
Abstract
Background
Surgical treatment of lesions involving the ventral craniovertebral junction (CVJ) and the lower clivus, traditionally involved complex lateral or transoral approaches to the skull base. However, mid or upper clivus involvement requires more extensive lateral approaches. Recently, the endoscopic endonasal approach (EEA) has become the standard for upper CVJ lesions and medial clival, and a valuable alternative for those tumors extending in its upper third as well as laterally. However, the EEA is associated with an increased risk of post-operative CSF leakage and infection when the tumor is characterized by an intradural extension. Furthermore, whenever the tumor has significant lateral and/or inferior extension below the odontoid process, the chances for a complete resection decrease.
Method
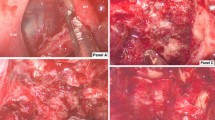
To analyze the extent of exposure of a hybrid microscopic-endoscopic transcondylar antero-lateral approach to the CVJ and clival region, and to verify its effectiveness in terms of mid and upper clival access. Five silicone-injected cadaver heads were used. Following a standard antero-lateral approach, condylectomy and jugular tubercle drilling were performed, after which angled endoscopes were utilized to extend the bone resection to the clivus. A volumetric assessment of the amount of clival removal was carried out. A case of CVJ chordoma operated through this approach is presented.
Results
The hybrid antero-lateral transcondylar approach provides adequate exposure of the ventral CVJ, up to the dorsum sellae and the sphenoid sinus, the contralateral petrous apex, and the contralateral paraclival internal carotid artery (ICA). Approximately 60% of the total clival volume can be removed with this approach. The main limitation is the limited visualization of the ipsilateral paraclival ICA and petrous apex.
Conclusion
The hybrid antero-lateral transcondylar approach is a valuable surgical option for CVJ tumor extending from C2 to the mid and upper clivus.







Similar content being viewed by others


References
al-Mefty O, Borba LA, Aoki N, Angtuaco E, Pait TG (1996) The transcondylar approach to extradural nonneoplastic lesions of the craniovertebral junction. J Neurosurg 84(1):1–6
Barges-Coll J, Fernandez-Miranda JC, Prevedello DM, Gardner P, Morera V, Madhok R, Carrau RL, Snyderman CH, Rhoton ALJ, Kassam AB (2010) Avoiding injury to the abducens nerve during expanded endonasal endoscopic surgery: anatomic and clinical case studies. Neurosurgery 67(1):144–154 discussion 154
Bejjani GK, Sekhar LN, Riedel CJ (2000) Occipitocervical fusion following the extreme lateral transcondylar approach. Surg Neurol 54(2):106–109
Bruneau M, Cornelius JF, George B (2006) Antero-lateral approach to the V3 segment of the vertebral artery. Oper Neurosurg 58(suppl_1):ONS-29
Bruneau M, George B (2008) The juxtacondylar approach to the jugular foramen. Neurosurgery 62(3 Suppl 1):71–75
Cavallo LM, Messina A, Cappabianca P, Esposito F, de Divitiis E, Gardner P, Tschabitscher M (2005) Endoscopic endonasal surgery of the midline skull base: anatomical study and clinical considerations. Neurosurg Focus 19(1):1–14
Choi D, Melcher R, Harms J, Crockard A (2010) Outcome of 132 operations in 97 patients with chordomas of the craniocervical junction and upper cervical spine. Neurosurgery 66(1):59–65 discussion 65
Cinalli G, Cappabianca P, de Falco R, Spennato P, Cianciulli E, Cavallo LM, Esposito F, Ruggiero C, Maggi G, de Divitiis E (2005) Current state and future development of intracranial neuroendoscopic surgery. Expert Rev Med Devices 2(3):351–373
Cohen MA, Evins AI, Lapadula G, Arko L, Stieg PE, Bernardo A (2017) The rectus capitis lateralis and the condylar triangle: important landmarks in posterior and lateral approaches to the jugular foramen. J Neurosurg 127(6):1398–1406
Dlouhy BJ, Dahdaleh NS, Menezes AH (2015) Evolution of transoral approaches, endoscopic endonasal approaches, and reduction strategies for treatment of craniovertebral junction pathology: a treatment algorithm update. Neurosurg Focus 38(4):E8
Doglietto F, Ferrari M, Mattavelli D et al (2018) Transnasal endoscopic and lateral approaches to the Clivus: a quantitative anatomic study. World Neurosurg 113:e659–e671
Fraser JF, Nyquist GG, Moore N, Anand VK, Schwartz TH (2010) Endoscopic endonasal transclival resection of chordomas: operative technique, clinical outcome, and review of the literature. J Neurosurg 112(5):1061–1069
Funaki T, Matsushima T, Peris-Celda M, Valentine RJ, Joo W, Rhoton ALJ (2013) Focal transnasal approach to the upper, middle, and lower clivus. Neurosurgery 73(2 Suppl operative):ons155–oons90 discussion ons190-1
George B, Lot G (1995) Anterolateral and posterolateral approaches to the foramen magnum: technical description and experience from 97 cases. Skull Base Surg 5(01):9–19
Hanakita S, Labidi M, Watanabe K, Froelich S (2018) A staged strategy for Craniocervical junction Chordoma with combination of endoscopic Endonasal approach and far lateral approach with endoscopic assistance: case report. J Neurol Surg B Skull Base 79(Suppl 4):S371–S377
Hopf NJ, Perneczky A (1998) Endoscopic neurosurgery and endoscope-assisted microneurosurgery for the treatment of intracranial cysts. Neurosurgery 43(6):1330–1337
Iaconetta G, Solari D, Villa A, Castaldo C, Gerardi RM, Califano G, Montagnani S, Cappabianca P (2018) The hypoglossal nerve: anatomical study of its entire course. World Neurosurg 109:e486–e492
Kasemsiri P, Carrau RL, Ditzel Filho LFS, Prevedello DM, Otto BA, Old M, de Lara D, Kassam AB (2014) Advantages and limitations of endoscopic endonasal approaches to the skull base. World Neurosurg 82(6 Suppl):S12–S21
Kassam AB, Gardner P, Snyderman C, Mintz A, Carrau R (2005) Expanded endonasal approach: fully endoscopic, completely transnasal approach to the middle third of the clivus, petrous bone, middle cranial fossa, and infratemporal fossa. Neurosurg Focus 19(1):E6
Kawashima M, Tanriover N, Rhoton ALJ, Ulm AJ, Matsushima T (2003) Comparison of the far lateral and extreme lateral variants of the atlanto-occipital transarticular approach to anterior extradural lesions of the craniovertebral junction. Neurosurgery 53(3):662–665
Labidi M, Watanabe K, Hanakita S, Park HH, Bouazza S, Bernat A-L, Froelich S (2018) The chopsticks technique for endoscopic endonasal surgery-improving surgical efficiency and reducing the surgical footprint. World Neurosurg 117:208–220
Lanzino G, Paolini S, Spetzler RF (2005) Far-lateral approach to the craniocervical junction. Neurosurgery 57(4 Suppl):367–371
Le C, Strong EB, Luu Q (2016) Management of Anterior Skull Base Cerebrospinal Fluid Leaks. J Neurol Surg B Skull Base 77(5):404–411
Matsushima T, Natori Y, Katsuta T, Ikezaki K, Fukui M, Rhoton AL (1998) Microsurgical anatomy for lateral approaches to the foramen magnum with special reference to transcondylar fossa (supracondylar transjugular tubercle) approach. Skull Base Surg 8(3):119–125
Mazur MD, Couldwell WT, Cutler A, Shah LM, Brodke DS, Bachus K, Dailey AT (2017) Occipitocervical instability after far-lateral transcondylar surgery: a biomechanical analysis. Neurosurgery 80(1):140–145
Mintelis A, Sameshima T, Bulsara KR, Gray L, Friedman AH, Fukushima T (2006) Jugular tubercle: morphometric analysis and surgical significance. J Neurosurg 105(5):753–757
Parlato C, Tessitore E, Schonauer C, Moraci A (2003) Management of benign craniovertebral junction tumors. Acta Neurochir 145(1):31–36
Perneczky A, Fries G (1998) Endoscope-assisted brain surgery: part 1--evolution, basic concept, and current technique. Neurosurgery 42(2):215–219
Perrini P, Benedetto N, Di Lorenzo N (2014) Transoral approach to extradural non-neoplastic lesions of the craniovertebral junction. Acta Neurochir 156(6):1231–1236
Sanan A, Abdel Aziz KM, Janjua RM, van Loveren HR, Keller JT (1999) Colored silicone injection for use in neurosurgical dissections: anatomic technical note. Neurosurgery 45(5):1264–1267
Sekhar LN, Ramanathan D (2012) Evolution of far lateral and extreme lateral approaches to the skull base. World Neurosurg 77(5–6):617–618
Sen CN, Sekhar LN (1990) An extreme lateral approach to intradural lesions of the cervical spine and foramen magnum. Neurosurgery 27(2):197–204
Shidoh S, Toda M, Kawase T, Nakajima H, Tomita T, Ogawa K, Yoshida K (2014) Transoral vs. endoscopic Endonasal approach for Clival/upper cervical Chordoma. Neurol Med Chir (Tokyo) 54(12):991–998
Shin H, Barrenechea IJ, Lesser J, Sen C, Perin NI (2006) Occipitocervical fusion after resection of craniovertebral junction tumors. J Neurosurg Spine 4(2):137–144
Shriver MF, Kshettry VR, Sindwani R, Woodard T, Benzel EC, Recinos PF (2016) Transoral and transnasal odontoidectomy complications: a systematic review and meta-analysis. Clin Neurol Neurosurg 148:121–129
Spektor S, Anderson GJ, McMenomey SO, Horgan MA, Kellogg JX, Delashaw JBJ (2000) Quantitative description of the far-lateral transcondylar transtubercular approach to the foramen magnum and clivus. J Neurosurg 92(5):824–831
Steinberger J, Skovrlj B, Lee NJ, Kothari P, Leven DM, Guzman JZ, Shin J, Shrivastava R, Caridi JM, Cho SK (2016) Surgical morbidity and mortality associated with transoral approach to the cervical spine. Spine (Phila Pa 1976) 41(9):E535–E540
Visocchi M, Signorelli F, Liao C, Rigante M, Paludetti G, Barbagallo G, Olivi A (2017) Endoscopic endonasal approach for craniovertebral junction pathologic conditions: myth and truth in clinical series and personal experience. World Neurosurg 101:122–129
Wen HT, Rhoton ALJ, Katsuta T, de Oliveira E (1997) Microsurgical anatomy of the transcondylar, supracondylar, and paracondylar extensions of the far-lateral approach. J Neurosurg 87(4):555–585
Acknowledgments
We thank Karl Storz SE & Co. (Tuttlingen, Germany) for kindly making their equipment available in order to allow us to complete our investigation. We thank Professor Beth De Felici for the English revision.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee (Hôpital Lariboisière, Assistance Publique – Hôpitaux de Paris, Université Paris – Diderot) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Additional information
Comments
This interesting paper deals with a modified anterolateral approach (novel hybrid antero-lateral transcondylar approach - HALT) to lesions involving cranio-vertebral junction (CVJ), upper and lateral aspect of the clivus. Traditionally, the surgical treatment of lesions involving the ventral CVJ comprises complex lateral or transoral approaches to the skull base. A standard antero-lateral approach, condylectomy and jugular tubercle drilling were performed, after which angled endoscopes were utilized to extend the bone resection to the clivus. The need of cadaver labs sometimes face with budget difficulty to fulfill the gold standard required by rich countries; nevertheless we all learned that it is possible to demonstrate its feasibility also in presence of limited resources (1). In my opinion the choice of an Extreme lateral approach should be better compared with the potententials of a standard submandibular retropharingeal aka Mc Afee approach, the latter providing a wide surgical domain as well. In the Authors ‘ statements, the identification of the lower clivus as the superior limit of transoral is purely orientative, since in special conditions, i.e. in childhood, it is possible to reach up to the superior third of the clivus by using a standard transoral approach (2). Finally to be underlined that the use of endoscope for CVJ surgery was first conceived for transmucosal surgeries (transnasal and transoral) as totally endoscopic approach and later on to extramucosal CVJ surgeries (i.e. anterolateral) as endocopic assisted procedures; such a definition, later on and more properly, became hybrid microscopic endoscopic surgery particulary intriguing for the significance of progression form its previous ancillary to the present leading actor surgical role (3).
Massimiliano VISOCCHI
Rome, Italy
REFERENCES
1) Signorelli F, Stumpo V, Della Pepa GM, La Rocca G, Oliva A, Olivi A, Visocchi M.(2019) Step-up Establishment of Neurosurgical Laboratory Starting with Limited Resources-Tips and Tricks. World Neurosurg. 126:83-89. doi: 10.1016/j.wneu.2019.02.034. Epub 2019 Feb 22. PMID: 30797916.
2) Visocchi M, Trevisi G, Iacopino DG, Tamburrini G, Caldarelli M, Barbagallo GM (2014) Odontoid process and clival regeneration with Chiari malformation worsening after transoral decompression: an unexpected and previously unreported cause of "accordion phenomenon". Eur Spine J. 4:S564-8
3) Visocchi M, Di Martino A, Maugeri R, González Valcárcel I, Grasso V, Paludetti G. (2015)Videoassisted anterior surgical approaches to the craniocervical junction: rationale and clinical results. Eur Spine J. 2713-23
This article is part of the Topical Collection on Neurosurgery general
Rights and permissions
About this article

Cite this article
Di Carlo, D.T., Voormolen, E.H., Passeri, T. et al. Hybrid antero-lateral transcondylar approach to the clivus: a laboratory investigation and case illustration. Acta Neurochir 162, 1259–1268 (2020). https://doi.org/10.1007/s00701-020-04343-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-020-04343-4