
Abstract
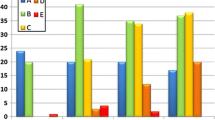
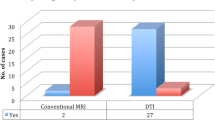
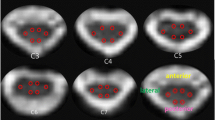
There are discrepancy between MR findings and clinical presentations. The compressed cervical cord in patients of the spondylotic myelopathy may be normal on conventional MRI when it is at the earlier stage or even if patients had severe symptoms. Therefore, it is necessary to take a developed MR technique—diffusion tensor imaging (DTI)—to detect the intramedullary lesions. Prospective MR and DTI were performed in 53 patients with cervical compressive myelopathy and twenty healthy volunteers. DTI was performed along six non-collinear directions with single-shot spin echo echo-planar imaging (EPI) sequence. Intramedullary apparent diffusion coefficient (ADC) and fractional anisotropy (FA) values were measured in four segments (C2/3, C3/4, C4/5, C5/6) for volunteers, in lesions (or the compressed cord) and normal cord for patients. DTI original images were processed to produce color DTI maps. In the volunteers’ group, cervical cord exhibited blue on the color DTI map. FA values between four segments had a significant difference (P < 0.01), with the highest FA value (0.85 ± 0.03) at C2/3 level. However, ADC value between them had no significant difference (P > 0.05). For patients, only 24 cases showed hyperintense on T2-weighted image, while 39 cases shown patchy green signal on color DTI maps. ADC and FA values between lesions or the compressed cord and normal spinal cord of patients had a significant difference (both P < 0.01). FA value at C2/3 cord is the highest of other segments and it gradually decreases towards the caudal direction. Using single-shot spin echo EPI sequence and six non-collinear diffusion directions with b value of 400 s mm−2, DTI can clearly show the intramedullary microstructure and more lesions than conventional MRI.








Similar content being viewed by others
References
Aota Y, Niwa T, Uesugi M, Yamashita T, Inoue T, Saito T (2008) The correlation of diffusion-weighted magnetic resonance imaging in cervical compression myelopathy with neurologic and radiologic severity. Spine 33:814–820
Baptiste DC, Fehlings MG (2006) Pathophysiology of cervical myelopathy. Spine J 6(6 Suppl):190S–197S
Baron EM, Young WF (2007) Cervical spondylotic myelopathy: a brief review of its pathophysiology, clinical course, and diagnosis. Neurosurgery 60(1suppl 1):35–41
Cercignani M, Horsefield MA, Agosta F, Filippi M (2003) Sensitivity-encoded diffusion tensor MR imaging of the cervical cord. AJNR 24:1254–1256
Clark CA, Barker GJ, Tofts PS (1999) Magnetic resonance diffusion imaging of the human cervical spinal cord in vivo. Magn Reson Med 41:1269–1273
Clark CA, Werring DJ (2002) Diffusion tensor imaging in spinal cord: methods and applications—a review. NMR Biomed 15:578–586
Clark CA, Werring DJ, Miller DH (2000) Diffusion imaging of the spinal cord in vivo: estimation of the principal diffusivities and application to multiple sclerosis. Magn Reson Med 43:133–138
Demir A, Ries M, Moonen CT, Vital JM, Dehais J, Arne P, Caillé JM, Dousset V (2003) Diffusion-weighted MR Imaging with apparent diffusion coefficient and apparent diffusion tensor maps in cervical spondylotic myelopathy. Radiology 229:37–43
Fehlings MG, Skaf G (1998) A review of the pathophysiology of cervical spondylotic myelopathy with insights for potential novel mechanisms drawn from traumatic spinal cord injury. Spine 23:2730–2737
Franconi F, Lemaire L, Marescaux L, Jallet P, Le Jeune JJ (2000) In vivo quantitative micro imaging of rat spinal cord at 7T. Magn Reson Med 44:893–898
Gulani V, Webb AG, Duncan ID, Lauterbur PC (2001) Apparent diffusion tensor measurements in myelin-deficient rat spinal cords. Magn Reson Med 45:191–195
Kaiser JA, Holland BA (1998) Imaging of the cervical spine. Spine 23:2701–2712
LaRocca H (1988) Cervical spondylotic myelopathy: natural history. Spine 13:854–855
Mamata H, Jolesz FA, Maier SE (2004) Characterization of central nervous system structures by magnetic resonance diffusion anisotropy. Neurochem Int 45:553–560
Moseley ME, Kucharczyk J, Mintorovitch J, Cohen Y, Kurhanewicz J, Derugin N, Asgari H, Norman D (1990) Diffusion-weighted MR imaging of acute stroke: correlation with T2-weighted and magnetic susceptibility-enhanced MR imaging in cats. AJNR 11:423–429
Ries M, Jones RA, Dousset V, Moonen CT (2000) Diffusion tensor MRI of the spinal cord. Magn Reson Med 44:884–992
Sampath P, Bendebba M, Davis JD, Ducker TB (2000) Outcome of patients treated for cervical myelopathy: a prospective, multicenter study with independent clinical review. Spine 25:670–676
Sinha S, Bastin ME, Whittle IR, Wardlaw JM (2002) Diffusion tensor MR imaging of high-grade cerebral gliomas. AJNR 23:520–527
Tsuchiya K, Katase S, Fujikawa A, Hachiya J, Kanazawa H, Yodo K (2003) Diffusion-weighted MRI of the cervical spinal cord using a single-shot fast spin-echo technique: findings in normal subjects and in myelomalacia. Neuroradiology 45:90–94
Wheeler-Kingshott CA, Hickman SJ, Parker GJ, Ciccarelli O, Symms MR, Miller DH, Barker GJ (2002) Investigating cervical spinal cord structure using axial diffusion tensor imaging. Neuroimage 16:93–102
Yukawa Y, Kato F, Yoshihara H, Yanase M, Ito K (2007) MR T2 image classification in cervical compression myelopathy: predictor of surgical outcomes. Spine 32:1675–1678
Acknowledgments
The manuscript submitted was supported by the Medical Science Foundation of the Department of Health of Guangdong Province (No.A2006529), the Medical Science Foundation of the Bureau of Health of Guangzhou city (No.2005-YB-040), and Doctoral Scientific Research Start-up Foundation of Guangzhou Medical College (No. 2006GD081). No benefits in any form have been or will be received from a commercial party related directly or indirectly to the subject of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Song, T., Chen, WJ., Yang, B. et al. Diffusion tensor imaging in the cervical spinal cord. Eur Spine J 20, 422–428 (2011). https://doi.org/10.1007/s00586-010-1587-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00586-010-1587-3