
Abstract
Surveillance cultures may detect colonisation with drug-resistant Gram-negative bacteria and can be hypothesised to guide appropriate initial antibiotic treatment for intensive care unit (ICU) patients. We investigated the microbiological data of 228 episodes of nosocomial bloodstream infection (BSI) due to Gram-negative bacteria in an ICU in which piperacillin/tazobactam or meropenem was used empirically for serious infections, to evaluate the contribution of surveillance cultures to an appropriate choice of initial antibiotic therapy. Surveillance cultures were taken in advance of BSI in 218 (95.6%) of 228 episodes. Concordant organisms with identical identification and susceptibilities were found in prior surveillance cultures and subsequent blood cultures in 65 (29.8%) of 218 episodes. Surveillance cultures predicted resistance in 52.9% and 51.4% of BSIs caused by resistant pathogens to piperacillin/tazobactam and meropenem, respectively. The negative predictive value of surveillance cultures negative for a resistant organism also exceeded 90% for piperacillin/tazobactam and meropenem. Given that the overall resistant rates of BSI pathogens of our study were 11.3% to piperacillin/tazobactam and 16.4% to meropenem, surveillance cultures in our setting may provide important information on the probability of drug resistance of the causative pathogens and some utility in aiding empiric antibiotic therapy for ICU patients who subsequently develop BSI.
Similar content being viewed by others


Introduction
The prevalence of multidrug-resistant organisms, for example, methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant enterococci (VRE), multidrug-resistant (MDR) Pseudomonas aeruginosa, carbapenem-resistant Acinetobacter baumannii (CR-AB) and extended-spectrum β-lactamase (ESBL)-producing Enterobacteriaceae, has been rising in intensive care units (ICUs) in recent years. Multidrug resistance makes antibiotic choice for serious infections more difficult. In critically ill patients at risk of infection with drug-resistant pathogens, physicians have a tendency to resort to broad-spectrum antimicrobials or combination therapy with more than two drugs, which are, themselves, linked with additional emergence of multidrug resistance. Therefore, it is difficult for physicians to choose the initial treatment without adequate information on the likely pathogens and their susceptibility profile.
Surveillance cultures are cultures collected despite an absence of clinical features pointing to an infection at the site from which the cultures were collected. Surveillance cultures for Gram-positive cocci of epidemiologic importance (for example, MRSA or VRE) are widely used for infection control purposes. Surveillance cultures may also detect colonisation with drug-resistant Gram-negative bacteria in advance of cultures collected for clinical indications and can be hypothesised to guide appropriate initial antibiotic treatment. However, routinely processing large numbers of such specimens can be expensive and time-consuming for clinical microbiology laboratories. Furthermore, the data on the value of surveillance cultures in guiding empiric antibiotic choice is mixed. In some previous studies, surveillance cultures were reported as a useful predictor of drug-resistant bacteria infections, especially in ventilator-associated pneumonia and bacteraemia [1–7]. However, the contribution of surveillance cultures is still controversial because other studies showed that surveillance cultures failed as a guide for appropriate initial antibiotics due to their low sensitivity [8–10]. The choice of initial antibiotics is quite critical in the management for sepsis in the ICU—in critically ill patients, inadequate initial empiric antibiotic treatment directly affects mortality, underscoring the importance of determining measures which can enhance empiric therapy [11, 12].
In the ICU of the Royal Brisbane and Women’s Hospital, all patients are under routine surveillance by culturing twice weekly endotracheal aspirates and rectal swabs. We investigated the microbiological data of patients with nosocomial bloodstream infection (BSI) in the ICU to evaluate the contribution of surveillance cultures to an appropriate choice of initial antibiotic treatment for this infection.
Materials and methods
Setting
This study was performed in the ICU of the 986-bed Royal Brisbane and Women’s Hospital.
The ICU has 19 beds and has a bed occupancy of 550–670 patient-days per month. It is within a hospital which is a major referral centre for trauma, burns and haematologic transplantation. In the ICU, endotracheal aspirates and rectal swabs are collected twice per week as surveillance cultures. In the absence of colonisation with resistant bacteria, ticarcillin/clavulanic acid was routinely prescribed as the empiric antibiotic therapy for serious infections presumed to be due to Gram-negative bacteria until 2006, when piperacillin/tazobactam became the first-line empiric therapy. Meropenem was used as empiric therapy in patients who had previously received piperacillin/tazobactam or who were known to be colonised with an organism resistant to piperacillin/tazobactam.
Study design
We reviewed nosocomial BSIs with Gram-negative bacilli in the ICU from January 2003 to December 2008. For each nosocomial BSI, we investigated the patient’s prior microbiological data, including both clinical and surveillance cultures during that ICU admission.
The study was approved by the low-risk Human Research Ethics Committee of the Royal Brisbane and Women’s Hospital.
Definitions
Nosocomial BSI was defined as BSI occurring 48 h or more after hospital admission. BSI containing two different species of bacteria was considered, for the purpose of statistical analysis, as two episodes. The antimicrobial susceptibilities of the bacterium implicated in nosocomial BSI were compared with those from bacteria isolated from the most recent surveillance culture (defined as those taken on two or more days before the onset of BSI). MDR was defined as presence of CR-AB, ESBL-producing Enterobacteriaceae or P. aeruginosa resistant to more than two of the following five antibiotics; piperacillin/tazobactam, cefepime, meropenem, ciprofloxacin and amikacin.
Microbiologic methods
Endotracheal aspirates and rectal swabs were taken twice per week as surveillance cultures. Surveillance endotracheal aspirates were cultured on blood and MacConkey agar, in a similar manner to clinical cultures. Rectal swabs were plated onto MacConkey agar containing 8 mg/L of gentamicin in order to screen for antibiotic-resistant Gram-negative bacilli. Bacteria growing on this media were then examined for the presence of ESBL production (in Klebsiella or Escherichia coli) or carbapenem resistance (in A. baumannii). Blood cultures were processed using the BacT/Alert System (bioMérieux, Marcy l’Etoile, France). The identification and susceptibility testing of isolates were performed using the VITEK 2 system (bioMérieux, Marcy l’Etoile, France).
Results
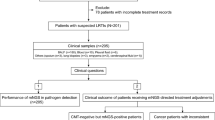
During the study period, 306 episodes of nosocomial BSI developed in 218 patients. Two hundred and twenty-eight episodes were due to Gram-negative bacteria (GNBs), of which P. aeruginosa (75 episodes), K. pneumoniae (38), Enterobacter spp. (26), E. coli (20) and Acinetobacter spp. (19) were the most common (Table 1).
Surveillance cultures and prediction of resistance
Surveillance cultures were taken in advance of Gram-negative BSI in 218 of 228 (95.6%) episodes (Table 1). In 65 (29.8%) of these surveillance cultures, an organism with identical identification and susceptibility pattern to the BSI pathogen was found (Table 1). Surveillance respiratory cultures contributed to the detection of matched isolates with the BSI pathogen in 60 episodes—surveillance rectal swabs detected the Gram-negative pathogen in one patient with ESBL-producing Enterobacteriaceae and five patients with Acinetobacter, including one case with simultaneous detection by surveillance respiratory culture.
Seventy-nine episodes with BSI due to GNBs were resistant to ticarcillin/clavulanic acid (35.4% of all GNBs tested) (Table 2). This included 28 with P. aeruginosa, 14 with E. cloacae, ten with A. baumannii, eight with Serratia marcescens, five with E. coli, two with K. pneumoniae and 12 with other GNBs. Surveillance cultures grew the same species with the predicted resistance in 35 (44.3%) cases of BSI. Other Gram-negative organisms (not found in the blood cultures) with resistance to ticarcillin/clavulanate were found in 10 (12.7%) surveillance cultures. No surveillance culture with a ticarcillin/clavulanate-resistant organism occurred in 34 patients. Thus, resistance to ticarcillin/clavulanate was predicted by surveillance cultures in 57.0% (45/79) of cases (Table 2).
Seventeen patients developed BSI due to GNBs resistant to piperacillin/tazobactam (11.3% of all GNBs tested) (Table 2); these included nine with P. aeruginosa, three with E. cloacae, three with A. baumannii, one with K. pneumoniae and two with other Gram-negative bacilli. Surveillance cultures grew the same species with the predicted resistance in 8 (47.1%) cases. Other Gram-negative organisms with resistance to piperacillin/tazobactam were found in 1 (5.9%) surveillance culture. Thus, resistance to piperacillin/tazobactam was predicted in 52.9% (9/17) of cases (Table 2).
Thirty-seven patients developed BSI due to GNBs resistant to meropenem (16.4% of all GNBs tested) (Table 2); these included 16 with P. aeruginosa, 11 with A. baumannii, five with Stenotrophomonas maltophilia and five with other GNBs. Surveillance cultures grew the same species with the predicted resistance in 16 (43.2%) cases. Other Gram-negative organisms with resistance to meropenem were found in 3 (8.1%) surveillance cultures. Thus, resistance to meropenem was predicted in 51.4% (19/37) of cases (Table 2).
Surveillance cultures: infection control implications
None of the patients with nosocomial Gram-negative BSIs were known to be colonised with an MDR Gram-negative organism prior to their ICU stay. During the course of their ICU stay, CR-AB, MDR P. aeruginosa and ESBL producers were detected by all means (surveillance and clinical cultures) in 18, 15 and four patients, respectively (Table 3). Of these, two MDR P. aeruginosa and one ESBL-producing E. coli were detected only by surveillance cultures. Surveillance cultures also detected CR-AB, MDR P. aeruginosa and ESBL producers prior to their detection in clinical specimens in 10, three and one patients, respectively.
Discussion
The collection of cultures for surveillance purposes is potentially time-consuming and costly for both nursing staff and laboratory staff. The purpose of this evaluation was to determine if the monetary and time costs are outweighed by potential clinical benefits in patients with BSI. Foreseeable benefits could include “an early warning sign” of antibiotic resistance, thus, allowing appropriate empiric antibiotic choice. We evaluated this potential by examining a cohort of patients with Gram-negative BSI acquired in the ICU.
Although surveillance cultures in our study detected concordant organisms in only 29.8% of nosocomial Gram-negative BSIs in the ICU, it is important to note the context of our study. Of all Gram-negative BSI isolates, 11.3% were resistant to piperacillin/tazobactam, 16.4% were resistant to meropenem and 35.4% were resistant to ticarcillin/clavulanate (Table 2). The interpretation of our results needs to be with this context in mind. In cases of BSI resistant to any of these antibiotics, 51–57% (depending on the drug) had a prior surveillance culture also showing resistance. Therefore, this increased the probability of a resistant organism being present in blood cultures, compared to the overall percentage susceptibility of Gram-negative organisms to each antibiotic. Perhaps more importantly, the negative predictive value of surveillance cultures negative for a resistant organism exceeded 90% for piperacillin/tazobactam and meropenem.
Most prior papers have investigated the contribution of surveillance cultures to the treatment of patients with ventilator-associated pneumonia. However, a small number of published papers have mentioned the role of surveillance cultures as a guide for empiric antibiotic treatment for BSIs, which was the approach that we have undertaken (Table 4). Papadomichelakis et al. found that twice weekly surveillance respiratory cultures in ICU detected concordant organisms in 66% of BSIs caused by resistant GNBs, and the percentage rose up to 86% by combination with data from rectal swab samples taken once weekly [6]. In their study, the detection rate of concordant pathogen in surveillance cultures was much higher than that of our study. However, there were several differences in the aetiology of BSIs in this Greek study compared to our own. Resistant organisms were cultured very frequently in their ICU. Eighty-two percent of GNBs which caused BSIs in the Greek study were resistant to one or more of ceftazidime, ciprofloxacin, piperacillin/tazobactam or imipenem, while only 40% of GNBs in our study were resistant to one or more of ticarcillin/clavulanate, piperacillin/tazobactam, meropenem, cefepime, ciprofloxacin or amikacin. Besides, they investigated only 47 BSIs caused by GNBs, and more than 90% of the BSI pathogens in their study were concentrated among only three species, Acinetobacter spp., Pseudomonas spp. and Klebsiella spp. These differences might explain the discrepancy between the high rate of concordance seen in their study and our results because the value of any test generally depends on the characteristics of the subjects.
Blot et al. also reported that the use of surveillance cultures was associated with higher rates of appropriate therapy for patients with bacteraemia caused by resistant GNBs [1]. The authors found that preceding colonisation was detected by surveillance cultures in 74.5% of 157 BSI episodes caused by antibiotic-resistant GNBs. It is noteworthy that they performed surveillance cultures quite aggressively—thrice weekly oral swabs, urine sampling, tracheal aspirates for patients receiving mechanical ventilation and once weekly rectal swabs. They also found that appropriate empiric antibiotic therapy was administered for 74.4% of BSIs in which prior colonisation had been detected compared to 55.0% of episodes that occurred without detection of prior colonisation. However, appropriate initial antibiotic therapy was not improved compared to those with delayed therapy. Since aggressive testing is costly, it should be considered carefully in terms of the potential cost-effectiveness balance. We can find no literature which provides conclusive evidence that the use of surveillance cultures improves clinical outcome from BSI in seriously ill patients. For logistical reasons, we were unable to perform such an outcome analysis ourselves.
We found that surveillance cultures have a role (albeit somewhat imperfect) in guiding empiric antibiotic therapy for patients subsequently found to have BSI. These cultures may have other roles—notably, surveillance cultures may have a potential role in infection control, especially in the ICU [13–18]. Nasal swab samples, which can be collected more easily than respiratory samples, are usually used in active surveillance for MRSA and rectal swabs are used for VRE and resistant enteric pathogens. They may detect more patients who have colonisation with resistant pathogens, indicating the need for contact isolation measures. In our study, 37 MDR Gram-negative organisms were found to be colonised or infected in the patients with a nosocomial BSI at some time during their ICU admission. Surveillance cultures detected 17/37 (45.9%) colonisations or infections prior to the detection in clinical specimens, including three cases which were detected only by surveillance cultures. Previously published data have demonstrated that many factors, including the prevalence of MDR organisms and the compliance of isolation precautions, might influence the efficacy and validity of active surveillance cultures for infection control reasons [13, 14, 17, 18]. Although surveillance cultures may detect some additional patients with MDR organisms, it has not yet been proven that this reduces the spread of MDR Gram-negative organisms in the ICU environment.
In our setting, the contribution of surveillance cultures in guiding initial antibiotic regimens for ICU patients who subsequently develop BSI may be important in patients given piperacillin/tazobactam or meropenem empirically. In particular, a negative surveillance culture for a piperacillin/tazobactam- or meropenem-resistant pathogen has a high negative predictive value for a nosocomial BSI with an organism resistant to these antibiotics. Given the contrasting utility of surveillance cultures in different scenarios and for different purposes, a multicentre randomised trial may be the only way to end the debate as to their utility in defining the optimal empiric antibiotic therapy. As we move into the future, the rapid detection of antibiotic-resistant bacteria directly from blood specimens may be a more appropriate way of prompting early appropriate empiric antibiotic therapy. However, for now, surveillance cultures in our setting do provide some utility in aiding empiric antibiotic therapy and infection control programmes.
References
Blot S, Depuydt P, Vogelaers D, Decruyenaere J, De Waele J, Hoste E, Peleman R, Claeys G, Verschraegen G, Colardyn F, Vandewoude K (2005) Colonization status and appropriate antibiotic therapy for nosocomial bacteremia caused by antibiotic-resistant gram-negative bacteria in an intensive care unit. Infect Control Hosp Epidemiol 26:575–579. doi:10.1086/502575
Boots RJ, Phillips GE, George N, Faoagali JL (2008) Surveillance culture utility and safety using low-volume blind bronchoalveolar lavage in the diagnosis of ventilator-associated pneumonia. Respirology 13:87–96
Depuydt P, Benoit D, Vogelaers D, Claeys G, Verschraegen G, Vandewoude K, Decruyenaere J, Blot S (2006) Outcome in bacteremia associated with nosocomial pneumonia and the impact of pathogen prediction by tracheal surveillance cultures. Intensive Care Med 32:1773–1781
Depuydt PO, Blot SI, Benoit DD, Claeys GW, Verschraegen GL, Vandewoude KH, Vogelaers DP, Decruyenaere JM, Colardyn FA (2006) Antimicrobial resistance in nosocomial bloodstream infection associated with pneumonia and the value of systematic surveillance cultures in an adult intensive care unit. Crit Care Med 34:653–659
Michel F, Franceschini B, Berger P, Arnal J-M, Gainnier M, Sainty J-M, Papazian L (2005) Early antibiotic treatment for BAL-confirmed ventilator-associated pneumonia: a role for routine endotracheal aspirate cultures. Chest 127:589–597. doi:10.1378/chest.127.2.589
Papadomichelakis E, Kontopidou F, Antoniadou A, Poulakou G, Koratzanis E, Kopterides P, Mavrou I, Armaganidis A, Giamarellou H (2008) Screening for resistant gram-negative microorganisms to guide empiric therapy of subsequent infection. Intensive Care Med 34:2169–2175
Reddy P, Malczynski M, Obias A, Reiner S, Jin N, Huang J, Noskin GA, Zembower T (2007) Screening for extended-spectrum beta-lactamase-producing Enterobacteriaceae among high-risk patients and rates of subsequent bacteremia. Clin Infect Dis 45:846–852. doi:10.1086/521260
Bouza E, Pérez A, Muñoz P, Jesús Pérez M, Rincón C, Sánchez C, Martín-Rabadán P, Riesgo M; Cardiovascular Infection Study Group (2003) Ventilator-associated pneumonia after heart surgery: a prospective analysis and the value of surveillance. Crit Care Med 31:1964–1970
Hayon J, Figliolini C, Combes A, Trouillet J-L, Kassis N, Dombret MC, Gibert C, Chastre J (2002) Role of serial routine microbiologic culture results in the initial management of ventilator-associated pneumonia. Am J Respir Crit Care Med 165:41–46
Sanders KM, Adhikari NKJ, Friedrich JO, Day A, Jiang X, Heyland D; Canadian Critical Care Trials Group (2008) Previous cultures are not clinically useful for guiding empiric antibiotics in suspected ventilator-associated pneumonia: secondary analysis from a randomized trial. J Crit Care 23:58–63
Deresinski S (2007) Principles of antibiotic therapy in severe infections: optimizing the therapeutic approach by use of laboratory and clinical data. Clin Infect Dis 45:S177–S183. doi:10.1086/519472
Kollef Marin H (2000) Inadequate antimicrobial treatment: an important determinant of outcome for hospitalized patients. Clin Infect Dis 31:S131–S138. doi:10.1086/314079
McGinigle KL, Gourlay ML, Buchanan IB (2008) The use of active surveillance cultures in adult intensive care units to reduce methicillin-resistant Staphylococcus aureus-related morbidity, mortality, and costs: a systematic review. Clin Infect Dis 46:1717–1725. doi:10.1086/587901
Tacconelli E (2009) Screening and isolation for infection control. J Hosp Infect 73:371–377
Weber SG, Huang SS, Oriola S, Huskins WC, Noskin GA, Harriman K, Olmsted RN, Bonten M, Lundstrom T, Climo MW, Roghmann M-C, Murphy CL, Karchmer TB (2007) Legislative mandates for use of active surveillance cultures to screen for methicillin-resistant Staphylococcus aureus and vancomycin-resistant enterococci: position statement from the Joint SHEA and APIC Task Force. Am J Infect Control 35:73–85
Centers for Disease Control and Prevention (CDC) (2009) Guidance for control of infections with carbapenem-resistant or carbapenemase-producing Enterobacteriaceae in acute care facilities. MMWR Morb Mortal Wkly Rep 58:256–260
Siegel JD, Rhinehart E, Jackson M, Chiarello L; Healthcare Infection Control Practices Advisory Committee (2007) Management of multidrug-resistant organisms in health care settings, 2006. Am J Infect Control 35:S165–S193
Cohen AL, Calfee D, Fridkin SK, Huang SS, Jernigan JA, Lautenbach E, Oriola S, Ramsey KM, Salgado CD, Weinstein RA; Society for Healthcare Epidemiology of America and the Healthcare Infection Control Practices Advisory Committee (2008) Recommendations for metrics for multidrug-resistant organisms in healthcare settings: SHEA/HICPAC Position paper. Infect Control Hosp Epidemiol 29:901–913. doi:10.1086/591741
Acknowledgements
We thank the intensive care unit (ICU) nursing staff and microbiology scientific staff for their ongoing efforts at controlling infections in critically ill patients.
Conflict of interest
All authors report no conflicts of interest relevant to this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Baba, H., Nimmo, G.R., Allworth, A.M. et al. The role of surveillance cultures in the prediction of susceptibility patterns of Gram-negative bacilli in the intensive care unit. Eur J Clin Microbiol Infect Dis 30, 739–744 (2011). https://doi.org/10.1007/s10096-010-1146-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10096-010-1146-1