
Abstract
Introduction
Gait impairment is a primary symptom of cervical spondylotic myelopathy (CSM); however, little is known about specific kinetic and kinematic gait parameters. The objectives of the study were: (1) to compare gait patterns of people with untreated CSM to those of age- and gender-matched healthy controls; (2) to examine the effect of gait speed on kinematic and kinetic parameters.
Materials and methods
Sixteen patients with CSM were recruited consecutively from a neurosurgery clinic, and 16 healthy controls, matched to age (±5 years) and gender, were recruited for comparison. Patients and controls underwent three-dimensional gait analysis using a Vicon® motion analysis system, at self-selected speed over a 10-m track. Controls were also assessed at the speed of their CSM match.
Results
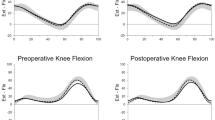
At self-selected speed, the CSM group walked significantly more slowly, with shorter stride lengths and longer double support duration. They showed significant decreases in several kinematic and kinetic parameters, including sagittal range of motion at the hip and knee, ankle plantarflexion, anteroposterior ground reaction force (GRF) at toe-off, power absorption at the knee in loading response and terminal stance, and power generation at the ankle. At matched speed, the CSM group showed significant decreases in knee flexion during swing, total sagittal knee range of motion, peak ankle plantarflexion and anteroposterior GRF.
Conclusion and implications
The findings suggested that people with CSM have significant gait abnormalities that have not been previously reported. In particular, there are key differences in the motor strategies used in the terminal stance phase of gait that cannot be explained by speed alone.


Similar content being viewed by others


References
Gough M, Shortland AP (2008) Can clinical gait analysis guide the management of ambulant children with bilateral spastic cerebral palsy? J Pediatr Orthop 28(8):879–883
Chen G, Patten C, Kothari DH, Zajac FE (2005) Gait differences between individuals with post-stroke hemiparesis and non-disabled controls at matched speeds. Gait Posture 22(1):51–56
Kuhtz-Buschbeck JP, Johnk K, Muder S, Stolze H, Mehdorn M (1999) Analysis of gait in cervical myelopathy. Gait Posture 9(3):184–189
Singh A, Crockard HA (1999) Quantitative assessment of cervical spondylotic myelopathy by a simple walking test. Lancet 354(9176):370–373
Singh A, Choi D, Crockard A (2009) Use of walking data in assessing operative results for cervical spondylotic myelopathy: long-term follow-up and comparison with controls. Spine (Phila Pa 1976) 34(12):1296–1300
Maezawa Y, Uchida K, Baba H (2001) Gait analysis of spastic walking in patients with cervical compressive myelopathy. J Orthop Sci Off J Jpn Orthop Assoc 6(5):378–384
Lee JH, Lee SH, Seo IS (2011) The characteristics of gait disturbance and its relationship with posterior tibial somatosensory evoked potentials in patients with cervical myelopathy. Spine (Phila Pa 1976) 36(8):E524–E530
Suzuki E, Nakamura H, Konishi S, Yamano Y (2002) Analysis of the spastic gait caused by cervical compression myelopathy. J Spinal Disord Tech 15(6):519–522
Hanlon M, Anderson R (2006) Prediction methods to account for the effect of gait speed on lower limb angular kinematics. Gait Posture 24(3):280–287
Patrick JH (2003) Case for gait analysis as part of the management of incomplete spinal cord injury. Spinal Cord 41(9):479–482
Moorthy RK, Bhattacharji S, Thayumanasamy G, Rajshekhar V (2005) Quantitative changes in gait parameters after central corpectomy for cervical spondylotic myelopathy. J Neurosurg Spine 2(4):418–424
Roislien J, Skare O, Gustavsen M, Broch NL, Rennie L, Opheim A (2009) Simultaneous estimation of effects of gender, age and walking speed on kinematic gait data. Gait Posture 30(4):441–445
Nurick S (1972) The Pathogenesis of the spinal cord disorder associated with cervical spondylosis. Brain 95:87–100
Japanese Orthopaedic Association (1994) Scoring system (17–2) for cervical myelopathy. J Jpn Orthop Assoc 68:490–503
Davis R, Ounpuu S, Tyburski D, Gage J (1991) A gait analysis data collection and reduction technique. Hum Mov Sci 10:575–587
Woltring HJ (1986) A fortran package for generalized, cross-validatory spline smoothing and differentiation. Adv Eng Softw UK 8(2):104–113
Williams G, Morris ME, Schache A, McCrory PR (2009) Incidence of gait abnormalities after traumatic brain injury. Arch Phys Med Rehabil 90(4):587–593
McDermott A, Bolger C, Keating L, McEvoy L, Meldrum D (2010) Reliability of three-dimensional gait analysis in cervical spondylotic myelopathy. Gait Posture 32(4):552–558
Winter DA (1985) Concerning the scientific basis for the diagnosis of pathological gait and for rehabilitation protocols. Physiother Can 37(4):245–252
Dietz V (2002) Proprioception and locomotor disorders. Nat Rev Neurosci 3(10):781–790
Anderson FC, Pandy MG (2003) Individual muscle contributions to support in normal walking. Gait Posture 17(2):159–169
Kirtley C (2006) Clinical gait analysis: theory and practice. Churchill Livingstone, London
Nadeau S, Gravel D, Arsenault AB, Bourbonnais D (1999) Plantarflexor weakness as a limiting factor of gait speed in stroke subjects and the compensating role of hip flexors. Clinical Biomechanics (Bristol, Avon) 14(2):125–135
Gage J (1991) Gait analysis in cerebral palsy. Cambridge University Press, Cambridge
Cook C, Brown C, Isaacs R, Roman M, Davis S, Richardson W (2010) Clustered clinical findings for diagnosis of cervical spine myelopathy. J Man Manip Ther 18(4):175–180
Acknowledgments
This work was funded by the Health Research Board of Ireland under grant number CTPF/2008/2.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Malone, A., Meldrum, D. & Bolger, C. Gait impairment in cervical spondylotic myelopathy: comparison with age- and gender-matched healthy controls. Eur Spine J 21, 2456–2466 (2012). https://doi.org/10.1007/s00586-012-2433-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-012-2433-6