
Abstract
Background
To present our intraoperative low-field magnetic resonance imaging (ioMRI) technique for stereotactic brain biopsy in various intracerebral lesions.
Method
Seventy-eight consecutive patients underwent stereotactic biopsies with the PoleStar N-20/N-30 ioMRI system and data were evaluated retrospectively. Biopsy technique included ioMRI before surgery, followed by insertion of the biopsy cannula in the lesion, and ioMRI before and after biopsy. Statistical analysis was performed to compare subgroups using Excel and SPSS statistic software.
Results
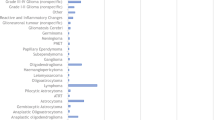
In all patients, stereotactic biopsy was possible, with a mean intraoperative surgery time of 86.2 ± 28.6 min and a mean hospital stay of 11.6 ± 4.6 days. In 97.4 % (n = 76), histology was conclusive, representing 58 brain tumors and 18 other pathologies. Five patients were biopsied previously without conclusive diagnosis, and all biopsies were conclusive this time. Mean cross-sectional lesion size in MRI T1 with contrast (n = 64) was 6.9 ± 5.7 cm2, and in lesions without T1 contrast enhancement (n = 14), T2 mean cross-sectional lesion size was 5.5 ± 3.9 cm2. Mean distance from the cortex surface to the lesion was 3.4 ± 1.2 cm. One patient suffered from a postoperative wound dehiscence; neither clinically or radiologically significant hemorrhage after surgery, nor intraoperative complications occurred.
Conclusions
Low-field ioMR-guided frameless stereotactic biopsy accurately diagnosed different intracerebral lesions without major complications for the patients, and within an acceptable surgery time and hospital stay. In repeated non-conclusive biopsies in particular, low-field ioMRI offers a technique for arriving at a diagnosis.


Similar content being viewed by others


References
Air EL, Warnick RE, McPherson CM (2012) Management strategies after nondiagnostic results with frameless stereotactic needle biopsy: Retrospective review of 28 patients. Surg Neurol Int 3:S315–319
Bernays RL, Kollias SS, Khan N, Brandner S, Meier S, Yonekawa Y (2002) Histological yield, complications, and technological considerations in 114 consecutive frameless stereotactic biopsy procedures aided by open intraoperative magnetic resonance imaging. J Neurosurg 97:354–362
Bernstein M, Al-Anazi AR, Kucharczyk W, Manninen P, Bronskill M, Henkelman M (2000) Brain tumor surgery with the Toronto open magnetic resonance imaging system: preliminary results for 36 patients and analysis of advantages, disadvantages, and future prospects. Neurosurgery 46:900–907, discussion 907–909
Czyz M, Tabakow P, Lechowicz-Glogowska B, Jarmundowicz W (2011) Prospective study on the efficacy of low-field intraoperative magnetic resonance imaging in neurosurgical operations. Neurol Neurochir Pol 45:226–234
Dammers R, Haitsma IK, Schouten JW, Kros JM, Avezaat CJ, Vincent AJ (2008) Safety and efficacy of frameless and frame-based intracranial biopsy techniques. Acta Neurochir (Wien) 150:23–29
Fahlbusch R, Ganslandt O, Nimsky C (2000) Intraoperative imaging with open magnetic resonance imaging and neuronavigation. Childs Nerv Syst 16:829–831
Gempt J, Buchmann N, Ryang YM, Krieg S, Kreutzer J, Meyer B, Ringel F (2012) Frameless image-guided stereotaxy with real-time visual feedback for brain biopsy. Acta Neurochir (Wien) 154:1663–1667
Hall WA (1998) The safety and efficacy of stereotactic biopsy for intracranial lesions. Cancer 82:1749–1755
Hall WA, Martin AJ, Liu H, Nussbaum ES, Maxwell RE, Truwit CL (1999) Brain biopsy using high-field strength interventional magnetic resonance imaging. Neurosurgery 44:807–813, discussion 813–804
Kanner AA, Vogelbaum MA, Mayberg MR, Weisenberger JP, Barnett GH (2002) Intracranial navigation by using low-field intraoperative magnetic resonance imaging: preliminary experience. J Neurosurg 97:1115–1124
Kollias SS, Bernays R, Marugg RA, Romanowski B, Yonekawa Y, Valavanis A (1998) Target definition and trajectory optimization for interactive MR-guided biopsies of brain tumors in an open configuration MRI system. J Magn Reson Imaging 8:143–159
Quinn J, Spiro D, Schulder M (2011) Stereotactic brain biopsy with a low-field intraoperative magnetic resonance imager. Neurosurgery 68:217–224, discussion 224
Schulder M, Catrambone J, Carmel PW (2005) Intraoperative magnetic resonance imaging at 0.12 T: is it enough? Neurosurg Clin N Am 16:143–154
Schulder M, Spiro D (2011) Intraoperative MRI for stereotactic biopsy. Acta Neurochir Suppl 109:81–87
Tronnier VM, Wirtz CR, Knauth M, Lenz G, Pastyr O, Bonsanto MM, Albert FK, Kuth R, Staubert A, Schlegel W, Sartor K, Kunze S (1997) Intraoperative diagnostic and interventional magnetic resonance imaging in neurosurgery. Neurosurgery 40:891–900, discussion 900–892
Tsermoulas G, Mukerji N, Borah AJ, Mitchell P, Ross N (2012) Factors affecting diagnostic yield in needle biopsy for brain lesions. Br J Neurosurg
van Velthoven V, Auer LM (1990) Practical application of intraoperative ultrasound imaging. Acta Neurochir (Wien) 105:5–13
Wen DY, Hall WA, Miller DA, Seljeskog EL, Maxwell RE (1993) Targeted brain biopsy: a comparison of freehand computed tomography-guided and stereotactic techniques. Neurosurgery 32:407–412, discussion 412–403
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Burkhardt, JK., Neidert, M.C., Woernle, C.M. et al. Intraoperative low-field MR-guided frameless stereotactic biopsy for intracerebral lesions. Acta Neurochir 155, 721–726 (2013). https://doi.org/10.1007/s00701-013-1639-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-013-1639-7