
Abstract
Background
Some reports indicate that one of major causes of clinical failure after periacetabular osteotomy is development of secondary femoroacetabular impingement (FAI). To assess the impact of range of motion (ROM) on the increase in FAI following rotational acetabular osteotomy (RAO), we performed FAI simulations before and after RAO.
Methods
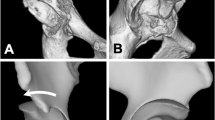
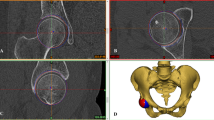
We evaluated 12 hips that had undergone RAO (study group), and 12 normal hips (control group). The study group was evaluated before and after surgery. Morphological parameters were evaluated to assess acetabular coverage. The acetabular anteversion angle, anterior CE angle, alpha angle, and combined anteversion angle were also measured. Impingement simulations were performed using 3D-CT. The ROM which causes bone-to-bone impingement was evaluated in flexion (flex), abduction, external rotation at 0° flexion, and internal rotation at 90° flexion. The lesions caused by impingement were evaluated.
Results
Radiographic measurements indicated improved postoperative acetabular coverage in the study group. The crossover sign was recognized pre- and postoperatively in every case in the study group and in no cases in the control group. In the simulation study, flexion, abduction, and internal rotation at 90° flexion decreased postoperatively. Impingement occurred within 45° internal rotation at 90° flexion in two preoperative and nine postoperative cases. The impingement lesions were anterosuperior of the acetabulum in all cases. There were correlations between anterior CE angle, CE angle, acetabular anteversion angle, and hip flexion angle. There were also correlations between the anterior CE angle, combined anteversion angle, and angle of internal rotation at 90° flexion.
Conclusions
In the postoperative simulation, there was a tendency to reduce the ROM in flexion, abduction, and internal rotation at 90° flexion due to impingement. Since there were more cases which caused impingement within 45° internal rotation at 90° flexion after RAO, we consider there is a potential for increased FAI after RAO.


Similar content being viewed by others

References
Ganz R, Klaue K, Vinh TS, Mast JW. A new periacetabular osteotomy for the treatment of hip dysplasia. Clin Orthop Relat Res. 1988;232:26–36.
Ninomiya S, Tagawa H. Rotational acetabular osteotomy for the dysplastic hip. J Bone Jt Surg Am. 1984;66:430–6.
Yasunaga Y, Yamasaki T, Ochi M. Patient selection criteria for periacetabular osteotomy or rotational acetabular osteotomy. Clin Orthop Relat Res. 2012;470:3342–54.
Steppacher SD, Tannast M, Ganz R, Siebenrock KA. Mean 20-year follow up of Bernese periacetabular osteotomy. Clin Orthop Relat Res. 2008;466:1633–44.
Ito H, Tanino H, Yamanaka Y, Minami A, Matsuno T. Intermediate to long-term results of periacetabular osteotomy in patients younger and older than 40 years of age. J Bone Jt Surg Am. 2011;93:1347–54.
Haddad FS, Garbuz DS, Duncan CP, Janzen DL, Munk PL. CT evaluation of periacetabular osteotomy. J Bone Jt Surg Br. 2000;82:526–31.
Suh DH, Lee DH, Jeong WK, Park SW, Kang CH, Lee SH. Virtual Bernese osteotomy using three-dimensional computed tomography in hip dysplasia. Arch Orthop Trauma Surg. 2012;132:447–54.
Myers SR, Eijer H, Ganz R. Anterior femoroacetabular impingement after periacetabular osteotomy. Clin Orthop Relat Res. 1999;363:93–9.
Siebenrock KA, Scholl E, Lottenback M, Ganz R. Bernese periacetabular osteotomy. Clin Orthop Relat Res. 1999;363:9–20.
Tönnis D. Normal values of the hip joint for the evaluation of X-rays in children and adults. Clin Orthop Relat Res. 1976;119:39–47.
Wiberg G. The anatomy and roentgenographic appearance of a normal hip joint. Acta Chir Scand. 1939;83(suppl 58):7–38.
Sharp IK. Acetabular dysplasia: the acetabular angle. J Bone Jt Surg Br. 1961;43:268–72.
Heyman CH, Herndon CH. Legg–Perthes disease. A method for the measurement of the roentgenographic result. J Bone Jt Surg Am. 1950;32:767–78.
Yasunaga Y, Yamasaki T, Matsuo T, Ishikawa M, Adachi N, Ochi M. Crossover sign after rotational acetabular osteotomy for dysplasia of the hip. J Orthop Sci. 2010;15:463–9.
Reynolds D, Lucas J, Klaue K. Retroverted of the acetabulum. J Bone Jt Surg Br. 1999;81:281–8.
Sakai T, Nishii T, Sugamoto K, Yoshikawa H, Sugano N. Is vertical-center-anterior angle equivalent to anterior coverage of the hip? Clin Orthop Relat Res. 2009;467:2865–71.
Sugano N, Noble PC, Kamaric E, Salama JK, Ochi T, Tullos HS. The morphology of the femur in developmental dysplasia of the hip. J Bone Jt Surg Br. 1998;80:711–9.
Nötzli HP, Wyss TF, Stoecklin CH, Schmid MR, Trieber K, Hodler J. The contour of the femoral head-neck junction as a predictor for the risk of anterior impingement. J Bone Jt Surg Br. 2002;84:556–60.
Nakahara I, Takao M, Sakai T, Nishii T, Yoshikawa H, Sugano N. Gender differences in 3D morphology and bone impingement of human hips. J Orthop Res. 2011;29:333–9.
Ziebarth K, Balakumar J, Domayer S, Kim YJ, Millis MB. Bernese periacetabular osteotomy in males: is there an increased risk of femoroacetabular impingement (FAI) after Bernese periacetabular osteotomy? Clin Orthop Relat Res. 2011;469:447–53.
Hasegawa Y, Masui T, Yamaguchi J, Kawabe K, Suzuki S. Factors leading to osteoarthritis after eccentric rotational acetabular osteotomy. Clin Orthop Relat Res. 2007;459:207–15.
Tannast M, Kubiak-Langer M, Langlotz F, Puls M, Murphy SB, Siebenrock KA. Noninvasive three-dimensional assessment of femoroacetabular impingement. J Orthop Res. 2007;25:122–31.
Kubiak-Langer M, Tannast M, Murphy SB, Siebenrock KA, Langolz F. Range of motion in anterior femoroacetabular impingement. Clin Orthop Relat Res. 2007;458:117–24.
Albers CE, Steppacher SD, Ganz R, Tannast M, Siebenrock KA. Impingement adversely affects 10-year survivorship after periacetabular osteotomy for DDH. Clin Orthop Relat Res. 2013;471:1602–14.
Nassif NA, Schoenecker PL, Thorsness R, Clohisy JC. Periacetabular osteotomy and combined femoral head-neck junction osteochondroplasty: a minimum two-year follow-up cohort study. J Bone Jt Surg Am. 2012;94:1959–66.
Ito H, Matsuno T, Hirayama T, Tanino H, Yamanaka Y, Minami A. Three-dimensional computed tomography analysis of non-osteoarthritic adult acetabular dysplasia. Skeltal Radiol. 2009;38:131–9.
Ahlberg A, Moussa M, Al-Nahadi M. On geographical variations in the normal range of joint motion. Clin Orthop Relat Res. 1988;234:229–31.
Roaas A, Andersson GB. Normal range of motion of the hip, knee and ankle joints in male subjects, 30–40 years of age. Acta Orthop Scand. 1982;53:205–8.
Siebenrock KA, Schöniger R, Ganz R. Anterior femoro-acetabular impingement due to acetabular retroversion: treatment with periacetabular osteotomy. J Bone Jt Surg Am. 2003;85:278–86.
Wettstein M, Dienst M. Hip arthroscopy for femoroacetabular impingement. Orthopade. 2006;35:85–93.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Iwai, S., Kabata, T., Maeda, T. et al. Three-dimensional kinetic simulation before and after rotational acetabular osteotomy. J Orthop Sci 19, 443–450 (2014). https://doi.org/10.1007/s00776-014-0547-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00776-014-0547-x