
Abstract
Hand, foot, and mouth disease (HFMD) is a common childhood illness that is caused by enteroviruses, and the prevalence of HFMD in China and around the world has resulted in a huge disease burden. Since 2010, the HFMD incidence has been the highest among infectious diseases in Suzhou, China. To investigate the epidemical, features, etiological characteristics, and clinical characteristics of HFMD in Suzhou City, East China, from 2011 to 2014. We retrospectively analyzed HFMD epidemiological data in Suzhou from 2011 to 2014. A total of 80,723 outpatients in the city of Suzhou were diagnosed with HFMD, including 1,846 severe cases. There were 2,387 (3.0 %) laboratory-confirmed cases, 807 of which exhibited severe symptoms. All analyses were stratified by age, disease severity, laboratory confirmation status, and enterovirus subtype. From 2011 to 2014, HFMD mainly affected children aged 1–3, and boys were more affected than girls. The highest peak incidences of HFMD occurred in May or June from 2011 to 2014, and lower peak incidences were observed from November to December and in districts with higher humidity. Enterovirus 71 and coxsackievirus A16 were the predominant viral genotypes in Suzhou in 2011 to 2012 and 2014, and the severe cases mainly correlated with EV71 subtypes. In 2013, other EVs were dominant. The proportion of patients with severe disease decreased significantly, and the VP1 capsid proteins of EV71 and CA16 from severe and mild cases were nearly identical. This study shows that it is time to start monitoring EVs in China and that we should accelerate vaccine research and develop public-health interventions for the control and prevention of HFMD, all of which will play an important role in the prevention of HFMD.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hand, foot, and mouth disease (HFMD) is a common, communicable disease of global concern that usually affects children under the age of five. Clinical symptoms are typically mild and self-limiting, but rarely, patients may also develop neurological complications, such as encephalomyelitis, aseptic meningitis, and acute flaccid paralysis, and die within a few days [1, 2]. HFMD is caused by a group of viruses belonging to the genus Enterovirus. Of these, enterovirus 71 (EV71) and coxsackievirus A16 (CA16) are the most common causative pathogens [3, 4], but several other human enteroviruses (EVs), including coxsackieviruses CA2, CA4-CA7, CA10, CA12, and CB1-CB5, can also cause the disease. Liu et al. [5] reported that the percentages of EV71, CA16, and other EVs isolated from HFMD survivors in Shanghai, Jiangsu, Hubei, Hunan, and Ningxia, China, were 43.44, 22.17, and 34.38 %, respectively; the percentages of EV71, CA16, and other EVs isolated from fatal HFMD cases were 90.22, 8.07, and 1.09 %, respectively, from 2008 to 2014.
In the past three decades, multiple, severe HFMD outbreaks have been documented throughout the world, especially in the Asia-Pacific region. HFMD has become a significant public health challenge throughout China since an EV71-caused HFMD outbreak in Fuyang, China, resulted in a large number of infected children. A total of 6,049 HFMD cases were reported, of which 3,023 (50 %) were hospitalized, 353 (6 %) were severe, and 22 (0.4 %) were fatal. Meanwhile, China immediately launched an emergency response strategy, including establishing a national HFMD supervision system in which HFMD was included in the notifiable class C infectious disease category and requiring that any HFMD case in China should be reported to the National Notifiable Disease Reporting System (NNDRS) [5–7]. Sporadic cases are reported directly to the NNDRS by a doctor. For an HFMD outbreak, Chinese Centers for Disease Control and Prevention (CDC) researchers will immediately arrange for patient segregation. According to the NNDRS, HFMD had the highest incidence among notifiable infectious diseases, and a total of 1,071,7283 HFMD cases including 3,046 fatalities and 490,923 laboratory-confirmed cases were reported to the NNDRS from 2008 to June 2014 in mainland China [5]. The sharp rise in the number of severe HFMD cases has adversely affected the health of children in China.
Suzhou borders Shanghai, and it covers an area of 8,488.42 square kilometers, of which the plains account for 55 % of the total area. The city has a thriving economy, a well-established transportation system, and a population of approximately 10.6 million. It also has a large burden of HFMD. From 2011 to 2014, a total of 80,723 probable cases of HFMD were diagnosed in Suzhou, 1,846 of which were severe. As a result, controlling the spread of HFMD has become an important public health issue in Suzhou. To eliminate HFMD, it is important to understand HFMD epidemiology, and genetic analyses are useful to document viral transmission pathways and to gather information that can aid in the control of HFMD. In this study, we investigated the epidemiological features and molecular epidemiology of HFMD in Suzhou from 2011 to 2014 to provide information to help guide the development of effective prevention and control measures in the city of Suzhou.
Materials and methods
Case definitions
According to the guidelines of the Prevention and Control of HFMD issued by the CDC (2009 Edition) (http://www.chinacdc.cn/jkzt/crb/szkb/jszl_2275/200906/t20090612_24707.htm), HFMD is categorized as follows: if a doctor diagnoses a patient as having a small rash on the hands, feet, mouth, or buttocks, with or without fever, the patient is defined as a suspected HFMD case. Patients appearing with any neurologic or cardiopulmonary complications are classified as severe HFMD cases, while the rest are classified as mild cases.
If a clinical specimen, including a throat swab or stool sample that was collected by medical workers, tested positive for EV71, CA16, or other EVs by real-time polymerase chain reaction (PCR) and virus isolation, the case was defined as HFMD.
Source of epidemiological data
All HFMD cases in China must be reported, and workers at the local hospitals must input the information into the NNDRS database within 24 h. Information is collected using a standardized form that includes basic demographic information (sex, date of birth, and address), case classification (probable or confirmed), severity (mild or severe), death status, date of symptom onset, date of diagnosis, date of death (if applicable), and virus type (EV71, CA16, or other EV) for confirmed cases.
Specimen collection
According to the HFMD Monitoring Technology Plan in Jiangsu province, in each district of Suzhou city, for mild cases, at least five specimens are collected per month, while all of the severe cases are sampled, including a throat swab or stool sample, which is transported to our laboratory using a cold chain (under 0 °C) within 24 h, and all of the samples are stored at −80 °C and tested within 1 month.
Detection of viral RNA from specimens
Viral RNA was extracted from 200 μl of clinical specimens using a QIAamp Viral RNA Mini Kit (QIAGEN, Hilden, Germany) according to the manufacturer’s instructions. The RNA from each sample was examined using a commercially available real-time PCR kit (Diagnostic Kit for Human Enterovirus, EV71, and CA16, Jiangsu Shuoshi Biological Technology Co., Ltd., Taizhou, China) according to the manufacturer’s protocols. Test results were classified into four categories: EV negative, EV71 positive, CA16 positive, or positive for another EV without further serotype identification.
Virus isolation
Specimens for virus isolation and culture were obtained from 332 samples that were positive by real-time PCR for CA16 or EV71 and whose cycle threshold (Ct) number (defined as the number of cycles for the fluorescence signal to cross the detection threshold) was less than 25. Human rhabdomyosarcoma (RD) cells (susceptible to EV71 and CA16) or human epithelial cell type 2 (Hep-2) cells (susceptible to other EVs) were grown for 7 days in Roswell Park Memorial Institute (RPMI)-1640 medium supplemented with HEPES (0.238 g per 100 ml), NaHCO3 (0.3 g per 100 ml), 8 % fetal bovine serum (Invitrogen, Carlsbad, CA, USA), and 0.30 U of streptomycin per ml. The cells were harvested when the cytopathic effect (CPE) was visible over at least 50–75 % of the cell layer. Sixty-five blind passages were performed for those cultures that did not exhibit CPE after 7 days. The medium from the infected cells was harvested using a pipette and stored immediately at −70 °C [8, 9].
Sequencing
The detection method was based on a one-step reverse transcription (RT)-PCR assay. The VP1 gene, which encodes the viral coat protein, of 31 of the EV71 and CA16 isolates, representing 18.8 % of the strains that were obtained from the virus cultures, was sequenced. The complete VP1 gene sequences from the 31 isolates were amplified by one-step RT-PCR. RT-PCR products were sent to Sangon Biotech Co., Ltd. (Shanghai, China) for DNA sequencing using an automated ABI 3730 DNA sequencer (Thermo Fisher Scientific, Waltham, MA, USA)[10]. The primers used for EV71-VP1 were as follows: forward, 5’-TATAATAGCACTAGCGGCAGC-3’; reverse, 5’-AGTAAGTCGCGAGAGCTGTCTTC-3’. The primers used for CA16-VP1 were as follows: forward, 5’-AGGTACTACACCCAGTGGTCAG-3’; reverse, 5’-GCAAGGTGCCGATTCACTACCCT-3’. The sequences obtained in this study have been deposited in the GenBank database under the accession numbers KT327132–KT327162.
Phylogenetic analysis
To construct a phylogenetic tree, different genotypes of EV71and CA16 reference strain sequences were obtained from the GenBank database at the National Center for Biotechnology Information. A total of 136 EV71 and CA16 sequences (including the 31 sequences generated in the present study), representing 75 regions throughout the world, were analyzed to determine the evolution of the viruses in the city of Suzhou. The sequences obtained in this study were screened using the online Basic Local Alignment Search Tool (BLAST) (http://blast.ncbi.nlm.nih.gov/Blast.cgi) to search for the most similar sequences. Multiple sequence alignments were performed using the ClustalW program. The robustness of the groupings was assessed using bootstrap resampling of 1,000 replicates, and phylogenetic trees were visualized with the MEGA 5.0 program.
Statistical analysis
All statistical analyses were performed using SPSS version 11.5 software (SPSS Inc., Chicago, IL, USA). Categorical variables were compared using the chi-squared test. All statistical tests were two-sided, and a difference with a P-value less than 0.05 was considered significant. Population statistics for Suzhou were obtained from the Suzhou Bureau of Public Security. Data on reported HFMD cases and deaths were obtained from the Suzhou CDC and the NNDRS of the Chinese CDC. Epidemiologic data were analyzed using Microsoft Excel.
Results
Epidemiological features
Demographic characteristics
A total of 80,723 HFMD cases in the city of Suzhou were reported to the NNDRS from January 2011 to December 2014, including 1,846 severe cases. Although there were more than 2,200 fatalities reported to the NNDRS from 2011 to 2014 in mainland China, there was no fatal cases in Suzhou. The average incidence rate of HFMD from 2011 to 2014 was 190.22 per 100,000. The incidence of HFMD was high in 2011, decreased in 2012–2013 (153.90 per 100,000), and emerged as a pandemic in 2014 (250.39 per 100,000). Among these cases, 49,065 were males and 31,719 were females, with an average male-to-female ratio of 1.54 (range: 1.49 to 1.62). The annual average incidence in males (231.71 per 100,000) was higher than that in females (149.78 per 100,000), and this difference was statistically significant (χ2= 3794.991, p < 0.0001). The majority of cases detected had mild to moderate symptoms (97.68 %, 78,853/80,723); the remaining cases (2.32 %) were classed as severe. The majority (65.76 %) of the cases occurred in children who did not attend school. The percentage of cases among children who attended a kindergarten or another school was 29.94 % and 5.71 %, respectively (Table 1).
Age and sex. The age of the 80,723 HFMD cases ranged from 1 month to 51 years. Although the whole-population incidence rate of HFMD was 190.22 per 100,000, the average incidence rate was 5,909.85 per 100,000 in the population aged ≤5 years, which accounted for 94.99 % (76,677) of the cases; 46,574 patients were boys and 30,103 were girls. Boys had a significantly higher incidence rate compared with that of girls (χ2=2647.11, P < 0.01). The highest peak incidence occurred in the 1- to 3-year-old group, accounting for 72.3 % of all HFMD cases (Table 1).
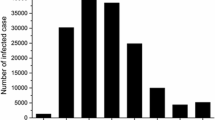
Seasonality. Although HFMD cases occurred throughout the year, the incidence rate of HFMD varied across each year and each month. Fluctuations in 2011 and 2012 were more obvious, with a large peak in May and June and a small peak in November and December. However, the large peak lasted from April to July, the small peak lasted from November to January in 2013, and the large and small peaks formed one continuous peak from April to December in 2014. Although there was a longer period of high incidence in 2013 and 2014, the proportion of severe cases was lower. From 2011 to 2014, there was a peak of severe cases in May of every year. In addition, there was a higher peak incidence of severe HFMD cases in August and September in 2011 and 2012 (Fig. 1).

HFMD cases and monthly distribution of severe cases in Suzhou city from 2011 to 2014
Location distribution. Clear differences in the annual HFMD incidence in different districts within the city of Suzhou were observed. From 2011 to 2013, the incidence in Suzhou as a whole decreased, except for the Wujiang and Taicang districts. However, in 2014, the HFMD incidence in all districts in Suzhou peaked. In 2011, the highest incidences were in Zhangjiagang and the Singapore industrial park, but from 2012 to 2014, the highest incidences were in Wujiang and Taicang, while the lowest incidence rate from 2011 to 2014 was in Kunshan (Fig. 2).

Annual HFMD incidence rates in the districts of Suzhou city from 2011 to 2014
Laboratory detection. Among the 80,723 reported HFMD cases, 2,387 (3.0 %) were laboratory-confirmed, including 807 severe cases and 1,580 mild cases. Among the 807 severe cases confirmed by laboratory tests, EV71, CA16, and other EVs accounted for 78.9, 8.6, and 12.5 %, respectively, of the cases. Among the 1,580 mild samples confirmed by laboratory tests, EV71, CA16, and other EVs accounted for 25.3, 35.3, and 39.4 %, respectively, of the cases. EV71 was the major agent in 2011 and 2012, while the other EVs were predominant in every month of 2013, and EV71 and CA16 were the predominant viral genotypes in 2014. The predominance of EV71 varied substantially by month, as it had a peak incidence from April to September of every year, while CA16 or other EVs had peak incidences from October to March of the following year (Fig. 3).

Etiological composition of laboratory-confirmed cases and severe rates in Suzhou city from 2011 to 2014
Phylogenetic analysis of the VP1 genes of EV71 and CA16
One hundred sixty-five strains were obtained from virus isolation experiments, 105 of which were EV71 strains and 60 of which were CA16 strains. Of the 165 strains, 20 % were taken as representatives for VP1 gene sequencing. Thirty-one complete VP1 gene sequences from 21 EV71 strains and 10 CA16 strains were amplified and sequenced, and their VP1 nucleotide sequences were 891 bp, encoding 297 amino acids. The VP1 nucleotide and amino acid sequence identities of the 21 EV71 strains ranged from 94.7 to 99.9 % and from 98.3 to 100.0 %, respectively. The VP1 nucleotide and amino acid sequence identities of the 10 CA16 isolates ranged from 96.4 to 99.9 % and from 99.3 to 99.7 %, respectively.
To characterize the EV71 strains circulating in Suzhou, we retrieved the sequences of EV71 genotypes and subtypes from GenBank, including representative sequences of the A, B1, B2, B3, B4, B5, C1, C2, C3, and C4 subtype strains. After comparison, all of the 21 EV71 strains isolated from Suzhou clustered exclusively in genotype C4, subtype C4a, and they were similar to EV71 sequences isolated from other provinces in mainland China. The phylogenetic tree shows that the EV71 strains of Suzhou formed three clusters. The strains isolated from 2011 to 2013 formed one cluster, and they have a close genetic relationship to 117-HZ- CHN-2011 (JX103503) strain that was isolated in Huizhou. The strains isolated in 2014 formed two clusters, which have a close genetic relationship to strains 265-GD-CHN-2009 (JF519702) (isolated in Guangdong) and MH704-SHH-CHN-2012 (JQ766172) (isolated in Shanghai), respectively (Fig. 4). Similarly, we retrieved the sequences of CA16 genotypes and subtypes from GenBank, including representative sequences of the A, B1a, B1b, and B2 subtype strains. After comparison, all 10 CA16 strains isolated from Suzhou clustered exclusively in genotype B1, subtype B1b, and they were similar to CA16 sequences isolated from other provinces in mainland China. The phylogenetic tree shows that the CA16 strains of Suzhou formed three clusters. The strains isolated in 2011 formed one cluster and had a close genetic relationship to the 21-TJ-CHN-2010 (JX455099) strain that was isolated in Tianjin. The strains isolated from 2012 to 2014 formed one cluster and had a close genetic relationship to the 213a-XM-CHN-2010 (JX127259) strain, and the two strains isolated in 2014 formed a cluster and had a close genetic relationship to the EV-1-SHX-CHN-2011 (JN582179) strain (Fig. 5).

Phylogenetic tree based on the complete VP1 sequences of Suzhou EV71 isolates and reference strains

Phylogenetic tree based on the complete VP1 sequences of Suzhou CVA16 isolates and reference strains
The phylogenetic dendrogram was constructed using the neighbor-joining method based on the 891-bp complete VP1 sequence of the 21 EV71 strains isolated in this study. Strains indicated by filled circles (●) and triangles (▲) are EV71 strains that were isolated from mild and severe cases, respectively.
The phylogenetic dendrogram was constructed using the neighbor-joining method based on the 891-bp complete VP1 sequence of the 10 CVA16 strains isolated in this study. Strains indicated by filled circles (●) and triangles (▲) are CVA16 strains that were isolated from mild and severe cases, respectively.
Discussion
This study reports the occurrence of HFMD in the city of Suzhou from 2011 to 2014; although there were 1,846 severe cases in Suzhou from 2011 to 2014, there were no fatal cases, perhaps because of a higher level of medical care, access to convenient transportation, and timely and effective treatment that resulted from the successful implementation of the policy of “early detection, early diagnosis, and early treatment”. Of the 80,723 cases, most were in children under the age of five (95.0 %) (Table 1), which is similar to previously reported domestic and foreign studies [11–14]. We found that the morbidity of HFMD in infants under the age of 1 was lower than that of children aged 1–5. It is possible that infants under the age of 1 have maternal antibodies against the virus and have less exposure to HFMD, thereby lessening their chance of infection [15, 16].
In the present study, children under the age of 3 accounted for 72.3 % of the total number of HFMD cases, and unschooled children accounted for 65.76 % of the total HFMD incidence, probably because of their low immunity resulting in poor self-protection and making it difficult to manage the health of such children [17, 18]. Boys acquired more HFMD infections than girls, perhaps because boys are more active and have poorer health habits, thereby increasing their chance of infection [19, 20].
HFMD epidemics have been shown to be significantly related to high temperatures in Japan and China [21–23]. Consistent with this, we found that there was a high peak incidence from May to July of 2011–2014 in Suzhou (Fig. 1). Suzhou has a subtropical monsoon marine climate, with four distinct seasons, and this period coincides with high temperatures. However, in 2013–2014, the incidence was maintained at a higher level throughout the entire year, and seasonal fluctuations, as were observed in 2011–2012, were not obvious. Whether this was related to high levels of air pollution is worth exploring. Because Suzhou has experienced more air particle pollution since 2013, this could lead viruses to adsorb to particulate matter, thereby enabling their long-term persistence. Further research is needed to investigate this question.
In addition to temperature, humidity has also been correlated with HFMD activity in Japan and in Shandong and Guangdong provinces of China [21–23]. The present study is agreement with these results. In the Suzhou area, Wujiang and Taicang, which are located next to Tai Lake and the Yangtze River, respectively, have higher relative humidities than Kunshan, which is farthest from the water. The highest incidences of HFMD occurred in Wujiang and Taicang from 2012 to 2014, while the lowest incidence rate from 2011 to 2014 occurred in Kunshan (Fig. 2).
According to a number of previously reported studies in China [24–27], EV71 infections led to an epidemic of severe cases, while CA16 infections led to the prevalence of mild cases. We found that when severe cases were prevalent, EV71 was isolated frequently, and when mild cases were prevalent, CA16 and other EV strains were isolated frequently. Compared with previous monitoring results, the proportion of other EV strains tended to increase yearly from 2011 to 2014. In 2013, other EVs were dominant, and the proportion of patients with severe disease significantly decreased. We have tested more than 300 specimens of EVs, more than 50 % of which were CA6. These results we will be discussed in a future article (data not shown) (Fig. 3).
EV71 molecular epidemiological studies based on the analysis of virus sequences began in 1995 [28]. Now, EV71 molecular epidemiology is mainly concerned with the VP1 gene, VP4 gene mutations, and the 5’ untranslated region. Of these, the VP1 gene has the greatest research value, and molecular epidemiological studies of CA16 are mainly concentrated on the capsid protein VP1. This is because (1) the VP1 protein is the major factor in terms of virus neutralization, as it directly determines viral antigenicity[29], and (2) the genetic diversity of the VP1 gene completely corresponds to the viral serotype; therefore, it not only can be used to classify different EV serotypes, but it can also be used to classify different small RNA viruses.
According to the evolutionary tree of the VP1 nucleotide sequence, EV71 is divided into three separate genetic types: A, B, and C. The A genotype is the prototype for the EV71 strain, and it contains only one strain, BrCr-USA-70; genotypes B and C can be further divided into five subtypes: B1, B2, B3, B4, and B5 and C1, C2, C3, C4, and C5, respectively, and the C4 can be divided into subtypes C4a and C4b [30]. Nucleotide sequence differences within the same genotype are less than 12 % [31]. Data show that the EV71 population in mainland China in the past 10 years is mainly divided into two classes. From 1998 to 2004, EV71 isolates from Guangdong and Shanghai belonged to the C4b subtype. After 2004, they were gradually replaced by the C4a subtype. During the past five years, subtype C4a has become the major EV71 epidemic strain in mainland China [32]. Since March 2008, most regions of China have had varying degrees of HFMD outbreaks, and the EV71 C4a subtype has been isolated repeatedly [4, 33]. This shows that after 2008 in mainland China, the C4a gene subtype may have become more widely distributed. The phylogenetic tree of the 21 EV71 strains that were isolated in this study showed that all of the EV71 strains in Suzhou in 2011–2014 were of the C4a subtype, and they might have originated from EV71 strains from Shanghai and Guangdong (Fig. 4).
In China, Li et al. [34] analyzed CA16 isolates in Shenzhen from 1999 to 2004. Based on the evolution of VP1, CA16 strains can be divided into A, B, and C genotypes, and nucleotide sequence differences between the B and C genotype range from 5.8 % to 11 %. In 2007, Perera et al. [35] analyzed 52 CA16 strains that were isolated over 10 years in five countries in the Asia-Pacific region. They divided CA16 strains into A and B genotypes, and genotype B was divided into the B1 and B2 subtypes. They demonstrated that the B and C genotypes reported by Li et al. are identical to their B1 and B2 subtypes.
In the city of Suzhou, which is located in the south of Jiangsu province, Shan et al. [36] found that two B1 branches, B1a and B1b, existed simultaneously and circulated in 2012, and they suggested that the B1b genotype has an evolutionary advantage. In the present study, we selected sequences of 47 CA16 strains from GenBank that represent strains that were isolated from different countries in different years, and compared them with the Suzhou isolates. Our results showed that the VP1 region of the 10 CA16 Suzhou strains had highly homologous nucleotide and amino acid sequences, all belonging to the B1b branch of the B1 subtype, which is consistent with a report in areas of Jiangsu province by Shan et al. (Fig. 5).
Based on the Suzhou HFMD monitoring results from 2011–2014, future work should focus on the prevention of HFMD infections. As the proportion of other EV strains tends to increase yearly, and the epidemiological information regarding the other EVs is limited, it is the time to start monitoring other EVs in China. Vaccination also remains the most significant and effective way to control disease. On December 4, 2015, China’s State Food and Drugs Administration approved the production of inactivated EV71 vaccines from human diploid cells. A phase III clinical trial of 12,000 subjects showed that an inactivated EV71 vaccine provided 97.3 % protection against HFMD and that there were no adverse reactions related to the vaccine. Once the use of this EV71 vaccine increases, it will reduce the number of severe HFMD cases and the incidence of HFMD caused by EV71. In view of the fact that other EVs, some of which were especially dominant in 2013, also account for a certain proportion of HFMD cases and can also cause severe HFMD, accelerating the development of vaccines against CA16 and other pathogens will play a an important role in the prevention of HFMD. In addition, we should popularize health education for young children and parents to promote good health-related behaviors, cut off the transmission source, and curb the spread of epidemics. These are economical and effective ways to reduce the risk of HFMD.
References
Liu CC, Tseng HW, Wang SM, Wang JR, Su IJ (2000) An outbreak of enterovirus 71 infection in Taiwan, 1998: epidemiologic and clinical manifestations. J Clin Virol 17:23–30
McMinn PC (2002) An overview of the evolution of enterovirus71 and its clinical and public health significance. FEMS Microbiol Rev 26:91–107
Xing Weijia, Liao Qiaohong, Viboud Cécile, Zhang Jing (2014) Epidemiological characteristics of hand-foot-and-mouth disease in China, 2008–2012. Lancet Infect Dis 14(4):308–318
Yong Z, Wen Bo X (2013) Molecular epidemiology of enteroviruses associated with hand, foot, and mouth disease in the mainland of china. Biomed Environ Sci 26(11):875–876
Liu S-L, Pan H, Liu P, Amer S, Chan T-C (2015) Comparative epidemiology and virology of fatal and nonfatal cases of hand, foot and mouth disease in mainland China from 2008 to 2014. Rev. Med. Virol. 25:115–128
Xu W, Liu CF, Yan L et a1 (2012) Distribution of enteroviruses is hospitalized ehidren with hand,foot and mouth disease and relationship between pathogens and nervous system complication. J Virol 9:1–9
Zhang Y, Zhu Z, Yang W, Ren J, Tan X, Wang Y et al (2010) An emerging recombinant human enterovirus 71 responsible for the 2008 outbreak of hand foot and mouth disease in Fuyang city of China. Virol J 7:94
Li Y, Zhu R, Qian Y et al (2011) Comparing Enterovirus 71 with CoxsackievirusA16 by analyzing nucleotide sequences and antigenicity of recombinant proteins of VP1s and VP4s. BMC Microbiology 11:246
Phuektes P, Hooi Chua B (2011) Sharon Sanders Mapping genetic determinants of the cell-culture growth phenotype of enterovirus 71. J General Virol 92:1380–1390
Linlin L, Yaqing H, Hong Y et al (2005) Genetic characteristics of human enterovirus 71 and coxsackievirus A16 circulating from 1999 to 2004 in Shenzhen, People’s Republic of China. J Clin Microbiol 43(8):3835–3839
Wang Y-C, Cheng H-B, Chen H-H (2010) Circulating viruses associated with severe complicated enterovirus infection in Taiwan: a multi-year analysis. Pediatry Infect Dis J. 29(4):334–339
Nguyen NTB, Pham HV, Hoang CQ, Nguyen et al (2014) Epidemiological and clinical characteristics of children who died from hand, foot and mouth disease in Vietnam, 2011. BMC Infect Dis 14:341
Di Biao, Zhang Ying, Xie Huaping et al (2014) Circulation of Coxsackievirus A6 in hand-foot-mouth disease in Guangzhou, 2010–2012. Virol J 11:157
Cabrerizo M, Tarragó D, Muñoz-Almagro C, Del Amo E, Domínguez-Gil M, Eiros JM (2014) Molecular epidemiology of enterovirus 71, coxsackievirus A16 and A6 associated with hand, foot and mouth disease in Spain. Clin Microbiol Infect 20(3):O150–O156
Xing W, Liao Q, Viboud C, Zhang J, Sun J, Wu JT (2014) Hand, foot, and mouth disease in China, 2008–12: an epidemiological study. Lancet Infect Dis. 14(4):308–318
Zeng M, Li YF, Wang XH, Lu GP, Shen HG, Yu H, Zhu QR (2012) Epidemiology of hand, foot, and mouth disease in children in Shanghai 2007–2010. Epidemiol Infect 140(6):1122–1130
Ni H, Yi B, Yin J, Fang T, He T, Du Y, Wang J, Zhang H, Xie L, Ding Y, Gu W, Zhang S, Han Y, Dong H, Su T, Xu G, Cao G (2012) Epidemiological and etiological characteristics of hand, foot, and mouth disease in Ningbo, China, 2008–2011. J Clin Virol 54(4):342–348
Wen-Hao W, Kuo T-C, Lin Y-T (2013) Molecular Epidemiology of enterovirus 71 infection in the central region of Taiwan from 2002 to 2012. Plos One. 8(12):e83711
Fan X, Jiang J, Liu Y, Huang X, Wang P, Liu L, Wang J, Chen W, Wu W, Xu B (2013) Detection of human enterovirus 71 and Coxsackievirus A16 in an outbreak of hand, foot, and mouth disease in Henan Province, China in 2009. Virus Genes 46(1):1–9
Qiaoyun F, Xiongfei J, Lihuan L, Angao X (2013) Epidemiology and etiological characteristics of hand, foot and mouth disease in Huizhou City between 2008 and 2011. Arch Virol 158(4):895–899
Onozuka D, Hashizume M (2011) The influence of temperature and humidity on the incidence of hand, foot, and mouth disease in Japan. Sci Total Environ. 1(410–411):119–125
Liu Y, Wang X, Pang C et al (2015) Spatio-temporal analysis of the relationship between climate and hand, foot, and mouth disease in Shandong province, China, 2008–2012. BMC Infect Dis. 24(15):146
Huang Y, Deng T, Yu S et al (2013) Effect of meteorological variables on the incidence of hand, foot, and mouth disease in children: a time-series analysis in Guangzhou, China. BMC Infect Dis 13:134
De Wu, Changwen Ke, Wei Li (2011) A large outbreak of hand, foot, and mouth disease caused by EV71 and CAV16 in Guangdong, China, 2009. Arch Virol 156:945–953
Chang S-C, Li W-C, Guang-Wu (2012) Genetic characterization of enterovirus 71 isolated from patients with severe disease by comparative analysis of complete Genomes Chen. J Med Virol 84:931–939
Wang X, Zhu C, Bao W, Zhao K, Niu J, Yu XF, Zhang W (2012) Characterization of full-length enterovirus 71 strainsfrom severe and mild disease patients in northeasternChina. PLoS One 7(3):e32405
Chen X, Tan X, Li J, Jin Y, Gong L, Hong M, Shi Y, Zhu S, Zhang B, Zhang S, Zhang Y, Mao N, Xu W (2013) Molecular epidemiology of coxsackievirus A16: Intratypeand prevalent intertype recombination identified. PLoS One 8(12):e82861
Brown BA, Pallansch MA (1995) Complete nucleotide sequence of enterovirus 71 is distinct from poliovirus. Virus Res. 39(2–3):195–205
Oberste MS, Maher K, Kilpat Rick DR et al (1999) Molecular evolution of the human enteroviruses: correlation of serotype with VP1 sequence and application to picornavirus classification. Virol 73:1941–1948
Shimizu H, Utama A, Onnimala N et al (2004) Molecular epidemiology of enterovirus 71 infection in the Western Pacific Region. Pediatr Int 46:231–235
Brown BA, Oberste MS, Alexander JP et al (1999) Molecular epidemiology and evolution of enterovirus 71 strains isolated from 1970 to 1998. Virol 73:9969–9975
Zhang Yong, Tan Xiao-Juan, Hai-Yan W et al (2009) An outbreak of hand, foot, and mouth disease associated with subgenotype C4 of human enterovirus 71 in Shandong. China. Clin Virol 44:262–267
Zhang Y, Wang D, Yah D et a1 (2010) Molecular Evidence of Persistent Epidemic and Evolution of Subgenotype B1 Coxsaekievirus A16—Associated Hand, Foot, and Mouth Disease in China.J Clin Microbi01 48:619–622
Li L, He Y, Yang H et al (2005) Genetic characteristics of human enterovirus 71 and coxsackievirus A16 circulating from 1999 to 2004 in Shenzhen, People′s Republic of China. J Clin Microbiol 439(3):3835–3839
Perera D, Yusof MA, Podin Y et al (2007) Molecular phylogeny of modern coxsackievirus A16. Arch Virol 152(6):1201–1208
Shan J, Ji H, Bao L et al (2014) Coxsackie virus type 16 genetic characteristic analysis of group A of Jiangsu province in 2012. Chin J Nanjing Med Univ 34(1):80–83
Acknowledgements
The authors thank the staff of all the districts of the Suzhou CDC for providing clinical specimens. This study was supported by financial grants from National Natural Science Foundation of China (Grant Number: 81402732), the National Natural Science Foundation of China (Grant Number: 81301479), the Natural Science Foundation of Shandong Province, China (Grant Number: ZR2013HQ008), the Jiangsu Prevention Medicine Foundation (Grant Numbers: YZ2012008 and Y2012071), and the Suzhou Applied Basic Research Program Foundation (Grant Number: SYS201262).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This study was funded by the National Natural Science Foundation of China (Grant Number: 81402732), the National Natural Science Foundation of China (Grant Number: 81301479), the Natural Science Foundation of Shandong Province, China (Grant Number: ZR2013HQ008), the Jiangsu Prevention Medicine Foundation (Grant Numbers: YZ2012008 and Y2012071), and the Suzhou Applied Basic Research Program Foundation (Grant Number: SYS201262). Author Yu Xia has received research grants from the Jiangsu Prevention Medicine Foundation (Grant Numbers: Y2012071)and the Suzhou Applied Basic Research Program Foundation (Grant Number: SYS201262). Author Hong Ji has received research grants from the National Natural Science Foundation of China (Grant Number: 81402732). Author Qiang Shen has received research grants from the Jiangsu Prevention Medicine Foundation (Grant Numbers: YZ2012008). Author Hong Liu has received research grants from the National Natural Science Foundation of China (Grant Number: 81301479) and the Natural Science Foundation of Shandong Province, China (Grant Number: ZR2013HQ008).
Conflict of interest
All the authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Xia, Y., Shan, J., Ji, H. et al. Study of the epidemiology and etiological characteristics of hand, foot, and mouth disease in Suzhou City, East China, 2011–2014. Arch Virol 161, 1933–1943 (2016). https://doi.org/10.1007/s00705-016-2878-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00705-016-2878-8