
Abstract
Objective
Cervical fractures with ankylosing spondylitis (CAS) are a specific type of spinal fracture with poor stability, low healing rate, and high disability rate. Its treatment is mainly surgical, predominantly through the anterior approach, posterior approach, and the anterior–posterior approach. Although many clinical studies have been conducted on various surgical approaches, controversy still exists concerning the choice of these surgical approaches by surgeons. The authors present here a systematic evaluation and meta-analysis exploring the utility of the anterior–posterior approach versus the anterior approach and the posterior approach.
Methods
After a comprehensive literature search of PubMed, Cochrane, Web of Science, and Embase databases, 12 clinical studies were included in the final qualitative analysis and 8 in the final quantitative analysis. Of these studies, 11 conducted a comparison between the anterior–posterior approach and the anterior approach and posterior approaches, while one examined only the anterior–posterior approach. Where appropriate, statistical advantage ratios and 95% confidence intervals were calculated.
Results
The present meta-analysis of postoperative neurological improvement showed no statistical difference in the overall neurological improvement rate between the anterior–posterior approach and anterior approach (OR 1.70, 95% CI 0.61 to 4.75; p = 0.31). However, the mean change in postoperative neurological function was lower in patients who received the anterior approach than in those who received the anterior–posterior approach (MD 0.17, 95% CI -0.02 to 0.36; p = 0.08). There was an identical trend between the anterior–posterior approach and posterior approach, with no statistically significant difference in the overall rate of neurological improvement (OR 1.37, 95% CI 0.70 to 2.56; p = 0.38). Nevertheless, the mean change in neurological function was smaller in patients receiving the anterior–posterior approach compared with the posterior approach, but there was no statistically significant difference between the two (MD 0.17, 95% CI -0.02 to 0.36; p = 0.08).
Conclusions
The results of this review and meta-analysis suggest that the benefits of the anterior–posterior approach are different from those of the anterior and posterior approaches in the treatment of ankylosing spondylitis-related cervical fractures. In a word, there is no significant difference between the cervical surgical approach and the neurological functional improvement. Therefore, surgeons should pay more attention to the type of cervical fracture, the displacement degree of cervical fracture, the spinal cord injury, the balance of cervical spine and other aspects to comprehensively consider the selection of appropriate surgical methods.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Ankylosing spondylitis (AS) combined with cervical spine fracture is a specific type of spinal trauma in AS patients. This chronic inflammatory disease is characterized by extensive ossification of bone, joint, and ligament tissues. The ankylosed spine increases local stress, and because AS patients often have a combination of osteoporosis and increased brittleness of the vertebral body, even small external forces can cause severe comminuted spinal transection fractures, also known as "carrot stick fractures". The yearly number of AS patients in the United States has been increasing [1], and found to be more common in men [2]. The incidence of spinal fractures in AS patients is up to five times higher than that in the normal population. AS complicated with cervical spine fractures is more common than other parts, often accompanied by cervical spinal cord injury, accounting for approximately 73% [3], followed by thoracic spine fractures [4]. The choice of the surgical method for AS patients with combined cervical medullary injury is strongly correlated with postoperative complications, length of stay, and in-hospital mortality [5]. Commonly used surgical procedures include the anterior, posterior, and anteroposterior approaches.
Most of them require strong internal fixation to counteract the locally concentrated stress and to maintain the stability of the fracture end. However, considerable controversy still exists on the requirements for preoperative traction repositioning, and on the choice of the optimal method: posterior, anterior, or combined anterior–posterior fixation [6,7,8,9]. Therefore, it is extremely important to analyze the available scientific evidence and summarize the existing findings on the optimal choice of an appropriate surgical procedure, which would serve clinical education and practical guidance.
Methods
The protocol and registration data are as follows: prospero.com; registered code: CRD42022315984.
The following inclusion criteria were applied: A retrospective clinical study of the surgical treatment of AS combined with cervical fractures.
The exclusion criteria implemented were as follows: (1) non-human experimental studies; (2) studies on non-surgical treatments; (3) studies that did not evaluate the combination of anterior and posterior approaches; (4) studies that did not assess clinical outcomes; and (5) case reports.
Literature search and selection
Literature from the PubMed, Embase, Web of Science, and Cochrane databases was systematically searched from 01/06/1990 to 03/31/2022.
The search strategy was based on a PubMed search with subject terms + free terms: ("Surgical Procedures, Operative" [Mesh] or Entry Terms) and ("Spondylitis, Ankylosing" [Mesh] or Entry Terms) as the search was conducted logically.
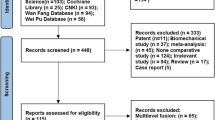
A total number of 162 published abstracts or manuscripts were identified. As can be seen in the PRISMA flow chart (Fig. 1), after applying the inclusion and exclusion criteria, a total number of 12 articles were included in the qualitative analysis and 8 articles in the quantitative analysis. Two independent researchers completed the selection and collation of the literature (Figs. 2, 3, 4 and 5).

PRISMA flow diagram of the study selection process

Risk-of-bias summary Green color indicates low risk, whereas yellow color denotes unknown risk


Impact of шгe surgical approach (anteroposterior vs anterior) on the rates of neurological improvement A, mean change in the postoperative neurological function B, complication rates C, rates of revise surgery D, and rates of dead in group E, rates of neurological deficits in upper cervical spine(C0-C4) and lower cervical spine(C5-C8) F. IV = inverse variance; M-H = Mantel–Haenszel test


Impact of the surgical approach (anteroposterior vs posterior) on the rates of neurological improvement A, mean change in the postoperative neurological function B,complication rates C,rates of revise surgery D,and rates of dead in the group E; rates of neurological deficits in upper cervical spine(C0-C4) and lower cervical spine(C5-C8) F. IV = inverse variance; M-H = Mantel–Haenszel test

The number of patients with ASIA grade A who use the combined approach is more than anterior or posterior approach. The number of patients with the ASIA grade is D or E accepting anterior or posterior approach is more than combined
Data analysis
We conducted data analysis using Review Manager, version 5.0 (Cochrane Collaboration). The Mantel–Haenszel test was adopted to calculate the dominance ratios and 95% confidence intervals, and forest plots were generated for each comparison. The overall effect of each method in the control and treatment groups was assessed using a fixed-effects model. Improvement in neurological function was selected as the primary outcome. The secondary outcome was the incidence of complications. The risk of bias was assessed using the Cochrane Risk of Bias tool to provide further insight into the conclusions drawn by the authors and our own subsequent meta-analysis.
Results
Study selection and characteristics
Of the initial 162 articles, 12 met the inclusion criteria and were clinically evaluated for neurological improvement. The quantitative analysis included eight studies, whose research information examined is summarized in Table 1. In 11 studies, the anterior–posterior approach was compared with either the anterior or posterior approach, whereas in one study, only the anterior–posterior approach was assessed. All studies measured the preoperative and postoperative neurological status, complications, revise surgery, and dead in Table 2.
Relations between approach and neurological outcome, complications, revise surgery and DEAD
The analysis showed that the anterior–posterior approach was the most common in our included studies, followed by the posterior and anterior approaches. Since the outcome data of each article was not compared under the same unified standard, the author did not conduct statistical analysis on the following data, we did not conduct statistical analysis on the following data.
Comparison between anterior-posterior approach and anterior approach
Our analysis of neurological outcomes and complication rates between the anterior–posterior approach and anterior approach revealed no significant difference in the overall neurological improvement rates, although the patients who received the anterior–posterior and anterior approach had higher neurological improvement rates (OR 1.70, 95% CI 0.61 to 4.75; p = 0.31). The mean change in the postoperative neurological status was improved in patients who underwent the anterior–posterior approach, but with no significant difference between the two groups (MD 0.14, 95% CI -0.23 to 0.51; p = 0.47). Similarly, no significant difference was found in the complication rates between the two approaches (OR 1.03, 95% CI 0.37 to 2.87; p = 0.96). Patients who underwent the anterior approach had a higher rate of secondary revision surgery than those in the anterior–posterior group, with a significant difference between the two groups (OR 0.37, 95% CI 0.14 to 0.99; p = 0.05); the mortality did not differ significantly between the two groups (OR 1.17, 95% CI 0.35 to 3.81; p = 0.79); no significant difference was found between the two groups between the neurological deterioration in the C0-C4 upper cervical spine (OR 0.50, 95%CI 0.04 to 7.10; p = 0.61) and the C5-C8 lower cervical spine (OR 0.80, 95%CI 0.53 to 1.21; p = 0.02).
Comparison of anterior-posterior versus posterior approach
Our analysis of neurological outcomes and complication rates between anterior–posterior versus posterior approaches showed trends similar to those of the anterior–posterior versus anterior approach comparison. Although the rate of the neurological improvement was higher in the patients who received the anterior–posterior approach (OR 1.37, 95% CI 0.70 to 2.56; p = 0.38), no significant difference was observed between their overall neurological improvement rates. An improvement in the mean change was established in the postoperative neurological status of patients who underwent anterior–posterior and posterior approaches, but there was no significant difference between the two (MD 0.17, 95% CI -0.02 to 0.36; p = 0.08). Similarly, no significant difference was detected in the rate of surgical complications between the anterior–posterior and posterior approaches (OR 1.39, 95% CI 0.70 to 2.78; p = 0.34); there was also no significant difference in the rate of revision surgery in patients who underwent anterior–posterior and posterior surgery and between the two groups for posterior surgery (OR 0.48, 95% CI 0.07 to 3.17; p = 0.45). Additionally, no significant difference was found between the two groups between the mortality in the two groups (OR 1.86, 95% CI 0.64 to 5.30; p = 0.26); no significant difference was found between the two groups between the neurological deterioration in the C0-C4 upper cervical spine (OR 0.36, 95% CI 0.03 to 4.21; p = 0.41) and the C5-C8 lower cervical spine (OR 0.95, 95%CI 0.27 to 3.30; p = 0.44).
Discussion
CAS is clinically characterized by progressive cartilage ossification combined with bone loss, resulting in a tubular spine that becomes stiff, fragile, and poorly resistant to stress and prone to fracture at low energy. Neck hyperextension is the most common mechanism of injury in CAS [22]. In the literature collected in this paper, there are also statistical data assessing the causes of injury. However, this paper did not analyze the causes of injury because different criteria for evaluating low-energy injuries and high-energy injuries are defined in the literature, hindering their comparison. Even though, it is easy to see that most of the literature still documents the etiology of low-energy injuries, indicating that low-energy trauma is a cause of fractures in patients with AS that cannot be ignored [23].
The incidence of cervical spine fractures in AS patients is three times higher than in the general population [24]. Despite the high incidence of fractures in patients with ankylosing spondylitis, delayed diagnosis is common. Chronic pain may mask patient's symptoms [24]. Simple DR films of the spine may not reveal fractures due to distorted anatomy, ligamentous ossification, and artifacts. On the other hand, early diagnosis and high suspicion of spinal cord injury may prevent possible long-term neurological damage. Therefore, due to the high susceptibility of patients with AS to spinal fractures and spinal cord injury even with only minor low-energy trauma, initial CT or MR imaging of the entire spine should be performed even if the patient is minimally symptomatic.
The change in neurological function was chosen as the main outcome indicator in this paper because it is an important indicator for evaluating the value of surgery. First, almost all the literature includes it as one of its outcome indicators for easy collection and statistics. Second, neurological function is also the purpose of our surgical treatment, and optimal neurological recovery can be achieved by an appropriate choice of surgical procedures to be applied. In the comparison presented in Table 1, we included the number of events, with no significant difference between the combined approach and the anterior and posterior approaches in terms of absolute values. We included inconsistent scales for the evaluation of neurological improvement in the literature (The B in The Fig 3 and 4), but two main scales owner applied: Frankel and ASIA grade scores. To enable the inclusion of a larger amount of data in this meta-analysis and to more objectively evaluate the outcome of the procedure, we employed the mean and variance values of the neurological improvement grade difference for comparison. However, during our statistical collection we found that better neurological recovery was obtained after the application of the combined approach than after that of the anterior and posterior approaches, but with no significant difference. This is also in line with the study of our current research, based on our analysis results and related literature show that the surgical approach is not directly related to the prognosis of patients [17]. Due to the particularity of the physical condition of patients with ankylosing spondylitis, the surgical methods should be individualized to avoid serious postoperative complications. Therefore, the indications of anterior, posterior and combined surgical approaches should depend on the nature of the injury, the mechanics at admission, the type of fracture, the degree of fracture displacement, the stability of fracture, the degree of nerve damage and so on. In the literature included here, the most appropriate procedure was performed, and some neurological recovery was achieved. Since the mechanics, severity and neurological outcome are quite different in the upper cervical spine (C0-C4) than lower (C5-C8) injuries, and the upper and lower cervical fractures are only partially divided in the included literature, this important detail is reflected in Table 1. In this article, there was no significant difference between the nerve damage of the upper and lower cervical injuries and the surgical approach. We are unable to collect more detailed conditions from the included literature, such as the type of fracture, spinal cord injury, fracture stability, fracture displacement and so on. However, the degree of postoperative neurological recovery is strongly correlated with the degree of cervical medullary injury damage, the presence or absence of diagnostic delay, and the adequacy of surgical decompression. Therefore, we recommend the implementation of stabilization surgery for CAS patients to achieve spinal balance and prevent further neurological impairment.
Metz-Stavenhagen et al. [25] recommended a combined anterior–posterior surgery approach in cases of severe combined posterior convexity, even though a higher complication rate exists after the use of this procedure. Michael et al. [26] found respiratory infections and urinary tract infections to be the least common complications in patients with CAS. In the present study, we also clearly established a higher complication rate in the combined approach, but with no statistically significant difference from those in the posterior and anterior approaches.
The reoperation rate is one of the indicators we utilized to evaluate the choice of the appropriate procedure. In this meta-analysis, we found a significant difference in the reoperation rate between the anterior and the combined approaches (p = 0.05), but not between the posterior and the combined approaches.
No significant difference was observed in mortality between the combined approach and the anterior and posterior approaches. Thus, we concluded that limited association existed between mortality in CAS patients and the procedure. Our statistical analysis showed that concurrent pulmonary infections and thrombosis were important causes of death in patients with CAS. Providing patients with strong immobilization and early lowering to the floor can effectively prevent such complications and reduce mortality.
Anterior fixation alone is the weakest and prone to complications method, leading to complications such as screw loosening and titanium plate displacement. Conversely, anterior surgery has the advantages of less trauma, complete decompression, and higher fusion rate, and is suitable for patients with good bone quality, less severe posterior column displacement and not accompanied by severe retroconvex deformity. Many reports of successful outcomes have been previously published. For example, Kouyoumdjian et al. [15] concluded that the anterior application of lengthened internal fixation plates can effectively counteract abnormalities. However, if the fracture is not completely repositioned by the anterior approach, it is in an unstable state due to the displacement of the posterior fracture end, and the increased anterior stress can easily cause internal fixation failure. Hence, the combined approach is more effective.
The posterior approach alone is stronger than the anterior, with adequate exposure and exact repositioning, and is suitable for most CAS patients, especially when the application of the anterior approach is difficult due to the presence of a posterior convexity deformity in the cervical spine. Its shortcomings are limited stability and the need for sufficiently long fixed segments to extend the surgical range [27]. It is also not suitable for CAS patients with fractures in the anterior column. Liu et al. [16] established no statistical difference in the degree of neurological recovery between the posterior-only approach and the combined approach, but the former had the advantages of shorter operative time, less surgical bleeding, and fewer surgery-related complications, and therefore the posterior-only approach is more favorable. In this article, there was no statistically significant difference between the combined anterior–posterior and posterior approaches. However, evidence suggests that patients with combined severe kyphosis are not suitable for simple posterior surgery because (1) it requires extensive dissection of the neck muscles, increases the risk of wound infection, and does not relieve the anterior spinal cord compression; (2) it is not suitable for patients with bone defects in the anterior column [28]; and (3) the stiffness of the posterior component and the vertebral body osteophytes, which may hinder the determination of the anatomical location of the instrument insertion point. As a result, it may lead to pedicle fractures, screw misalignment, nerve defects, and vertebral artery injury. Okten et al. [10] documented intraoperative complications of nerve root damage and vertebral artery injury due to improper screw placement in three patients with posterior approaches.
The combined anterior–posterior approach provides the best firmness compared to that achieved by the anterior and posterior approaches. We consider that the combined anterior–posterior approach may be the best option for treating cervical fractures in patients with AS. The use of this approach facilitates the achievement of the balance of the cervical spine, strong fixation of the anterior, middle, and posterior columns, and adequate and rapid nerve decompression. In addition, this combined approach can overcome the disadvantages of anterior surgery and posterior surgery alone. The rate of early three-column fusion increases after strict stabilization of the cervical fracture; and the incidence of loosening, dislodgement, fracture, and sinking of the implanted instrumentation is also lower. Due to firm fixation, patients are able to maintain better strength of their cervical motion and are able to get out of bed earlier, which helps to reduce complications, such as hemorrhagic pneumonia, deep vein thrombosis and decubitus ulcers. Payer et al. [29] reported in their study the treatment of four CAS cases with the combined approach. After a mean follow-up of 11 months, all patients showed good alignment with no deformities. Einsiedel et al. [12] suggested a combined approach with an anterior approach followed by a posterior approach in the first stage of surgery, whereas Ji et al. [30] supported that a sequential approach followed by an anterior approach was more appropriate. Olerud et al. [11] concluded that although a combined approach is associated with more surgical bleeding, more trauma, and longer operative time, a combined anterior and posterior approach is still recommended. However, due to the long operative time and high bleeding volume, it is not suitable for CAS patients with a poor physical condition.
Conclusion
Overall, this article highlights the results of the analysis of the combined anterior–posterior approach compared to the anterior and posterior approaches alone in the treatment of patients with CAS. The rate of revision surgery was higher in the anterior approach, but with no statistically significant differences in other aspects of outcome indicators. We conclude that for severe posterior convex deformities and loss the balance of the cervical spine if physical conditions permitting, a combined anterior–posterior approach is a relatively effective option for patients with CAS to ensure stability of the fracture end and to reduce the number of second-stage surgeries to improve patient acceptance. In a word, there is no significant difference between the neurological functional improvement and cervical surgical approach selected by the surgeons after considering the patient's condition. Therefore, surgeons should pay more attention to the type of cervical fracture, the displacement degree of cervical fracture, the spinal cord injury, the balance of cervical spine and other aspects to comprehensively consider the selection of appropriate surgical methods.
References
Walsh J, Hunter T, Schroeder K, Sandoval D, Bolce R (2019) Trends in diagnostic prevalence and treatment patterns of male and female ankylosing spondylitis patients in the United States, 2006–2016. BMC Rheumatol 3:39. https://doi.org/10.1186/s41927-019-0086-3
Longo UG, Loppini M, Petrillo S, Berton A, Maffulli N, Denaro V (2015) Management of cervical fractures in ankylosing spondylitis: anterior, posterior or combined approach? Br Med Bull 115:57–66. https://doi.org/10.1093/bmb/ldv010
Zeng QY, Chen R, Darmawan J, Xiao ZY, Chen SB, Wigley R, Le Chen S, Zhang NZ (2008) Rheumatic diseases in China. Arthritis Res Ther 10:R17. https://doi.org/10.1186/ar2368
Hartmann S, Tschugg A, Wipplinger C, Thome C (2017) Analysis of the literature on cervical spine fractures in ankylosing spinal disorders. Global Spine J 7:469–481. https://doi.org/10.1177/2192568217700108
Jacobs WB, Fehlings MG (2008) Ankylosing spondylitis and spinal cord injury: origin, incidence, management, and avoidance. Neurosurg Focus 24:E12. https://doi.org/10.3171/FOC/2008/24/1/E12
Lazennec JY, d’Astorg H, Rousseau MA (2015) Cervical spine surgery in ankylosing spondylitis: Review and current concept. Orthop Traumatol Surg Res 101:507–513. https://doi.org/10.1016/j.otsr.2015.02.005
Chon H, Park JH (2017) Cervical vertebral body fracture with ankylosing spondylitis treated with cervical pedicle screw: a fracture body overlapping reduction technique. J Clin Neurosci 41:150–153. https://doi.org/10.1016/j.jocn.2017.04.012
Yan L, Luo Z, He B, Liu J, Hao D (2017) Posterior pedicle screw fixation to treat lower cervical fractures associated with ankylosing spondylitis: a retrospective study of 35 cases. BMC Musculoskelet Disord 18:81. https://doi.org/10.1186/s12891-017-1396-5
Yang B, Lu T, Li H (2017) Single-session combined anterior-posterior approach for treatment of ankylosing spondylitis with obvious displaced lower cervical spine fractures and dislocations. Biomed Res Int 2017:9205834. https://doi.org/10.1155/2017/9205834
Okten AI, Arslan A, Olguner SK, Acik V, Istemen I, Arslan B, Gezercan Y (2021) Surgical outcomes of subaxial cervical fractures in patients with ankylosing spinal disorder. Turk Neurosurg 31:510–518. https://doi.org/10.5137/1019-5149.JTN.31174-20.2
Olerud C, Frost A, Bring J (1996) Spinal fractures in patients with ankylosing spondylitis. Eur Spine J 5:51–55
Einsiedel T, Schmelz A, Arand M, Wilke H-J, Gebhard F, Hartwig E, Kramer M, Neugebauer R, Kinzl L, Schultheiss M (2006) Injuries of the cervical spine in patients with ankylosing spondylitis: experience at two trauma centers. J Neurosurg Spine 5:33–45
An SB, Kim KN, Chin DK, Kim KS, Cho YE, Kuh SU (2014) Surgical outcomes after traumatic vertebral fractures in patients with ankylosing spondylitis. J Korean Neurosurg Soc 56:108–113. https://doi.org/10.3340/jkns.2014.56.2.108
Badve SA, Bhojraj SY, Nene AM, Varma R, Mohite S, Kalkotwar S, Gupta A (2010) Spinal instability in ankylosing spondylitis. Indian J Orthop 44:270–276. https://doi.org/10.4103/0019-5413.65151
Kouyoumdjian P, Guerin P, Schaelderle C, Asencio G, Gille O (2012) Fracture of the lower cervical spine in patients with ankylosing spondylitis: retrospective study of 19 cases. Orthop Traumatol Surg Res 98:543–551. https://doi.org/10.1016/j.otsr.2012.03.011
Liu B, Ji H, Zhang Z, Guo Y, Lv Y, Yang Z, Hou G, Zhou F, Tian Y (2021) Surgical treatment for cervical spine fracture in patients with ankylosing spondylitis: single posterior approach or combined anterior-posterior approach? Clin Spine Surg 34:E308–E314. https://doi.org/10.1097/BSD.0000000000001155
Luksanapruksa P, Millhouse PW, Carlson V, Ariyawatkul T, Heller J, Kepler CK (2019) Comparison of surgical outcomes of the posterior and combined approaches for repair of cervical fractures in ankylosing spondylitis. Asian Spine J 13:432–440. https://doi.org/10.31616/asj.2018.0197
Guo Q, Cui Y, Wang L, Lu X, Ni B (2016) Single anterior approach for cervical spine fractures at C5–T1 complicating ankylosing spondylitis. Clin Neurol Neurosurg 147:1–5. https://doi.org/10.1016/j.clineuro.2016.05.015
He A, Xie D, Cai X, Qu B, Kong Q, Xu C, Yang L, Chen X, Jia L (2017) One-stage surgical treatment of cervical spine fracture-dislocation in patients with ankylosing spondylitis via the combined anterior-posterior approach. Medicine (Baltimore) 96:e7432. https://doi.org/10.1097/MD.0000000000007432
Sapkas G, Kateros K, Papadakis SA, Galanakos S, Brilakis E, Machairas G, Katonis P (2009) Surgical outcome after spinal fractures in patients with ankylosing spondylitis. BMC Musculoskelet Disord 10:96. https://doi.org/10.1186/1471-2474-10-96
Yang H, Wang H, Zhang B, Sun Y, Wang L, Lu X (2021) Cervical spine fracture-dislocation in patients with ankylosing spondylitis and severe thoracic kyphosis: application of halo vest before and during surgical management. Clin Neurol Neurosurg 207:106744. https://doi.org/10.1016/j.clineuro.2021.106744
Tico N, Ramon S, Garcia-Ortun F, Ramirez L, Castello T, Garcia-Fernandez L, Lience E (1998) Traumatic spinal cord injury complicating ankylosing spondylitis. Spinal Cord 36:349–352. https://doi.org/10.1038/sj.sc.3100619
Lee CK, Yoon DH, Kim KN, Yi S, Shin DA, Kim B, Lee N, Ha Y (2016) Characteristics of cervical spine trauma in patients with ankylosing spondylitis and ossification of the posterior longitudinal ligament. World Neurosurg 96:202–208. https://doi.org/10.1016/j.wneu.2016.08.110
Detwiler KN, Loftus CM, Godersky JC, Menezes AH (1990) Management of cervical spine injuries in patients with ankylosing spondylitis. J Neurosurg 72:210–215. https://doi.org/10.3171/jns.1990.72.2.0210
Metz-Stavenhagen P, Krebs S, Meier O (2001) Cervical fractures in ankylosing spondylitis. Orthopade 30:925–931. https://doi.org/10.1007/s001320170005
Mathews M, Bolesta MJ (2013) Treatment of spinal fractures in ankylosing spondylitis. Orthopedics 36:e1203-1208. https://doi.org/10.3928/01477447-20130821-25
Serin E, Karakurt L, Yilmaz E, Belhan O, Varol T (2004) Effects of two-levels, four-levels, and four-levels plus offset-hook posterior fixation techniques on protecting the surgical correction of unstable thoracolumbar vertebral fractures: a clinical study. Eur J Orthop Surg Traumatol 14:1–6
Taggard DA, Traynelis VC (2000) Management of cervical spinal fractures in ankylosing spondylitis with posterior fixation. Spine (Phila Pa 1976) 25:2035–2039. https://doi.org/10.1097/00007632-200008150-00006
Payer M (2006) Surgical management of cervical fractures in ankylosing spondylitis using a combined posterior-anterior approach. J Clin Neurosci 13:73–77. https://doi.org/10.1016/j.jocn.2005.02.010
Ji Hong-quan ZF, TlAN Yun LIU, Zhong-jun, (2013) Operation choices for cervical spinal fracture in patients with ankylosing spondylitis. Chin J Trauma 29:297–301. https://doi.org/10.3760/cma.j.issn.1001-8050.2013.4.003
Author information
Authors and Affiliations
Contributions
CHJ and HFL were responsible for the conception and design; CHJ and CDY were responsible for manuscript writing and revision; ZSZ, SLL, WJZ and CHJ participated in the data analysis; and all authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chen, HJ., Chen, DY., Zhou, Sz. et al. Combined anterior and posterior approach in treatment of ankylosing spondylitis-associated cervical fractures: a systematic review and meta-analysis. Eur Spine J 32, 27–37 (2023). https://doi.org/10.1007/s00586-022-07435-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-022-07435-0