
Abstract
Purpose
Patients undergoing gynecological surgery are considered to be a high-risk cohort for postoperative nausea and vomiting (PONV). The purpose of this study was to assess the association of intraoperative end-tidal carbon dioxide (EtCO2) with risk of PONV in patients underwent gynecological open surgery.
Methods
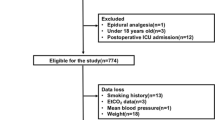
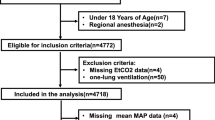
In this single-center retrospective observational study, we included patients aged 20–60 years who underwent elective gynecological open surgery. We obtained data for the incidence of PONV within 24 h after operation. We collected EtCO2 every minute during the operation, and determined the lowest value of EtCO2. We compared the lowest EtCO2 between patients with and without PONV. Multivariate logistic regression analysis was performed to assess the independent association of EtCO2 with the risk of PONV.
Results
A total of 146 patients were included in the current study. There were 81 patients with PONV within 24 h after the operation. The median lowest value of EtCO2 in patients with PONV was significantly lower than that in patients without PONV (31 vs 33 mmHg, p = 0.02). In the multivariate logistic regression model, we found that lowest EtCO2 ≤ 31 mmHg was independently associated with increase in the risk of PONV (adjusted odds ratio = 3.37, p = 0.02).
Conclusion
In this retrospective observational study, low intraoperative EtCO2 was shown to be independently associated with increased risk of PONV. However, this result may be skewed by uncollected information including previous PONV, motion sickness or other unknown bias, so future studies should be conducted to refute or confirm our findings.


Similar content being viewed by others

References
Gan TJ, Diemunsch P, Habib AS, Kovac A, Kranke P, Meyer TA, Watcha M, Chung F, Angus S, Apfel CC, Bergese SD, Candiotti KA, Chan MT, Davis PJ, Hooper VD, Lagoo-Deenadayalan S, Myles P, Nezat G, Philip BK, Tramer MR, Society for Ambulatory A. Consensus guidelines for the management of postoperative nausea and vomiting. Anesth Analg. 2014;118:85–113.
Myles PS, Williams DL, Hendrata M, Anderson H, Weeks AM. Patient satisfaction after anaesthesia and surgery: results of a prospective survey of 10,811 patients. Br J Anaesth. 2000;84:6–10.
Kenny GN. Risk factors for postoperative nausea and vomiting. Anaesthesia. 1994;49(Suppl):6–10.
Sarna GS, Obrenovitch TP, Matsumoto T, Symon L, Curzon G. Effect of transient cerebral ischaemia and cardiac arrest on brain extracellular dopamine and serotonin as determined by in vivo dialysis in the rat. J Neurochem. 1990;55:937–40.
Teramoto Y, Urano T, Nagai N, Takada Y, Ikeda K, Takada A. Plasma levels of 5-HT and 5-HIAA increased after intestinal ischemia/reperfusion in rats. Jpn J Physiol. 1998;48:333–9.
Watcha MF, White PF. Postoperative nausea and vomiting. Its etiology, treatment, and prevention. Anesthesiology. 1992;77:162–84.
Theye RA, Milde JH, Michenfelder JD. Effect of hypocapnia on cardiac output during anesthesia. Anesthesiology. 1966;27:778–82.
Hermes A. Kontos HPMJ, Richardson DW, Patterson JRJL. Circulatory responses to hypocapnia in the anesthetized dog. Am J Physiol. 1965;208(1):139–43.
Guzman JA, Kruse JA. Splanchnic hemodynamics and gut mucosal-arterial PCO(2) gradient during systemic hypocapnia. J Appl Physiol. 1985;1999(87):1102–6.
Laffey JG, Kavanagh BP. Hypocapnia. N Engl J Med. 2002;347:43–53.
Apfel CC, Laara E, Koivuranta M, Greim CA, Roewer N. A simplified risk score for predicting postoperative nausea and vomiting: conclusions from cross-validations between two centers. Anesthesiology. 1999;91:693–700.
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. The Lancet. 2007;370:1453–7.
Kanda Y. Investigation of the freely available easy-to-use software 'EZR' for medical statistics. Bone Marrow Transplant. 2013;48:452–8.
Saghaei M, Matin G, Golparvar M. Effects of intra-operative end-tidal carbon dioxide levels on the rates of post-operative complications in adults undergoing general anesthesia for percutaneous nephrolithotomy: a clinical trial. Adv Biomed Res. 2014;3:84.
Son JS, Oh JY, Ko S. Effects of hypercapnia on postoperative nausea and vomiting after laparoscopic surgery: a double-blind randomized controlled study. Surg Endosc. 2017;31:4576–82.
Apfel CC, Korttila K, Abdalla M, Kerger H, Turan A, Vedder I, Zernak C, Danner K, Jokela R, Pocock SJ, Trenkler S, Kredel M, Biedler A, Sessler DI, Roewer N, Investigators I. A factorial trial of six interventions for the prevention of postoperative nausea and vomiting. N Engl J Med. 2004;350:2441–51.
Borison HL. Area postrema: chemoreceptor circumventricular organ of the medulla oblongata. Prog Neurobiol. 1989;32:351–90.
Bunce KT, Tyers MB. The role of 5-HT in postoperative nausea and vomiting. Br J Anaesth. 1992;69:60S–S6262.
Koivuranta M, Laara E, Snare L, Alahuhta S. A survey of postoperative nausea and vomiting. Anaesthesia. 1997;52:443–9.
Acknowledgements
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
About this article

{kind=link}
Cite this article
Fujimoto, D., Egi, M., Makino, S. et al. The association of intraoperative end-tidal carbon dioxide with the risk of postoperative nausea and vomiting. J Anesth 34, 195–201 (2020). https://doi.org/10.1007/s00540-019-02715-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00540-019-02715-4