
Abstract
Introduction
The natural history of cervical spine lesions in rheumatoid arthritis (RA) is variable. We have actively performed occipito-thoracic fusion for severe destructive rheumatoid cervical disorders and reported its clinical results and complications. In our previous study, the most frequent complication was the adjacent-level failures caused by the fragile spine. The objective of this study was to determine risk factors for adjacent-level failures after occipito-thoracic fusion.
Materials and Methods
Subjects were 35 RA patients (31 females and 4 males) who underwent occipito-thoracic fusion using RRS Loop Spinal System® (Robert Reid Inc. Tokyo, Japan), and the incidence and characteristics of adjacent-level failures were investigated. Furthermore, the adjacent-level failures were divided into two types according to their levels, fracture at the lowest level of the fusion area and that at the level inferior to the fusion area, and the characteristics of each type were evaluated.
Results and Conclusion
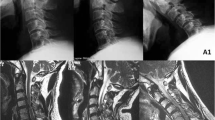
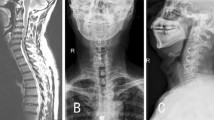
Nine (26 %) of 35 patients suffered adjacent-level failures (10 vertebral fractures). Adjacent-level failures occurred when the distance of fixation was “O–T4” or longer. The long fusion might cause adjacent-level failures due to greater mechanical stress. Seven fractures occurred at the lowest level of the fusion area, and all of them were cured without symptoms by conservative treatment. Three fractures occurred at the level inferior to the fusion area, and one of them needed additional surgery due to sudden paraplegia resulting from collapse of the adjacent vertebra. After occipito-thoracic fusion, burst fractures at the level inferior to the fusion area might cause sudden paraplegia, and therefore a careful observation should be required for patients with these fractures.





Similar content being viewed by others

References
Ochi T, Iwase R, Yonemasu K et al (1988) Natural course of joint destruction and fluctuation of serum C1q levels in patients with rheumatoid arthritis. Arthritis Rheum 31(1):37–43
Omura K, Hukuda S, Katsuura A et al (2002) Evaluation of posterior long fusion versus conservative treatment for the progressive rheumatoid cervical spine. Spine 27(12):1336–1345
Matsuyama Y, Kawakami N, Yoshihara H et al (2005) Long-term results of occipitothoracic fusion surgery in RA patients with destruction of the cervical spine. J Spinal Disord Tech 18(Suppl):S101–S106
Shimizu T, Tanouchi T, Ino M et al (2009) Revision surgeries following cervical fusion in rheumatoid arthritis: What should we learn from these cases?. In: 38th annual meeting of Japanese Society for Spine Surgery and Related Research Abstract book, p 380
Tanouchi T, Shimizu T, Fueki K et al (2012) Neurological improvement and prognosis after occipito-thoracic fusion in patients with mutilating-type rheumatoid arthritis. Eur Spine J 21(21):2506–2511
Tanouchi T, Shimizu T, Fueki K et al (2008) Complication and prognosis after occipito-thoracic fusion in mutilating type of rheumatoid arthritis. In: 37th annual meeting of Japanese Society for Spine Surgery and Related Research Abstract book, pp 79–80
Shimizu T, Edakuni H, Shimada H et al (1996) Occipito-cervical, thoracic fusion. In: Koichiro Hayashi (ed) OS now No21. Medical view, Tokyo, pp 35–47 In Japanese
Hirano K, Matsuyama Y, Sakai Y et al (2010) Surgical complications and management of occipitothoracic fusion for cervical destructive lesions in RA patients. J Spinal Disord Tech 23(2):121–126
Ishi K, Matsumoto M, Takahashi Y et al (2010) Risk factors for development of subaxial subluxations following atlantoaxial arthrodesis for atlantoaxial subluxations in rheumatoid arthritis. Spine 35:1551–1555
Iizuka H, Iizuka Y, Kobayashi R et al (2013) Effect of a reduction of the atlanto-axial angle on the cranio-cervical and subaxial angles following atlanto-axial arthrodesis in rheumatoid arthritis. Eur Spine J 22(5):1137–1141
Mori K, Imai S, Omura K et al (2010) Clinical output of the rheumatoid cervical spine in patients with mutilating-type joint involvement: for better activities of daily living and longer survival. Spine 35(13):1279–1284
Kraus DR, Peppelman WC, Agarwal AK et al (1991) Incidence of subaxial subluxation in patients with generalized rheumatoid arthritis who have had previous occipital cervical fusions. Spine 16:S486–S489
Matsunaga S, Ijiri K, Koga H (2000) Results of a longer than 10-year follow-up of patients with rheumatoid arthritis treated by occipitocervical fusion. Spine 25:1749–1753
Mori T, Matsunaga S, Sunahara N et al (1998) 3- to 11-year followup of occipitocervical fusion for rheumatoid arthritis. Clin Orthop Relat Res 351:169–179
Song KJ, Choi BW, Jeon TS, Lee KB, Chang H (2011) Adjacent segment degenerative disease: is it due to disease progression or a fusion-associated phenomenon? Comparison between segments adjacent to the fused and non-fused segments. Eur Spine J 20(11):1940–1945
Song KJ, Lee SK, Song JH, Choi BY (2009) The comparison of multi-level fusion versus one-level fusion to the development of adjacent level degeneration in anterior cervical arthrodesis with PEEK cage and plate augmentation for the degenerative cervical spinal disorders. J Korean Orthop Assoc 44(6):613–618
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tanouchi, T., Shimizu, T., Fueki, K. et al. Adjacent-level failures after occipito-thoracic fusion for rheumatoid cervical disorders. Eur Spine J 23, 635–640 (2014). https://doi.org/10.1007/s00586-013-3128-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-013-3128-3