
Abstract
Background
Microvascular decompression (MVD) of hemifacial spasm (HFS) associated with the vertebral artery (VA) shows higher rates of incomplete cure and complications compared to non-VA-related HFS.
Method
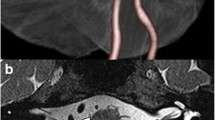
Purely endoscopic MVD for VA-associated HFS via a retrosigmoid keyhole was performed. Neurovascular conflicts by a directly offending artery and VA around the root exit zone of the facial nerve were clearly demonstrated under 30° endoscopic view without significant cerebellar retraction. The VA and directly offending artery were safely transposed with preservation of perforators under excellent view.
Conclusion
Endoscopic MVD offers reliable decompression for VA-associated HFS with minimal invasiveness.


Similar content being viewed by others


References
Hitotsumatsu T, Matsushima T, Inoue T (2003) Microvascular decompression for treatment of trigeminal neuralgia, hemifacial spasm, and glossopharyngeal neuralgia: three surgical approach variations: technical note. Neurosurgery 53:1436–1441 discussion 1442-1443
Komatsu F, Imai M, Hirayama A, Hotta K, Hayashi N, Oda S, Shimoda M, Matsumae M (2017) Endoscopic microvascular decompression with transposition for trigeminal neuralgia and hemifacial spasm: technical note. J Neurol Surg A Cent Eur Neurosurg 78:291–295
Masuoka J, Matsushima T, Nakahara Y, Inoue K, Yoshioka F, Kawashima M, Abe T (2017) Outcome of microvascular decompression for hemifacial spasm associated with the vertebral artery. Neurosurg Rev 40:267–273
Takemura Y, Inoue T, Morishita T, Rhoton AL Jr (2014) Comparison of microscopic and endoscopic approaches to the cerebellopontine angle. World Neurosurg 82:427–441
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The institutional ethics committee approved this study, and informed consent was obtained from patients.
Conflict of interest
None.
Electronic supplementary material
ESM 1
The 4-mm 0° endoscope is introduced, and the arachnoid membrane between CN VIII and CN IX is sharply incised. The 4-mm 30° endoscope is then introduced, and CN VII is visualized through the space between CN VIII and CN IX. The REZ of CN VII is seen to be compressed in tandem fashion directly by the PICA as an offending artery and indirectly by the VA. After the PICA and VA have been shifted caudally, the indentation on the REZ (white arrow) is visualized. The VA is safely lifted from the brainstem and transposed caudally using a few Teflon pledgets placed medially to the facial nerve. Transposition of the PICA is then applied. The PICA is fixed at the petrosal dura mater using Teflon felt string and fibrin glue. CN V, trigeminal nerve; CN VI, abducens nerve; CN XI, accessory nerve; XII, hypoglossal nerve. (WMV 68251 kb)
Rights and permissions
About this article

Cite this article
Komatsu, F., Imai, M. & Matsumae, M. How I do it: endoscopic microvascular decompression for hemifacial spasm associated with the vertebral artery. Acta Neurochir 160, 157–159 (2018). https://doi.org/10.1007/s00701-017-3392-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-017-3392-9