
Abstract
Purpose
Monitoring motor evoked potentials (MEPs) has been recognized as a highly reliable method to detect intraoperative spinal cord ischemia (SCI) in aortic repair. However, the data regarding the sensitivity and specificity of MEPs for predicting postoperative paraplegia are limited. We retrospectively assessed the value of intraoperative MEP amplitudes for predicting postoperative paraplegia.
Methods
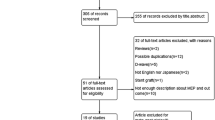
The medical records of 44 patients were reviewed. A train-of-five stimulation was delivered to C3–C4, and MEPs were recorded from the abductor pollicis brevis and the tibialis anterior muscles. The cutoff point for detecting SCI was set at 75% decrease of the baseline MEP. Receiver operating characteristic curves were applied at various cutoff points.
Results
Three patients (6.8%) had postoperative paraplegia. The minimum MEP during surgery had 100% sensitivity and 64.9% specificity in predicting paraplegia, and the MEP at the end of surgery had 66.7% sensitivity and 78.0% specificity in predicting paraplegia: only 1 patient, who had borderline paraplegia (right monoparesis), showed a false-negative result. Receiver operating characteristic curves indicated that adequate cutoff points for the minimum MEP during surgery and for the MEP amplitude at the end of surgery were a 75–90% decrease and a 64–75% decrease of the baseline MEP, respectively.
Conclusion
Monitoring MEPs had relatively high sensitivity and acceptable specificity, with the cutoff point set at 75% decrease of the baseline MEP, for predicting paraplegia and paraparesis. Because of the small sample in our study, further investigations would be necessary to investigate an adequate cutoff point that could predict postoperative paraplegia.







Similar content being viewed by others

References
Svensson LG, Crawford ES, Hess KR, Coselli JS, Safi HJ. Experience with 1509 patients undergoing thoracoabdominal aortic operations. J Vasc Surg. 1993;17:357–70.
Safi HJ, Estrera AL, Miller CC, Huynh TT, Porat EE, Azizzadeh A, Meada R, Goodrick JS. Evolution of risk for neurologic deficit after descending and thoracoabdominal aortic repair. Ann Thorac Surg. 2005;80:2173–9.
Bicknell CD, Riga CV, Wolfe JHN. Prevention of paraplegia during thoracoabdominal aortic aneurysm repair. Eur J Vasc Endovasc Surg. 2009;37:654–60.
Juvonen T, Biancari F, Rimpilainen J, Satta J, Rainio P, Kiviluoma K. Strategies for spinal cord protection during descending thoracic and thoracoabdominal aortic surgery: up-to-date experimental and clinical results- a review. Scand Cardiovasc J. 2002;36:136–60.
Coselli JS, Conklin LD, LeMaire SA. Thoracoabdominal aortic aneurysm repair: review and update of current strategies. Ann Thorac Surg. 2002;74:S1881–4.
Jacobs MJ, Mess W, Mochtar B, Nijenhuis EJ, Statius van Eps RG, Schrink GWH. The value of motor evoked potentials in reducing paraplegia during thoracoabdominal aneurysm repair. J Vasc Surg. 2006;43:239–46.
Solan TB. Electrophysiologic monitoring during surgery to repair the thoracoabdominal aorta. Semin Cardiothorac Vasc Anesth. 2004;8:113–25.
MacDonald DB, Janusz M. An approach to intraoperative neurophysiologic monitoring of thoracoabdominal aneurysm surgery. J Clin Neurophysiol. 2002;19:43–54.
Kakinohana M, Nakamura S, Fuchigami T, Miyata Y, Sugahara K. Influence of the descending thoracic aortic cross clamping on bispectral index values and plasma propofol concentration in humans. Anesthesiology. 2006;104:939–43.
Kawanishi Y, Munakata H, Matsumori M, Tanaka H, Yamashita T, Nakagiri K, Okada K, Okita Y. Usefulness of transcranial motor evoked potentials during thoracoabdominal aortic surgery. Ann Thorac Surg. 2007;83:456–61.
Shine TSJ, Harrison BA, De Ruyter ML, Crook JE, Heckman M, Daube JR, Stapelfeldt WH, Cherry KJ, Gloviczki P, Bower TC, Murray MJ. Motor and somatosensory evoked potentials. Their role in predicting spinal cord ischemia in patients undergoing thoracoabdominal aortic aneurysm repair with regional lumbar epidural cooling. Anesthesiology. 2008;108:580–7.
Keyhani K, Miller CC III, Estrera AL, Wegryn T, Sheinbaum R, Safi HJ. Analysis of motor and somatosensory evoked potentials during thoracic and thoracoabdominal aortic aneurysm repair. J Vasc Surg. 2009;49:36–41.
Murakami H, Tsukube T, Kawanishi Y, Okita Y. Transcranial myogenic motor-evoked potentials after transient spinal cord ischemia predicts neurologic outcome in rabbits. J Vasc Surg. 2004;39:207–13.
Kakinohana M, Abe M, Miyata Y, Oshiro M, Saikawa S, Arakaki K, Kuniyoshi Y, Sugahara K. Delayed response of transcranial myogenic motor-evoked potential monitoring to spinal cord ischemia during repair surgery for descending thoracic aortic aneurysm. J Anesth. 2008;22:304–7.
Lips J, de Haan P, Bouma GJ, Jacobs MJ, Kalkman CJ. Delayed detection of motor pathway dysfunction after selective reduction of thoracic spinal cord blood flow in pigs. J Thorac Cardiovasc Surg. 2002;123:531–8.
Griepp RB, Griepp EB. Spinal cord perfusion and protection during descending thoracic and thoracoabdominal aortic surgery: the collateral network concept. Ann Thorac Surg. 2007;83:S865–9.
Acher CW, Wynn M. A modern theory of paraplegia in the treatment of aneurysms of the thoracoabdominal aorta: an analysis of technique specific observed/expected ratios for paralysis. J Vasc Surg. 2009;49:1117–24.
Sakamoto T, Kawaguchi M, Kakimoto M, Inoue S, Takahashi M, Furuya H. The effect of hypothermia on myogenic motor-evoked potentials to electrical stimulation with a single pulse and a train of pulses under propofol/ketamine/fentanyl anesthesia in rabbits. Anesth Analg. 2003;96:1692–7.
Hollier LH, Money SR, Naslund TC, Proctor CD Sr, Buhrman WC, Marino RJ, Harmon DE, Kazmier FJ. Risk of spinal cord dysfunction in patients undergoing thoracoabdominal aortic replacement. Am J Surg. 1992;164:210–3.
Crawford ES, Crawford JL, Safi HJ, Coselli JS, Hess KR, Brooks B, Norton HJ, Glaeser DH. Thoracoabdominal aortic aneurysms: preoperative and intraoperative factors determining immediate and long-term results of operations in 605 cases. J Vasc Surg. 1986;3:389–404.
de Haan P, Kalkman CJ, de Mol BA, Ubags LH, Veldman DJ, Jacobs MJ. Efficacy of transcranial motor-evoked myogenic potentials to detect spinal cord ischemia during operations for thoracoabdominal aneurysm. J Thorac Cardiovasc Surg. 1999;113:87–100.
Safi HJ, Miller CC, Azizzadeh A, Ilipoulos D. Observations on delayed neurologic deficit after thoracoabdominal aortic aneurysm repair. J Vasc Surg. 1997;26:616–22.
Jacobs MJ, Meylaerts SA, de Haan P, de Mol BA, Kalkman CJ. Strategies to prevent neurologic deficit based on motor-evoked potentials in type I and II thoracoabdominal aortic aneurysm repair. J Vasc Surg. 1999;29:48–59.
Etz CD, Luehr M, Kari FA, Bodian CA, Smego D, Plestis KA, Griepp RB. Paraplegia after extensive thoracic and thoracoabdominal aortic aneurysm repair: does critical spinal cord ischemia occur postoperatively? J Thorac Cardiovasc Surg. 2008;135:324–30.
Acknowledgments
The authors thank Ms. Ryuko Imai, Mr. Tsunenori Takatani, Ms. Masami Yamanaka, and the other staff of the Central Clinical Laboratory (Nara Medical University, Kashihara, Nara, Japan) for their invaluable collaboration in monitoring MEPs in this study.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Horiuchi, T., Kawaguchi, M., Inoue, S. et al. Assessment of intraoperative motor evoked potentials for predicting postoperative paraplegia in thoracic and thoracoabdominal aortic aneurysm repair. J Anesth 25, 18–28 (2011). https://doi.org/10.1007/s00540-010-1044-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00540-010-1044-9