
Abstract
Background
Solitary non-chordomatous lesions of the clivus are rare pathologies, which represent a diagnostic challenge. This study provides an overview of the clinical, radiological and prognostic characteristics of non-chordomatous clival lesions, highlighting current therapeutic options.
Methods
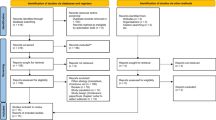
Twenty-two non-chordomatous lesions of the clivus were collected. A retrospective analysis of clinical and radiological patterns as well as survival data was conducted.
Results
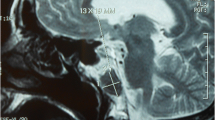
Clinical presentation was a result of local mass effect. Imaging features, although mainly specific, were not always diagnostic. Extent of surgery was gross total in 45.5 % of cases. Depending on the histology, biological behaviour and presence of seeding, adjuvant treatment was performed, tailoring the treatment strategy to the single patient.
Conclusions
Solitary non-chordomatous lesions of the clival bone are more prevalent than expected. They should be approached with a correct differential diagnosis, considering specific epidemiological, radiological, and histopathological characteristics, to minimise diagnostic bias and allow the planning of the best treatment strategy.




Similar content being viewed by others

References
Adada B, Al-Mefty O (2003) Fibrous dysplasia of the clivus. Neurosurgery 52:318–322, discussion 323
Al-Mefty O, Anand VK (1990) Zygomatic approach to skull-base lesions. J Neurosurg 73:668–673
Balasingam V, Anderson GJ, Gross ND, Cheng CM, Noguchi A, Dogan A, McMenomey SO, Delashaw JB Jr, Andersen PE (2006) Anatomical analysis of transoral surgical approaches to the clivus. J Neurosurg 105:301–308
Ballaux D, Verhelst J, Pickut B, De Deyn PP, Mahler C (1999) Ectopic macroprolactinoma mimicking a chordoma: a case report. Endocr Relat Cancer 6:117–122
Barnes L (1991) Pathobiology of selected tumors of the base of the skull. Skull Base Surg 1:207–216
Boari N, Roberti F, Biglioli F, Caputy AJ, Mortini P (2010) Quantification of clival and paraclival exposure in the Le Fort I transmaxillary transpterygoid approach: a microanatomical study. J Neurosurg 113:1011–1018
Buyuklu F, Tarhan E, Cakmak O, Ozgirgin N, Arikan U (2005) Isolated fibrous dysplasia of the sphenoid sinus. Rhinology 43:309–312
Castro JR, Linstadt DE, Bahary JP, Petti PL, Daftari I, Collier JM, Gutin PH, Gauger G, Phillips TL (1994) Experience in charged particle irradiation of tumors of the skull base: 1977–1992. Int J Radiat Oncol Biol Phys 29:647–655
Crocker M, Corns R, Bodi I, Zrinzo A, Gleeson M, Thomas N (2010) Chondromyxoid fibroma of the skull base invading the occipitocervical junction: report of a unique case and discussion. Skull Base 20:101
Eisig SB, Feghali J, Hall C, Goodrich JT (2000) The 2-piece Le Fort I osteotomy for cranial base access: an evaluation of 9 patients. J Oral Maxillofac Surg 58:482–486
Fisch U (1983) The infratemporal fossa approach for nasopharyngeal tumors. Laryngoscope 93:36–44
Fon G, Sage MR (1979) Osteochondroma of the clivus. Australas Radiol 23:46–53
Gagliardi F, Boari N, Mortini P (2011) Reconstruction techniques in skull base surgery. J Craniofac Surg 22:1015–1020
Gagliardi F, Boari N, Mortini P (2013) Solitary nonchordomatous lesions of the clival bone: differential diagnosis and current therapeutic strategies. Neurosurg Rev 36:513–522
Gagliardi F, Boari N, Riva P, Mortini P (2012) Current therapeutic options and novel molecular markers in skull base chordomas. Neurosurg Rev 35:1–13, discussion 13–14
Gagliardi F, Boari N, Roberti F, Gragnaniello C, Biglioli F, Caputy AJ, Mortini P (2012) Extradural subtemporal transzygomatic approach to the clival and paraclival region with endoscopic assist. J Craniofac Surg 23:1468–1475
Gagliardi F, Losa M, Boari N, Spina A, Reni M, Terreni MR, Mortini P (2013) Solitary clival plasmocytomas: misleading clinical and radiological features of a rare pathology with a specific biological behaviour. Acta Neurochir (Wien) 155:1849–1856
Kassam AB, Gardner P, Snyderman C, Mintz A, Carrau R (2005) Expanded endonasal approach: fully endoscopic, completely transnasal approach to the middle third of the clivus, petrous bone, middle cranial fossa, and infratemporal fossa. Neurosurg Focus 19:E6
Khanam H, Lipper MH, Wolff CL, Lopes MB (2001) Calvarial hemangiomas: report of two cases and review of the literature. Surg Neurol 55:63–67, discussion 67
Kim E (2010) Fibrous dysplasia of the clivus. J Korean Neurosurg Soc 48:441–444
Kondziolka D, Lunsford LD, Flickinger JC (1991) The role of radiosurgery in the management of chordoma and chondrosarcoma of the cranial base. Neurosurgery 29:38–45, discussion 45–36
Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, Burger PC, Jouvet A, Scheithauer BW, Kleihues P (2007) The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol 114:97–109
Machida K, Makita K, Nishikawa J, Ohtake T, Iio M (1986) Scintigraphic manifestation of fibrous dysplasia. Clin Nucl Med 11:426–429
Moravan MJ, Petraglia AL, Almast J, Yeaney GA, Miller MC, Edward Vates G (2012) Intraosseous hemangioma of the clivus: a case report and review of the literature. J Neurosurg Sci 56:255–259
Pallini R, Sabatino G, Doglietto F, Lauretti L, Fernandez E, Maira G (2009) Clivus metastases: report of seven patients and literature review. Acta Neurochir (Wien) 151:291–296, discussion 296
Rapidis AD, Archondakis G, Anteriotis D, Skouteris CA (1997) Chondrosarcomas of the skull base: review of the literature and report of two cases. J Craniomaxillofac Surg 25:322–327
Roberti F, Sekhar LN, Jones RV, Wright DC (2007) Intradural cranial chordoma: a rare presentation of an uncommon tumor. Surgical experience and review of the literature. J Neurosurg 106:270–274
Roche PH, Mercier P, Fournier HD (2007) Temporopolar epidural transcavernous transpetrous approach. Technique and indications. Neurochirurgie 53:23–31
Rosahl SK, Erpenbeck V, Vorkapic P, Samii M (2000) Solitary follicular thyroid carcinoma of the skull base and its differentiation from ectopic adenoma–review, use of galectin-3 and report of a new case. Clin Neurol Neurosurg 102:149–155
Sekhar LN, Javed T, Jannetta PJ (1993) Petroclival meningiomas. In: Sekhar LN, Janecka IP (eds) Surgery of cranial base tumors. Raven, New York, pp 605–659
Sekhar LN, Schramm VL Jr, Jones NF (1987) Subtemporal-preauricular infratemporal fossa approach to large lateral and posterior cranial base neoplasms. J Neurosurg 67:488–499
Sirvanci M, Karaman K, Onat L, Duran C, Ulusoy OL (2002) Monostotic fibrous dysplasia of the clivus: MRI and CT findings. Neuroradiology 44:847–850
Stapleton SR, Wilkins PR, Archer DJ, Uttley D (1993) Chondrosarcoma of the skull base: a series of eight cases. Neurosurgery 32:348–355, discussion 355–346
Tien RD (1992) Fat-suppression MR imaging in neuroradiology: techniques and clinical application. AJR Am J Roentgenol 158:369–379
Uttley D, Archer DJ, Marsh HT, Bell BA (1991) Improved access to lesions of the central skull base by mobilization of the zygoma: experience with 54 cases. Neurosurgery 28:99–103, discussion 103–104
Uttley D, Moore A, Archer DJ (1989) Surgical management of midline skull-base tumors: a new approach. J Neurosurg 71:705–710
Valentini V, Nicolai G, Lore B, Aboh IV (2008) Intraosseous hemangiomas. J Craniofac Surg 19:1459–1464
Vanhoenacker FM, De Praeter G, Kools D, Voormolen M, Parizel PM (2011) Unusual lesion of the clivus: diagnosis and discussion. Skelet Radiol 40:243–244, 223–244
Volpe NJ, Liebsch NJ, Munzenrider JE, Lessell S (1993) Neuro-ophthalmologic findings in chordoma and chondrosarcoma of the skull base. Am J Ophthalmol 115:97–104
Weber AL, Brown EW, Hug EB, Liebsch NJ (1995) Cartilaginous tumors and chordomas of the cranial base. Otolaryngol Clin N Am 28:453–471
Wei YT, Jiang S, Cen Y (2010) Fibrous dysplasia of skull. J Craniofac Surg 21:538–542
Williams WG, Lo LJ, Chen YR (1998) The Le Fort I-palatal split approach for skull base tumors: efficacy, complications, and outcome. Plast Reconstr Surg 102:2310–2319
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
Comment
This case series reminds us of the differential diagnosis of clival lesions; surprisingly, 30 % of patients in this series harboured non-chordomatous lesions. This further emphasises the need for at least tissue diagnosis on clival lesions (whether symptomatic or asymptomatic) because of the significant heterogeneity of lesions in this location with differences in the natural history, treatment, and outcome. However, when the radiological features are typical of clival ecchondrosis, a biopsy is not indicated.
Amir Dehdashti
NY, USA
Rights and permissions
About this article

Cite this article
Gagliardi, F., Spina, A., Boari, N. et al. Solitary lesions of the clivus: what else besides chordomas? An extensive clinical outlook on rare pathologies. Acta Neurochir 157, 597–605 (2015). https://doi.org/10.1007/s00701-014-2340-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-014-2340-1