
Abstract
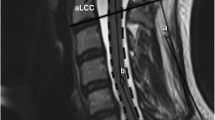
Although flexion cervical MRI has been recommended for the diagnosis of Hirayama disease (HD), no study focused on the MR features at different neck flexion angles. Moreover, no uniform flexion angle has been confirmed in clinical practice. The purpose of this study is to quantitatively investigate the MRI typical signs of HD patients in different neck flexion degree and gives a suggestion to the MR scanning. Cervical MRI in neutral and different flexion positions (cervical flexion angle 20°, 25°, 30°, 35°, and 40°) were performed in 45 HD patients. Three MRI features including anterior shifting of the posterior wall of the cervical dural canal (ASD), widening of cervical epidural space, and epidural flow voids (EFV) at each flexed position were summarized. To evaluate ASD quantitatively, the widest cervical epidural space with the maximum sagittal diameters (d) and cervical canal sagittal diameter (D) at the same level were measured. The d/D values at different angles were calculated and compared. ASD was demonstrated in 34 out of 45 cases (75.6%) at 20° and in all cases (100%) at other 4 angles (χ 2 = 25.728, P < 0.05). Significant difference was demonstrated for the appearance rate of EFV (mean 72.8%) among different angles (χ 2 = 11.373, P = 0.021). The peak mean d/D value was found at 35°. Neck flexion angles have effects on ASD, widening of cervical epidural space and EFV. 25° is recommended as the least effective diagnostic flexion angle for MRI diagnosis of HD, and 35° may be the best one.




Similar content being viewed by others


Abbreviations
- HD:
-
Hirayama disease
- ASD:
-
Anterior shifting of the posterior wall of the cervical dural canal
- EFV:
-
Epidural flow voids
- RF:
-
Radiofrequency
References
Fu Y, Pei X, Zhang J, Kang D, Han H, Fan D (2008) Morphological changes of the lower cervical spinal cord under neutral and fully flexed position by MRI in Chinese patients with Hirayama’s disease. Amyotroph Lateral Scler 9:156–162
Robberecht W, Aguirre T, VandenBosch L et al (1997) Familial juvenile focal amyotrophy of the upper extremity (Hirayama disease)—Superoxide dismutase 1 genotype and activity. Arch Neurol Chicago 54:46–50
Schroder R, Keller E, Flacke S et al (1999) MRI findings in Hirayama’s disease: flexion-induced cervical myelopathy or intrinsic motor neuron disease? J Neurol 246:1069–1074
Hirayama K, Tokumaru Y (2000) Cervical dural sac and spinal cord in juvenile muscular atrophy of distal upper extremity. Neurology 54:1922–1926
Chen CJ, Chen CM, Wu CL, Ro LS, Chen ST, Lee TH (1998) Hirayama disease: MR diagnosis. Am J Neuroradiol 19:365–368
Baba Y, Nakajima M, Utsunomiya H et al (2004) Magnetic resonance imaging of thoracic epidural venous dilation in Hirayama disease. Neurology 62:1426–1428
Sonwalkar HA, Shah RS, Khan FK et al (2008) Imaging features in Hirayama disease. Neurol India 56:22–26
Pei X, Han H, Xie J et al (2006) Dynamic magnetic resonance imaging study on Hirayama disease. Chin J Med Imaging Technol 26:1255–1257
Liu H, Li C, He D et al (2006) The diagnosis of a fully flexed neck position MRI diagnosis in juvenile muscular atrophy of the distal upper extremity. Chin J Radiol 40:745–747
Fu Y, Fan D, Pei X et al (2007) MRI diagnosis of Hirayama disease. Chin J Radiol 41:352–355
Hirayama K (1991) Non-progressive juvenile spinal muscular atrophy of the distal upper limb (Hirayama’s disease). In: De Jong JM (ed.) Handbook of clinical neurology. Vol 15. Elsevier, Amsterdam, pp 107–120
Bossuyt PM, Reitsma JB, Bruns DE (2003) Towards complete and accurate reporting of studies of diagnostic accuracy: the STARD initiative. Radiology 226:24–28
Takeshita K, Peterson ET, Bylski-Austrow D, Crawford AH, Nakamura K (2004) The nuchal ligament restrains cervical spine flexion. Spine 29((Phila Pa 1976)):E388–E393
Patel TR, Chiocca EA, Freimer ML, Christoforidis GA (2009) Lack of epidural pressure change with neck flexion in a patient with Hirayama disease: case report. Neurosurgery 64:1196–1197
Acknowledgments
This research was founded by Program for New Century Excellent Talents in University (Grant number: NCET-05-0019), National Natural Science Foundation of China (Grant number: 30972811) and Beijing municipal commission of education.
Author information
Authors and Affiliations
Corresponding author
Additional information
C. Hou, X. Yang, X. Xu and H. Gao contributed equally to this work.
Rights and permissions
About this article
Cite this article
Hou, C., Han, H., Yang, X. et al. How does the neck flexion affect the cervical MRI features of Hirayama disease?. Neurol Sci 33, 1101–1105 (2012). https://doi.org/10.1007/s10072-011-0912-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-011-0912-x