
Abstract
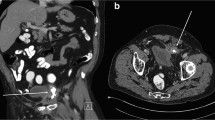
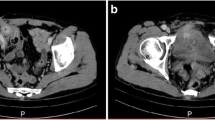
Tension-free and sutureless hernioplasty by plug and mesh of nonreabsorbable material is one of the most common techniques for inguinal hernia repair. It’s a simple and quick procedure with a low cost and allows for a short hospital stay. It shows a low reoccurrence rate, but it can result, in very few cases, in complications strictly related to prosthetic material. The literature describes some cases of plug migration from its proper position, for example, to the scrotum, preperitoneal adipose tissue, and abdominal cavity. We report on a case of sigmoid colon perforation due to a plug of Trabucco hernioplasty performed 2 years previously.


Similar content being viewed by others

References
LeBlanc KA (2001) Complications associated with the plug-and-mesh method of inguinal hernioplasty. Hernia 5:135–138
Zanghi G, Biondi A, Di Mauro G, Caruso G, Basile G, Catalano F, Basile F (2001) The polypropylene wall in the surgical treatment of inguinal hernia and crural: our experience on 500 cases. Ann Ital Chir 72:449–452
Dieter RA (1999) Mesh plug migration in scrotum: a new complication of hernia repair. Int Surg 84:57–59
Chuback JA, Singh RS, Sills C, Dick LS (2000) Small bowel obstruction resulting from mesh plug migration after open inguinal hernia repair. Surgery 127:475–476
Majeski J (1998) Migration of wire mesh into the intestinal lumen causing an intestinal obstruction 30 years after repair of a ventral hernia. South Med J 91:496–498
Miller K, Junger W (1997) Ileo-cutaneous fistula formation following laproscopic polypropylene mesh hernia repair. Surg Endosc 11:772–773
Bodenbach M, Bschleipfer T, Stoschek M, Beckert R, Sparwasser C (2002) Intravescical migration of a polypropylene mesh implant after laproscopic transperitoneal hernioplasty. Urologe A 41:366–368
Rieger N, Brundell S (2002) Colo-vescical fistula secondary to laproscopic trans-abdominal preperitoneal polypropylene mesh hernioplasty. Surg Endosc 16:218–219
Aldridge AJ, Simpson JNL (2001) Erosion and perforation of colon by synthetic mesh in a recurrent paracolostomy hernia. Hernia 5:110–112
Fernandez Lobato R, Martinez Santos C, Ortega Deballon P, Fradejas Lopez JM, Marin Lucas FJ, Moreno Azcoita M (2001) Colocutaneous fistula due to polypropylene mesh. Hernia 5:107–109
Losanoff JE, Richman BW, Jones JW (2002) Entero-colocutaneous fistula: A late consequence of polypropylene mesh abdominal wall repair: Case report and review of the literature. Hernia 6:144–147
Festa V, Rollino R, Baracchi F, Morino M, Morino F, Trabucco E (2002) Use of the “flat mesh” T4r in the Trabucco inguinal hernioplasty. Technical note. Minerva Chir 57(5): 707–710
Trabucco EE (2000) Sutureless inguinal mesh ernioplasty. Osp Ital Chir 6:225–232
Acknowledgments
Despite their relative rarity, the major complications of inguinal hernioplasty assume great importance if we look at the number of interventions performed. Every year in the United States, there are 700,000 patients operated on for inguinal hernias, and if 1.1% encounter generic complications, 7,000 cases have nonregular periods.
The case that we observed—fortunately the only one and unique for its gravity—confirms that there is no scale of importance in surgical interventions; this should not be a critique of the prosthetic hernioplasty technique, rather only an occasion to remember that the danger of the unexpected is frequently hidden in the most simple and common situations.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Benedetti, M., Albertario, S., Niebel, T. et al. Intestinal perforation as a long-term complication of plug and mesh inguinal hernioplasty: Case report. Hernia 9, 93–95 (2005). https://doi.org/10.1007/s10029-004-0256-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10029-004-0256-z