
Abstract
Background
Internalizing psychopathology, anxiety in particular, is assumed to contribute to the development of gender Identity disorder (GID). Until now, anxiety has only been reported in studies using parent-report questionnaires; physiological correlates of anxiety have not been studied. In this study we assessed anxiety and stress in children with GID by measuring their cortisol, heart rate (HR) and skin conductance levels (SCL) and asking them to repeat their moods and experience of control.
Methods
By using an established psychological challenge, involving provocation and frustration, we investigated whether children with GID as compared to healthy controls react in a more anxious way under these experimental circumstances. We assessed anxiety levels in 25 children with GID and 25 matched controls by measuring cortisol, HR and skin conductance and examined whether a pattern of increased physiological activity corresponded with the feeling of being less in control and having more intense negative emotions.
Results
The results showed that children with GID had more negative emotions and a tonically elevated SCL. There were no differences between the groups in cortisol and HR.
Conclusion
This is the first study that shows that children with GID have a more anxious nature as compared to their normal counterparts.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Children diagnosed with a gender identity disorder (GID) experience feelings of belonging to the other sex. They have a strong cross-gender identification and a persistent discomfort with their biological sex or gender role associated with their sex.
For a better understanding of the development of GID, Zucker and Bradley [26] hypothesized a model in which child-, parent- and family factors either have an interactive or an additive effect on the development of GID. In this model, GID is largely determined by anxiety in the child (For a detailed description of this model see [26]). It is proposed that anxiety is a result of an innate vulnerability to elevated arousal in response to stressful or challenging situations. This anxiety produces a situation in which the child experiences an intense need for anxiety reduction. If there is a context in which he or she perceives that the opposite-sex role provides a sense of safety or security, the defensive solution to deal with the anxiety can be found in the other sex. It is possible that children with an atypical gender development perceive the other sex as more secure, safe or valued and try to reduce the perceived anxiety by behaving in accordance to the other sex [26]. Studies that used a parent report questionnaire measuring emotional and behavior problems in the child, the Child Behavior Checklist (CBCL) indeed showed a predominance of internalizing problems in children with GID [26]. However, from these parent-report studies we do not know if children with GID generally react in a more anxious way to stressful and challenging situations than control children. As a number of studies consider physiological responses [hypothalamic-pituitary-adrenal (HPA) axis response, heart rate (bpm), skin conductance levels (SCL)] as indices of anxiety proneness [6, 20, 21] we wanted to assess anxiety levels in 25 GID children by measuring physiological correlates of anxiety.
During stress, activation of the HPA system results in the release of the steroid hormone cortisol from the adrenal gland. There is evidence that an elevation in children’s cortisol is related to internalizing problems [3, 15, 16, 21]. A study by Ashman et al. [3] found that children who were reported to have internalizing symptoms were also more likely to show an elevated stress response to a mild laboratory stressor. Granger et al. [15, 16] found that the cortisol increase in response to a conflict-inducing task was associated with social withdrawal, social anxiety and socially inhibited behavior during the task, and also predicted children’s internalizing problem behaviors and anxiety disorders at follow-up. Another finding that also points to an association between an elevated cortisol concentrations and internalizing behavior is that of Schmidt et al. [21]. This study showed that 4-year olds who showed several wary behaviors during peer play had relatively high morning salivary cortisol levels. At 14 months of age these children had been reported to be shy and behaviorally inhibited.
There is also evidence that heart rate (HR) measured in beats per minute indicates a anxious nature. Battaglia et al. [4] found that children born to parents with a panic disorder showed increased behavioral inhibition and higher HR when exposed to novel and mildly stressful situations. A study by Schmidt et al. [22] showed that shy children had significantly greater HR increases during a task designed to elicit self-presentation anxiety compared to non-shy children. This finding is consistent with findings by Beidel [6], that children with clinically significant test anxiety had higher HRs during two social-evaluative tasks than their non-anxious peers.
From adult studies it is known that SCLs are influenced by emotional arousal and are higher in anxious individuals. However, child studies that used skin conductance as an objective measurement for assessing anxiety responses or for indicating behavioral inhibition, all used different stimuli and different paradigms for assessing skin conductance. Consequently, the findings of these child studies are more disparate than the findings from adult studies. For example, Cole et al. [10] tried to predict if emotion regulation in 5-year olds, indexed by types of facial expressivity, was associated with different patterns of autonomic activity during negative mood induction procedure. There was a significant effect of the expressive group on average change in skin conductance and the average change in skin conductance was significantly different between the inexpressive and the expressive groups of children during film clips that induced negative emotion. This study shows that inexpressive children had significant less change in skin conductance during film clips that induced negative emotion [10]. Another study of Scarpa et al. [20] found, for example, that 3-year-old inhibited children had a significant higher SCL than 3-year-old uninhibited children while they listened to a standard stimulus auditory tape consisting of stimuli that were selected to elicit an orienting response. However, Fowles et al. [12] found no increase in skin conductance when 4-year-old children were exposed to emotional film clips.
The aim of the present study was to find out whether children with GID have increased physiological activity during stress. We also examined whether a pattern of increased physiological activity corresponds with stronger feelings of having no control and more intense negative emotions. By using an established psychological challenge, involving provocation and frustration, we investigated whether children with GID as compared to healthy controls react in a more anxious way under these experimental circumstances.
Method
The study was approved by the Medical Ethical Committee of University Medical Center Utrecht, and parents gave written informed consent.
Subjects
Subjects (n = 50: 25 matched controls [MC] and 25 children with a GID) were Caucasian and aged between 7 and 12 years (mean age GID group = 9.3 years; mean age MC group = 10.2 years; F 1,48 = 6.68, P < 0.02). The control children were recruited from grades 3 to 6 of regular local elementary schools. The 25 control children were selected from a larger sample of 62 volunteers and parental permission for participation was obtained. Of these 62 control children, 20 boys and 5 girls were selected as matched sex controls to the children with GID. The parents of the matched control children were asked whether their children (ever) had any psychiatric complaints. There were no children with psychiatric complaints. The GID group (n = 25) consisted of boys (n = 20) and girls (n = 5) who had met the criteria for GID as set out in the DSM-IV [2]. The GID group was solicited from the Gender Identity Clinic, which was housed within the Department of Child and Adolescent Psychiatry at the University Medical Center Utrecht. These children were solicited from a cohort children referred to the Gender Identity Clinic in a period of 6 years.
Diagnoses of the GID subjects were based on standardized procedures including psychological assessment of the child, interviews with the child and interviews with the parents on the child’s developmental history and current functioning, family functioning and family history of the parents (for a detailed description of the procedure and instruments used see [9]). Exclusion criterion was an IQ less than 75.
Procedure
Non-stress phase. The participants spent 30 min filling in questionnaires and watching (e.g., Disney) cartoons. These film clips were shown in order to get used to the situation and attain reliable psychophysiological baseline levels. Stress phase. Stress was induced for 65 min and involved social stress (anxiety for failure). The stress was induced by competition between the real participant and a videotaped opponent of similar age and sex, who competed with the participant for best performance (see for details [13, 14]). The participant had to perform a difficult computer task under time pressure while the video-opponent was “watching” his/her performance. The computer task was standardized by using a videotape of the competitor, who criticized the performance of the participant in a competitive and derogatory way. Furthermore, the task was programmed in such a way that the participant could only perform badly. After the first badly performance, the participants were told by the video-opponent to do the task once more. The second time the task was made to be even more frustrating. An opportunity for a reaction was provided after he or she had been provoked twice by the competitor. None of the participants were aware that the video-opponent was not a real subject [13, 14]. Non-stress phase. During the final 30 min, the participant filled in questionnaires, watched videos, and was told he or she was the winner of the competition.
The CBCL was completed shortly before the control children’s participation in the study by their parents and shortly before the psychological assessment of the children with GID. The CBCL data were used to find out whether the GID group was representative for the entire cohort and to screen the control children. The CBCL data at the time of the study are reported in the “Results” section.
Procedure for saliva cortisol collection and analysis
Each subject participated in the experiment between 1:00 P.M. and 4:00 P.M. because afternoon values do not strongly decrease over time and are more clearly influenced by external stimulation. All the time points of measurement (matching specific tasks) were the same for HR, skin conductance and the psychological states. Moreover, six saliva samples were taken. The effect of stress exposure on cortisol reactivity has been shown in the Van Goozen et al. [14] study.
Saliva samples, collected in plastic vials after saliva production was stimulated with citric acid, were stored at −20°C until analysis. Cortisol concentrations were measured without extraction using an in-house competitive radio immunoassay with a polyclonal anticortisol antibody (K7348). [1,2-3H (N)] Hydrocortisone (NET 185, NEN DuPont, Dreiech, Germany) was used as a tracer after chromatographic verification of its purity. The lower limit of detection was 0.5 nmol/l, and interassay variation was 11.0%, 8.2%, and 7.6% at 4.7, 9.7, and 14.0 nmol/l, respectively (n = 20). Saliva cortisol levels correlate highly with serum cortisol concentrations and reflect the unbound fraction of circulation cortisol.
Procedure for skin conductance and heart rate measurement
Participants were seated throughout the session and asked to sit still. Electrodermal activity (SC4 skin conductance; Contact Precision Instruments, London) was recorded by a constant-voltage (0.5 V) method from the distal phalanges of the middle and ring fingers of the non-dominant hand using Ag/AgCl electrodes with electrode collars of 0.5 cm in diameter, which were filled with Hewlett-Packard Redux Creme. Before each recording session the skin conductance coupler was calibrated to map activity from 0 to approximately 52 microsiemens. A finger pulse amplifier (photoplethysmograph; Contact Precision Instruments) for the recording of HR was fixed to the index finger of the non-dominant hand. HR was expressed in the number of beats per minute (bpm). SCL and HR were recorded continuously during 5 events, matching specific tasks. After the competition was over, the equipment was switched off and the electrodes were detached.
Recording of psychological states
Children rated their feelings five times. An adaptation for children of a clinical self-rating scale was used [24]. A negative feeling score per event was calculated by adding scores of nine dichotomous items (“ I feel: happy/gloomy, well/sick, cheerful/not cheerful, good/bad, loved/not loved, satisfied/not satisfied, afraid/not afraid, strong/weak, angry/not angry”; [14, 24]). They also indicated five times on a 7-point rating scale how much they felt in control of the situation. Specifically they reported after each task whether they expected to win or lose the competition.
Statistical analysis
For the CBCL scales, T-scores were computed and used in analyses. To see if the participating children were representative of the complete cohort, we compared the mean scores on the Total-, Internalizing-, and Externalizing scale of the CBCL [1] of the participating GID group and 31 non-participating children from the same cohort. Mann–Whitney analysis was used to see if there were significant differences on the Total, Internalizing and Externalizing scale. One-factor analyses of variance were used to assess the effect of diagnostic group on CBCL factors, both broad-band and narrow-band.
Repeated-measures multivariate analyses of variance (MANOVAs) with group (GID versus matched controls, hereafter MC) as between-subjects factor and time as within-subjects factor were used to assess changes in levels of cortisol, skin conductance and HR, negative mood, and feelings of control. We used a one-way analyses of variance with baseline level as dependent variable and group (GID versus MC) as factor to assess if the two groups showed a different pattern of autonomic arousal and HPA activity at baseline. The first measurement is the baseline measurement and the stress value is the mean of the following four.
To analyze the magnitude of the stress task we computed effect sizes (ES) in accordance with Cohen (1977) (Cohen’s d) for cortisol values, HR, SCL, negative feelings and feelings of control. We computed the ES with use of the original standard deviation and compared the mean of the dependent variable of the GID and the MC group during the stress phase. Values of ES 0.8 is considered to be large, ES 0.5 is medium and ES 0.2 is small [7].
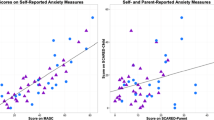
Pearson correlations were used to examine whether baseline values and stress-induced changes in biological variables correlated with CBCL factors and subjectively reported feelings.
Results
Clinical characteristics
Age was not significant correlated with cortisol, HR, SCl, negative feelings and feelings of control and was therefore not included in the analyses.
Mann–Whitney analysis showed no significant differences on the Total, Internalizing and Externalizing scale between the participating children with GID and 31 non-participating children belonging to the same cohort.
The GID group differed significantly from the MC group in their mean T-score on the CBCL Anxious/Depressed scale (F 1,48 = 7.09, P = 0.01), the Attention Problems scale (F 1,48 = 9.785, P < 0.01), the Delinquent scale (F 1,48 = 5.55, P < 0.05), and the Aggressive scale (F 1,48 = 4.99, P < 0.05). Also, the groups differed in internalizing (F 1,48 = 10.39, P < 0.01) and externalizing behavior (F 1,48 = 5.62, P < 0.05) (see Table 1).
Differences between children with GID and control children
Cortisol
One-way ANOVA revealed a significant difference between baseline cortisol values of both groups (M mc = 7.02, M gid = 5.27; F 1,49 = 8.26, P = 0.006); the cortisol values of the MC group were higher than the cortisol values of the GID group. In both groups the values increased during the task.
A repeated-measures MANOVA over all six samples revealed a main effect of time (F 5,48 = 3.80, P = 0.024) (Cohen’s d = 0.88), no effect of group (F 1,48 = 1.44, NS) and no interaction between group and time (F 5,48 = 0.31, NS).
There were no significant correlations between cortisol and CBCL factors, nor between cortisol and negative mood or feelings of control at baseline and during stress in both groups.
Heart rate
There was no difference in HR (bpm) (M mc = 92.55, M GID = 89.36; F 1,49 = 1.28, NS) at baseline and in both groups HR increased during stress.
A repeated-measures MANOVA indicated a significant main effect of time (F 4,48 = 12.26, P < 0.001) (Cohen’s d = 0.28), but no main effect of group (F 1,48 = 0.66, NS) nor an interaction (F 4,48 = 1.39, NS) between group and time. There were no significant correlations between HR and CBCL measures, nor between HR and negative mood or feelings of control at baseline or during the stress task in both groups.
Skin conductance level
There was a difference in SCL (M mc = 17.60, M GID = 23.47; F 1,48 = 4.60, P = 0.037) at baseline; SCL was higher in the GID group. SCL increased in both groups during stress. A repeated-measures MANOVA indicated a significant main effect of time (F 4,46 = 113.10, P = 0.001) (Cohen’s d = 0.88), a main effect of group (F 1,46 = 4.71, P = 0.035) but no interaction between group and time (F 4,46 = 0.43, NS). There were no significant correlations between SCL and CBCL measures or between SCL and negative mood or feelings of control during stress and baseline in both groups.
Negative mood and feelings of control
Figure 1 shows that the reported intensity of negative moods increased more strongly in the GID group as a result of stress. There was a difference in negative mood (M mc = 5.76, M GID = 3.25; F 1,49 = 14.68, P < 0.001) at baseline. A repeated-measures MANOVA indicated a significant interaction between group and time (F 4,48 = 7.65, P < 0.001) and a main effect of time (F 4,48 = 13.76, P < 0.001) (Cohen’s d = 0.13). There was no main effect of group (F 1,48 = 1.13, NS) (see Fig. 1).

Negative feelings in children with GID and matched control children. GID = gender identity disorder; MC = matched controls
With respect to feelings of control, there was a difference (M mc = 4.64, M GID = 4.12, F 1,49 = 6.15, P = 0.017) at baseline, with the GID group reporting feeling less in control. Moreover, there was a significant interaction effect between group and time (F 4,47 = 2.70, P = 0.032) and a main effect of time (F 4,47 = 22.84, P < 0.001) (Cohen’s = 0.87); and a main effect of group (F 1,47 = 8.88, P = 0.005). In both groups feelings of control were influenced by stress. The expectation of losing increased while stress was induced and the expectation of winning increased after the stress had ended, in the second non-stress phase. However, this pattern was more pronounced in the GID group (see Fig. 2).

Controllability in children with GID and matched control children. GID = gender identity disorder; MC = matched controls
Discussion
The aim of the current study was to compare HPA axis functioning and autonomic nervous system (ANS) activity in 25 children with a GID and 25 matched controls under stressful and non-stressful conditions.
The results proceeded from the participating group children with GID point to a discrepancy between the physiological and psychological measurements of stress. Although, the children with GID were not different from matched control children with respect to HPA axis functioning and ANS activity when exposed to stress, they did report stronger negative moods and felt more out of control during stress as compared to their normal counterparts (see Figs. 1, 2). Furthermore, the results showed a tonically elevated SCL in children with GID that could not be explained as a result of stress.
Cognitive models of fear use two cognitive dimensions to describe the process of becoming anxious. The first one is the appraisal of the situation (i.e. is the situation challenging?) and the second one is the appraisal of one’s own ability to cope with the situation (i.e. do I have the situation under control?) [5, 25]. The results of our study showed that anxious patterns do not seem to be present on all levels of physiological functioning in children with GID. However, the results show that the children with GID had different perceptions of the task than the control children did; the children with GID experienced more negative feelings and feelings of being less in control than the control children. In view of the cognitive models of fear, we think that this result points to an underestimation of their ability to cope with the stress situation (second dimension in the cognitive model). Furthermore, earlier research showed that a high level of anxiety in children was accompanied by a high level of negative feelings and cognitions, assessed by means of a self-report measure [18]. As our results also showed that children with GID experienced more negative feelings, we think that this result is in line with the Muris et al. [18] study and points to a more anxious nature in children with GID. The absence of a physiological reaction in children with GID can be explained by the first dimension of the cognitive model; the children with GID may not have appraised this particular stress task as more challenging than the control children. Perhaps a different type of stressor (e.g., anxiety for ostracism instead of anxiety for failure) addressing other kinds of internalizing problems would have resulted in a different physiological reaction in children with GID. Internalizing problems are disturbances of emotion or behavioral deficits (e.g. anxiety, social withdrawal and depression). Unfortunately, we know very little about the prevalence of anxiety and mood disorders among children with GID. Although researchers (e.g. [8, 26]) have reported a predominance of internalizing problems in children with GID, we do not know exactly which psychiatric disorders are prevalent among children with GID. Further research has to focus on specification of internalizing disorders among children with GID.
In GID children SCLs were found to be higher not only during baseline measurement conditions, but also during stress. Studies have specifically linked reduced skin conductance levels or reduced skin conductance reactivity to a pathological lack of fear (fearlessness), as seen in sensation-seekers and psychopaths [17, 19] or in children with a conduct disorder [14, 23]. From this point of view a high level of SCL could point to a more anxious, inhibited and cautions nature. Furthermore, SCL is a pure measure of emotional arousal and it provides a direct reflection of sympathetic activity [11, 20]. Therefore it is possible that a tonically elevated SC level reflects a more anxious temperament in children with GID.
Limitation
On entrance, we found that the children in the MC group had higher levels of cortisol. This result can be explained by the fact that the children with GID had visited the gender clinic frequently, and even had been through several testing occasions and were therefore more familiarized with the current research setting than the control children. It is possible that the children in the MC group were more nervous at baseline, which was reflected in their higher initial cortisol values. However, we do not think that our conclusions should be revised because of this result. The pattern of cortisol release in children with GID turned out not to be very different form the pattern found in the MC group.
To summarize, internalizing problems and especially anxiety have been repeatedly reported in studies using parent-report questionnaires. The present study showed that children with GID did not react in a typically anxious way with regard to two physical correlates of anxiousness; cortisol and HR. However, the tonically elevated skin conductance and the more negative appraisals of the stress situation and one’s own ability to deal with the stress situation, may be an indication of a more anxious nature in children with GID than in children without GID.
References
Achenbach TM (1991) Manual for the child behavior checklist and 1991 profile. University of Vermont Department of Psychiatry, Burlington
American Psychiatric Association (1994) Diagnostic and statistical manual of mental disorders, 4th edn. (DSM-IV). American Psychiatric Association, Washington, DC
Ashman AB, Dawson G, Panagiotides H, Yamada E, Wilkinson CW (2002) Stress hormone levels of children of depressed mothers. Dev Psychopathol 14:333–349
Battaglia M, Bajo S, Strambi LF, Brambilla F, Castronovo C, Vanni G, Bellodi L (1997) Physiological and behavioral responses to minor stressors in offspring of patients with panic disorder. J Psychiatr Res 31:365–376
Beck AR, Emery G, Greenber RL (1985) Anxiety disorders and phobias: a cognitive perspective. Basic Books, New York
Beidel DC (1988) Psychophysiological assessment of anxious emotional states in children. J Abnorm Psychol 97:80–82
Cohen J (1988) Statistical power of analysis for the behavioural sciences, 2nd edn. Lawrence Earlbaum Associates, Hillsdale, NJ
Cohen-Kettenis PT, Owen A, Kaijser VG, Bradley SJ, Zucker KJ (2002) Demographic characteristics, social competence, and behavior problems in children with gender identity disorder: a cross-national, cross-clinic comparative analysis. J Abnorm Child Psychol 31:41–53
Cohen-Kettenis PT, Pfäfflin F (2003) Transgenderism and intersexuality in childhood and adolescence. Sage Publications, California, London, New Delhi
Cole PM, Zahn-Waxler C, Usher BA, Welsh JD, Fox NA (1996) Individual differences in emotion regulation and behavior problems in preschool children. J Abnorm Psychol 105:518–529
Dawson ME, Schell AM, Fillion DL (1990) The electrodermal system. In: Cacioppo JT, Tassinary LG (eds) Principles of psychophysiology: physical, social, and inferential elements. Cambridge University Press, New York, pp 295–324
Fowles DC, Kochanska G, Murray K (2000) Electrodermal activity and temperament in preschool children. Psychophysiology 37:777–787
van Goozen SHM, Matthys W, Cohen-Kettenis PT, Gispen-de Wied C, Wiegant VM, van Engeland H (1998) Salivary cortisol and cardiovascular activity during stress in oppositional-defiant disorder boys and normal controls. Biol Psychiatry 43:531–539
van Goozen SHM, Matthys W, Cohen-Kettenis PT, Buitelaar JK, van Engeland H (2000) Hypothalamic-pituitary-adrenal axis and autonomic nervous system activity in disruptive children and matched controls. J Am Acad Child Adolesc Psychiatry 39:1438–1445
Granger DA, Weisz JR, Kauneckis D (1994) Neuroendocrine reactivity, internalizing behavior problems, and control-related cognitions in clinic-referred children and adolescents. J Abnorm Psychol 103:267–276
Granger DA, Weisz JR, McCracken JT, Ikeda SC, Douglas P (1996) Reciprocal influences among adrenocortical activation, psychosocial processes, and the behavioral adjustment of clinic-referred children. Child Dev 67:3250–3262
Herpetz SC, Mueller B, Wenning B, Qunaibi M, Lichterfeld C, Herpetz-Dahlmann B (2003) Autonomic responses in boys with externalising disorders. J Neural Transm 110:1181–1195
Muris O, Luermans J, Merckelbach H, Mayer B (2000) “Danger is lurking everywhere”. The relation between anxiety and threat perception abnormalities in normal children. J Behav Ther Exp Psychiatry 31:123–136
Raine A (1993) The psychopathology of crime: criminal behavior as a clinical disorder. Academic Press, San Diego
Scarpa A, Raine A, Mednick SA, Venables PH (1997) Heart rate and skin conductance in behaviorally inhibited Mauritian children. J Abnorm Psychol 106:182–190
Schmidt LA, Fox NA, Rubin KH, Sternberg EM, Gold PW, Smith CC, Schulkin J (1997) Behavioral and neuroendocrine responses in shy children. Dev Psychobiol 30:127–140
Schmidt LA, Fox NA, Schulkin J, Gold PW (1999) Behavioral and psychophysiological correlates of self-presentation in temperamentally shy children. Dev Psychobiol 35:119–135
Snoek H, van Goozen SHM, Mathys W, Buitelaar JK, van Engeland H (2004) Stress responsivity in children with externalizing behavior disorders. Dev Psychopathol 16:389–406
Von Zerssen D (1986) Clinical self-rating scales (CSRS of the Munich psychiatric information system). In: Sartorius N, Ban TA (eds) Assessment of depression. Spinger-Verlag, Berlin pp 270–303
Wright JH, Bordon J (1991) Cognitive therapy of depression and anxiety. Psychiatr Ann 21:425–428
Zucker KJ, Bradley SJ (1995) Gender identity disorder and psychosexual problems in children and adolescents. Guilford Press, New York
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License ( https://creativecommons.org/licenses/by-nc/2.0 ), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Wallien, M.S., van Goozen, S.H. & Cohen-Kettenis, P.T. Physiological correlates of anxiety in children with gender identity disorder. Eur Child Adolesc Psychiatry 16, 309–315 (2007). https://doi.org/10.1007/s00787-007-0602-7
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00787-007-0602-7