
Abstract
Purposes
The purpose of this study was to evaluate the hypothesis that the survival of patients undergoing R0 resection after triplet chemotherapy for resectable esophageal cancer with unfavorable prognostic factors (Category 3) would be similar to that of patients undergoing esophagectomy for esophageal cancer without such factors (Category 1).
Methods
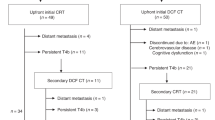
Patients with Category 3 tumors were assigned to receive triplet chemotherapy consisting of 5-fluorouracil, doxorubicin and nedaplatin (FAN) followed by radical esophagectomy. The outcomes of the bimodality treatment for Category 3 patients (n = 25) were compared with those of Category 1 patients (n = 41) in a prospective cohort study.
Results
Grade 3 or higher toxicity developed during chemotherapy in 32 % of the Category 3 patients, with no treatment-related deaths. No significant difference was detected in the surgery-related mortality and morbidity rates between the two groups. The recurrence-free survival was significantly worse in Category 3 than in Category 1 patients (p = 0.002), although the overall survival was not significantly different (p = 0.085) between the two groups in cases of R0 resection (5-year survival rates: 34.4 vs. 66.5 %).
Conclusions
Although FAN chemotherapy followed by radical esophagectomy can be safely performed, this treatment modality may not have sufficient power to cure Category 3 disease.






Similar content being viewed by others

References
Nishimaki T, Shimoji H, Sunagawa H. Recent changes and the future roles of esophageal cancer surgery. Ann Thorac Cardiovasc Surg. 2004;10:324–32.
Nishimaki T, Suzuki T, Suzuki S, Kuwabara S, Hatakeyama K. Outcomes of extended radical esophagectomy for thoracic esophageal cancer. J Am Coll Surg. 1998;186:306–12.
Nishimaki T, Suzuki T, Tanaka Y, Aizawa K, Hatakeyama K, Muto T. Intramural metastases from esophageal cancer: local indicators of advanced disease. World J Surg. 1996;20:32–7.
Okuyama T, Korenaga D, Edagawa A, Itoh S, Oki E, Kawanaka H, et al. Prognostic effects of oral anti-cancer drugs as adjuvant chemotherapy for 2 years after gastric cancer surgery. Surg Today. 2012;42:734–40.
Sjoquist KM, Burmeister BH, Smithers BM, Zalcberg JR, Simes RJ, Barbour A, et al. Survival after neoadjuvant chemotherapy or chemoradiotherapy for respectable oesophageal carcinoma: an updated meta-analysis. Lancet Oncol. 2011;12:681–92.
Ando N, Kato H, Igawa H, Shinoda M, Ozawa S, Shimizu H, et al. A randomized trial comparing postoperative adjuvant chemotherapy with cisplatin and 5-fluorouracil versus preoperative chemotherapy for localized advanced squamous cell carcinoma of the thoracic esophagus (JCOG9907). Ann Surg Oncol. 2012;19:68–74.
Sobin LH, Wittekind C. UICC: TNM classification of malignant tumors. 6th ed. New York: Wiley-Liss; 2002.
Nishimaki T, Tanaka O, Ando N, Ide H, Watanabe H, Shinoda M, et al. Evaluation of the accuracy of preoperative staging in thoracic esophageal cancer. Ann Thorac Surg. 1999;68:2059–64.
Kosugi S, Kanda T, Nakagawa S, Ohashi T, Nishimaki T, Hatakeyama K. Efficacy and toxicity of fluorouracil, doxorubicin, and cisplatin/nedaplatin treatment as neoadjuvant chemotherapy for advanced esophageal carcinoma. Scand J Gastroenterol. 2005;40:886–92.
Japan Esophageal Society. Japanese Classification of Esophageal Cancer. 10th ed. Tokyo: Kanehara & Co., Ltd; 2008.
Komukai S, Nishimaki T, Watanabe H, Ajioka Y, Suzuki T, Hatakeyama K. Significance of immunohistochemically demonstrated micrometastases to lymph nodes in esophageal cancer with histologically negative nodes. Surgery. 2000;127:40–6.
Nishimaki T, Tanaka O, Suzuki T, Aizawa K, Hatakeyama K, Muto T. Patterns of lymphatic spread in thoracic esophageal cancer. Cancer. 1994;74:4–11.
Kelsen DP, Ginsberg R, Pajak TF, Sheahan DG, Gunderson L, Mortimer J, et al. Chemotherapy followed by surgery compared with surgery alone for localized esophageal cancer. N Engl J Med. 1998;339:1979–84.
Miyata H, Yamasaki M, Kurokawa Y, Takiguchi S, Nakajima K, Fujiwara Y, et al. Clinical relevance of induction triplet chemotherapy for esophageal cancer invading adjacent organs. J Surg Oncol. 2012;106:441–7.
Rizk NP, Ishwaran H, Rice TW, Chen LQ, Schipper PH, Kesler KA, et al. Optimum lymphadenectomy for esophageal cancer. Ann Surg. 2010;251:46–50.
Morgan MA, Lewis WG, Casbard A, Roberts SA, Adams R, Clark GW, et al. Stage-for-stage comparison of definitive chemoradiotherapy, surgery alone and neoadjuvant chemotherapy for oesophageal carcinoma. Br J Surg. 2009;96:1300–7.
Peyre CG, Hagen JA, DeMeester SR, Van Lanschot JJ, Hölscher A, Law S, et al. Predicting systemic disease in patients with esophageal cancer after esophagectomy: a multinational study on the significance of the number of involved lymph nodes. Ann Surg. 2008;248:979–85.
Law S, Fok M, Chow S, Chu KM, Wong J. Preoperative chemotherapy versus surgical therapy alone for squamous cell carcinoma of the esophagus: a prospective randomized trial. J Thorac Cardiovasc Surg. 1997;114:210–7.
Ancona E, Ruol A, Santi S, Merigliano S, Sileni VC, Koussis H, et al. Only pathologic complete response to neoadjuvant chemotherapy improves significantly the long term survival of patients with resectable esophageal squamous cell carcinoma. Cancer. 2001;91:2165–74.
Bonner JA, Harari PM, Giralt J, Azarnia N, Shin DM, Cohen RB, et al. Radiotherapy plus cetuximab for squamous-cell carcinoma of the head and neck. N Engl J Med. 2006;354:567–78.
Conflict of interest
H. Shimoji and the co-authors have no conflicts of interest to declare in association with this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Shimoji, H., Kinjo, T., Karimata, H. et al. Clinical and oncological effects of triplet chemotherapy followed by radical esophagectomy for resectable esophageal cancer associated with unfavorable prognostic factors. Surg Today 44, 1273–1281 (2014). https://doi.org/10.1007/s00595-013-0700-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00595-013-0700-8