
Abstract.
Background/Purpose: Severe pancreatitis develops in 15% to 20% of patients with acute pancreatitis, morphologically characterized by extra- and intrapancreatic necrosis and associated with single or multiple organ failure. It is well accepted that surgery is indicated in patients with infected pancreatic necrosis. However, management of sterile necrosis is still controversial. In a prospective study, we evaluated the effect of maximal intensive care unit (ICU) treatment combined with prophylactic antibiotics in patients with necrotizing pancreatitis.
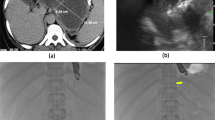
Methods: A total of 306 consecutive patients with acute pancreatitis were hospitalized between November 1993 and August 2001. All patients with necrotizing pancreatitis diagnosed by computed tomography received ICU treatment, including antibiotics (imipenem/cilastin). Fine-needle aspiration of pancreatic necrosis was performed in patients with clinical signs of sepsis, and necrosectomy combined with continuous postoperative lavage was indicated when bacterial testing demonstrated infection. In the presence of sterile necrosis, surgery was only performed when there was no clinical improvement despite maximal ICU treatment.
Results: Necrotizing pancreatitis was found in 121 patients. Infected necrosis was verified in 41 patients (34%) at a mean of 26 days. Four percent of patients with sterile necrosis and 95% of patients with infected necrosis were operated on. The surgical procedure was successful in 83% of patients as a single intervention; relaparotomy had to be performed in only 7 patients (17%). Pancreatic abscesses were found in 7 patients; four of these were drained interventionally. The overall mortality of the patients with necrotizing pancreatitis was 9.9%. The mortality of patients with sterile and infected necrosis was 2.5% and 24%, respectively (sterile vs infected; P < 0.01).
Conclusions: Due to improved intensive care treatment, including prophylactic antibiotics, surgical intervention is usually not indicated in the early course of severe acute pancreatitis. Surgery is clearly indicated in patients with proven infected necrosis. Patients with sterile necrosis should undergo surgery when there is no clinical improvement within 4 weeks of intensive care treatment. In the majority of patients a single intervention is sufficient. Reinterventions are rare and even in patients with abscess formation are not needed, because these can easily be drained interventionally.
Similar content being viewed by others


Author information
Authors and Affiliations
Additional information
Received: March 26, 2002 / Accepted: April 15, 2002
Offprint requests to: M.W. Büchler
About this article
Cite this article
Hartwig, W., Werner, J., Müller, C. et al. Surgical management of severe pancreatitis including sterile necrosis. J Hep Bil Pancr Surg 9, 429–435 (2002). https://doi.org/10.1007/s005340200053
Issue Date:
DOI: https://doi.org/10.1007/s005340200053