early diagnosis. World J Surg 31:86–92
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lehnert, B.E., Gross, J.A., Linnau, K.F. et al. Utility of ultrasound for evaluating the appendix during the second and third trimester of pregnancy. Emerg Radiol 19, 293–299 (2012). https://doi.org/10.1007/s10140-012-1029-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10140-012-1029-0