
Abstract
Aims
To identify metabolic phenotypes at increased risk of impaired glucose tolerance (IGT) in Italian overweight/obese children (n = 148, age 5–10 years) and adolescents (n = 531, age 10–17.9 year).
Methods
Phenotypes were defined as follows: obesity by the 95th cut-points of the Center for Disease Control body mass index reference standards, impaired fasting glucose (fasting plasma glucose ≥100 mg/dl), high circulating triglycerides (TG), TG/HDL cholesterol ≥2.2, waist-to-height ratio (WTHR) >0.6, and combination of the latter with high TG or TG/HDL cholesterol ≥2.2.
Results
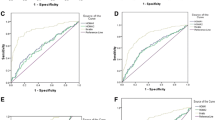
In the 148 obese children, TG/HDL-C ≥ 2.2 (OR 20.19; 95 % CI 2.50–163.28, p = 0.005) and the combination of TG/HDL-C ≥ 2.2 and WTHR > 0.60 (OR 14.97; 95 % CI 2.18–102.76, p = 0.006) were significantly associated with IGT. In the 531 adolescents, TG/HDL-C ≥ 2.2 (OR 1.991; 95 % CI 1.243–3.191, p = 0.004) and the combination with WTHR > 0.60 (OR 2.24; 95 % CI 1.29–3.87, p = 0.004) were associated with significantly increased risk of IGT. In the whole sample, having high TG levels according to the NIH National Heart, Lung and Blood Institute Expert Panel was not associated with an increased risk of presenting IGT.
Conclusions
TG/HDL-C ratio can be useful, particularly in children, to identify obese young patients at risk of IGT. Its accuracy as screening tool in a general population needs to be verified. The combination of TG/HDL-C ratio and WTHR > 0.6 did not improve prediction. Having high TG according to the NIH definition was not associated with increased risk of developing IGT.
Similar content being viewed by others


Abbreviations
- BMI:
-
Body mass index
- BP:
-
Blood pressure
- FBG:
-
Fasting blood glucose
- IFG:
-
Impaired fasting glucose
- IGT:
-
Impaired glucose tolerance
- HDL-C:
-
High-density lipoprotein cholesterol
- OGTT:
-
Oral glucose tolerance test
- T2D:
-
Type 2 diabetes
- TG/HDL-C:
-
Triglycerides-to-HDL cholesterol ratio
- WTHR:
-
Waist-to-height ratio
References
Misra A, Bhardwaj S (2014) Obesity and the metabolic syndrome in developing countries: focus on South Asians. Nestle Nutr Inst Workshop Ser 78:133–140
Savoye M, Caprio S, Dziura J et al (2014) Reversal of early abnormalities in glucose metabolism in obese youth: results of an intensive lifestyle randomized controlled trial. Diabetes Care 37(2):317–324
Tuomi T, Santoro N, Caprio S, Cai M, Weng J, Groop L (2014) The many faces of diabetes: a disease with increasing heterogeneity. Lancet 383(9922):1084–1094
Defronzo RA (2009) Banting Lecture. From the triumvirate to the ominous octet: a new paradigm for the treatment of type 2 diabetes mellitus. Diabetes 58(4):773–795
Shashaj B, Luciano R, Contoli B et al (2015) Reference ranges of HOMA-IR in normal-weight and obese young Caucasians. Acta Diabetol. doi:10.1007/s00592-015-0782-4
American Diabetes Association (2004) Screening for type 2 diabetes. Diabetes Care 27:S11–S14
Weiss R, Dziura J, Burgert TS et al (2004) Obesity and the metabolic syndrome in children and adolescents. N Engl J Med 350:2362–2374
Cambuli VM, Incani M, Pilia S et al (2009) Oral glucose tolerance test in Italian overweight/obese children and adolescents results in a very high prevalence of impaired fasting glycaemia, but not of diabetes. Diabetes Metab Res Rev 25:528–534
Conwell LS, Batch JA (2004) Oral glucose tolerance test in children and adolescents: positives and pitfalls. J Paediatr Child Health 40:620–626
Greig F (2012) Which obese youth are at increased risk for type 2 diabetes? Latent class analysis and comparison with diabetic youth. Pediatr Diabetes 13:181–188
Love-Osborne K, Butler N, Gao D, Zeitler P (2006) Elevated fasting triglycerides predict impaired glucose tolerance in adolescents at risk for type 2 diabetes. Pediatr Diabetes 7:205–210
Tsay J, Pomeranz C, Hassoun A et al (2010) Screening markers of impaired glucose tolerance in the obese pediatric population. Horm Res Paediatr 73:102–107
Morandi A, Maschio M, Marigliano M et al (2014) Screening for impaired glucose tolerance in obese children and adolescents: a validation and implementation study. Pediatr Obes 9(1):17–25
Janghorbani M, Almasi SZ, Amini M (2015) The product of triglycerides and glucose in comparison with fasting plasma glucose did not improve diabetes prediction. Acta Diabetol 52(4):781–788
Jeffery AN, Metcalf BS, Hosking J, Streeter AJ, Voss LD, Wilkin TJ (2012) Age before stage: insulin resistance rises before the onset of puberty: a 9-year longitudinal study (EarlyBird 26). Diabetes Care 35(3):536–541
Ong KK, Petry CJ, Emmett PM et al (2004) Insulin sensitivity and secretion in normal children related to size at birth, postnatal growth, and plasma insulin-like growth factor-I levels. Diabetologia 47(6):1064–1070
Manco M, Spreghini MR, Luciano R et al (2013) Insulin sensitivity from preschool to school age in patients with severe obesity. PLoS ONE 8(7):e68628
Valerio G, Maffeis C, Balsamo A et al (2013) Severe obesity and cardiometabolic risk in children: comparison from two international classification systems. PLoS ONE 8(12):e83793
National Heart, Lung, and Blood Institute (2011) Expert Panel on integrated guidelines for cardiovascular health and risk reduction in children and adolescents: summary report. Pediatrics 128(suppl 5):S237
Kuczmarski RJ, Ogden CL, Guo SS et al (2002) 2000 CDC growth charts for the United States: methods and development. Vital Health Stat 11(246):1–190
Khoury M, Manlhiot C, McCrindle B (2013) Role of the waist/height ratio in the cardiometabolic risk assessment of children classified by body mass index. J Am Coll Cardiol 62:742–751
Di Bonito P, Moio N, Scilla C et al (2012) Usefulness of the high triglyceride-to-HDL cholesterol ratio to identify cardiometabolic risk factors and preclinical signs of organ damage in outpatient children. Diabetes Care 35:158–162
Di Bonito P, Valerio G, Grugni G et al (2015) Comparison of non-HDL-cholesterol versus triglycerides-to-HDL-cholesterol ratio in relation to cardiometabolic risk factors and preclinical organ damage in overweight/obese children: the CARITALY study. Nutr Metab Cardiovasc Dis 25(5):489–494
Nolfe G, Spreghini MR, Sforza RW, Morino G, Manco M (2012) Beyond the morphology of the glucose curve following an oral glucose tolerance test in obese youth. Eur J Endocrinol 166(1):107–114
Dabelea D, Mayer-Davis EJ, Saydah S et al (2014) Prevalence of type 1 and type 2 diabetes among children and adolescents from 2001 to 2009. JAMA 311(17):1778–1786
Bonnefond A, Froguel P (2015) Rare and common genetic events in type 2 diabetes: What should biologists know? Cell Metab 21(3):357–368
Tanamas SK, Magliano DJ, Balkau B et al (2015) The performance of diabetes risk prediction models in new populations: the role of ethnicity of the development cohort. Acta Diabetol 52(1):91–101
Giannini C, Santoro N, Caprio S et al (2011) The triglyceride-to-HDL cholesterol ratio: association with insulin resistance in obese youths of different ethnic backgrounds. Diabetes Care 34(8):1869–1874
Maffeis C, Pinelli L, Brambilla P et al (2010) Fasting plasma glucose (FPG) and the risk of impaired glucose tolerance in obese children and adolescents. Obesity (Silver Spring) 18(7):1437–1442
O’Malley G, Santoro N, Northrup V et al (2010) High normal fasting glucose level in obese youth: a marker for insulin resistance and beta cell dysregulation. Diabetologia 53(6):1199–1209
Morrison KM, Xu L, Tarnopolsky M, Yusuf Z, Atkinson SA, Yusuf S (2012) Screening for dysglycemia in overweight youth presenting for weight management. Diabetes Care 35(4):711–716
Toledo-Corral CM, Alderete TL, Richey J, Sequeira P, Goran MI, Weigensberg MJ (2015) Fasting, post-OGTT challenge, and nocturnal free fatty acids in prediabetic versus normal glucose tolerant overweight and obese Latino adolescents. Acta Diabetol 52(2):277–284
Bailey DP, Savory LA, Denton SJ, Davies BR, Kerr CJ (2013) The hypertriglyceridemic waist, waist-to-height ratio, and cardiometabolic risk. J Pediatr 162(4):746–752
Lemieux I, Pascot A, Couillard C et al (2000) Hypertriglyceridemic waist: A marker of the atherogenic metabolic triad (hyperinsulinemia; hyperapolipoprotein B; small, dense LDL) in men? Circulation 102(2):179–184
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical standard
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Human and animal rights disclosure
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Informed consent
Informed consent was obtained from all patients for being included in the study.
Additional information
Managed by Massimo Porta.
On the behalf of the Childhood Obesity Group of the Italian Society of Paediatric Endocrinology and Diabetology. See study members referred in “Appendix” section.
Appendix
Appendix
Childhood Obesity Group of the Italian Society of Paediatric Endocrinology and Diabetology: Nicola Corciulo, MD, Ospedale S. Cuore di Gesù Gallipoli, Lecce; Maria Rosaria Licenziati, MD, Dipartimento di Pediatria, AORN Santobono-Pausilipon, Napoli. Anita Morandi, MD, Pediatria ad Indirizzo Diabetologico e Malattie del Metabolismo, Università di Verona, Verona; Beatrice Moro, MD, Ospedale Civile Piove di Sacco, Padova; Alessandro Sartorio, MD, Divisione di Auxologia, Istituto Auxologico Italiano, Piancavallo, Verbania; Rita Tanas, MD, Azienda Ospedaliero-Universitaria Arcispedale S. Anna, Ferrara.
Rights and permissions
About this article

Cite this article
Manco, M., Grugni, G., Di Pietro, M. et al. Triglycerides-to-HDL cholesterol ratio as screening tool for impaired glucose tolerance in obese children and adolescents. Acta Diabetol 53, 493–498 (2016). https://doi.org/10.1007/s00592-015-0824-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00592-015-0824-y