
Abstract
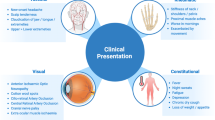
Prompt institution of corticosteroids (CS) can prevent devastating neuro-ophthalmic complications (NOC) in patients with giant cell arteritis (GCA). Guidelines on managing GCA place emphasis on early recognition of symptoms and prompt treatment of the disease where there is a high index of clinical suspicion. The aims of this study are to review the clinical findings in patients with GCA, evaluate the baseline practice in diagnosis and treatment and to identify delays in treating patients with NOC. The study utilised retrospective case notes review of patients diagnosed with GCA between 2003 and 2008. Sixty-five patients were identified (47 females, 18 males, mean age, 75 years). A significant minority presented with constitutional, polymyalgic and ischaemic symptoms. Mean time from symptom onset to diagnosis of GCA was 35 days. CS were not delayed in those diagnosed with GCA. Recognition of ischaemic symptoms was slow. Visual loss at presentation occurred in 16 patients (24.6%). Ten patients (15.4%) presented with NOC in the absence of headache, seven (70%) of whom developed permanent visual impairment. Five (7.7%) patients had cerebrovascular complications. There are major delays in the recognition and treatment of GCA. There is a high incidence of irreversible ischaemic complications which may partly result from diagnostic and treatment delay.
Similar content being viewed by others

References
Borg FA, Salter VL, Dasgupta B (2008) Neuro-ophthalmic complications in giant cell arteritis. Curr Allergy Asthma Rep 8:323–330
Gonzalez-Gay MA, Garcia-Porrua C, Llorca J et al (2000) Visual manifestations of giant cell arteritis. Trends and clinical spectrum in 161 patients. Med Baltim 79:283–292
Liozon E, Herrmann F, Ly K et al (2001) Risk factors for visual loss in giant cell (temporal) arteritis: a prospective study of 174 patients. Am J Med 111:211–217
Sandercock PA, Warlow CP, Jones LN, Starkey IR (1989) Predisposing factors for cerebral infarction: the Oxfordshire community stroke project. BMJ 298:75–80
Goodman BW Jr (1979) Temporal arteritis. Am J Med 67:839–852
Font C, Cid MC, Coll-Vinent B, Lopez-Soto A, Grau JM (1997) Clinical features in patients with permanent visual loss due to biopsy-proven giant cell arteritis. Br J Rheumatol 36:251–254
Danesh-Meyer H, Savino PJ, Gamble GG (2005) Poor prognosis of visual outcome after visual loss from giant cell arteritis. Ophthalmology 112:1098–1103
Smetana GW, Shmerling RH (2002) Does this patient have temporal arteritis? JAMA 287:92–101
Nesher G, Berkun Y, Mates M et al (2004) Risk factors for cranial ischemic complications in giant cell arteritis. Med Baltim 83:114–122
The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group (1995) Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 333:1581–1587
Hacke W, Kaste M, Bluhmki E et al (2008) Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med 359:1317–1329
Dasgupta B, Hassan N, British Society for Rheumatology Guidelines Group (2007) Giant cell arteritis: recent advances and guidelines for management. Clin Exp Rheumatol 25:S62–S65
Dasgupta B, Giant Cell Arteritis Guideline Development Group (2010) Concise guidance: diagnosis and management of giant cell arteritis. Clin Med 10:381–386
Mukhtyar C, Guillevin L, Cid MC et al (2009) EULAR recommendations for the management of primary small and medium vessel vasculitis. Ann Rheum Dis 68:310–317
Hunder GG, Bloch DA, Michel BA et al (1990) The American College of Rheumatology 1990 criteria for the classification of giant cell arteritis. Arthritis Rheum 33:1122–1128
Cid MC, Font C, Oristrell J et al (1998) Association between strong inflammatory response and low risk of developing visual loss and other cranial ischemic complications in giant cell (temporal) arteritis. Arthritis Rheum 41:26–32
Hernandez-Rodriguez J, Segarra M, Vilardell C et al (2003) Elevated production of interleukin-6 is associated with a lower incidence of disease-related ischemic events in patients with giant-cell arteritis: angiogenic activity of interleukin-6 as a potential protective mechanism. Circulation 107:2428–2434
Acknowledgements
Thanks to Yvonne Townsend, Research and Audit Department, Southend University Hospital NHS Trust.
Disclosures
None
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ezeonyeji, A.N., Borg, F.A. & Dasgupta, B. Delays in recognition and management of giant cell arteritis: results from a retrospective audit. Clin Rheumatol 30, 259–262 (2011). https://doi.org/10.1007/s10067-010-1616-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-010-1616-y