
Abstract
According to the World Health Organization, cardiovascular diseases contribute to 17.7 million deaths per year and are rising with a growing ageing population. In order to handle these challenges, the evolved countries are now evolving workable solutions based on new communication technologies such as ambient assisted living. In these solutions, the most well-known solutions are wearable devices for patient monitoring, telemedicine and mHealth systems. This systematic literature review presents the detailed literature on ambient assisted living solutions and helps to understand how ambient assisted living helps and motivates patients with cardiovascular diseases for self-management to reduce associated morbidity and mortalities. Preferred reporting items for systematic reviews and meta-analyses technique are used to answer the research questions. The paper is divided into four main themes, including self-monitoring wearable systems, ambient assisted living in aged populations, clinician management systems and deep learning-based systems for cardiovascular diagnosis. For each theme, a detailed investigation shows (1) how these new technologies are nowadays integrated into diagnostic systems and (2) how new technologies like IoT sensors, cloud models, machine and deep learning strategies can be used to improve the medical services. This study helps to identify the strengths and weaknesses of novel ambient assisted living environments for medical applications. Besides, this review assists in reducing the dependence on caregivers and the healthcare systems.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
Chronic conditions are impacting and burdening economies of countries around the world and contributing around 60 to 75% of deaths. These challenges lead to increasing the pressures on healthcare systems and have a serious impact on workforce shortages crisis [1, 2]. According to the World Health Organization, 31% of deaths have reported due to cardiovascular disease (CVD) [3]. An increase in the prevalence of long-term chronic conditions coupled with factors such as an ageing population acts as a growing contributory factor leading to a shift in the CVD incidence and mortality in older ages [4, 5]. This shift has led to an increased dependence on clinicians and caregivers for the management of multiple chronic conditions [6, 7]. It is reported and forecasted by United Nations in [8] that by the year 2050, 21% of the world’s population (nearly two billion people) will be more than 65 years of age [1, 9]. In Australia, this proportion is estimated to increase to 25% of the total population, leading to a potential quadrupling in healthcare costs and a higher incidence of life with disability [10,11,12]. Research shows that between 2002 and 2045, 50% of the total healthcare expenditure will be directed towards the ageing population, causing a large burden on the economy [10, 13].
Cardiovascular diseases are non-communicable diseases (NCDs), which are rapidly growing and burden for patients and their caregivers and shifted more towards the ageing population from the past two decades [14, 15]. The acceptance of modern technologies is increasing with the ease, quality and efficiency that they are bringing to the healthcare system [6, 15]. The people aged over 65 years lived in households living alone and needing assistance with at least one activity, healthcare, mobility, or self-care [11, 16]. The rising numbers of the ageing population with the need for high-level aged care require services that provide positive support to cater to the needs of this age group [17]. Increased consumer demand for wearable devices is making the demarcation between fitness and wearable medical devices indistinct [18]. Further value is added to these devices by the addition of other innovative techniques that assist in goal setting. They also enable interactive social support groups and rewards for achieving health-related milestones during treatment by gamification. The use of a gaming platform incentivizes, motivates and captures people’s interests, turning ubiquitous healthcare into a reality [19,20,21,22,23]. Living environments and digitization are now connected where devices are communicating with each other, by using various health applications, wearable watches and devices, smart clothes that are connected with infrastructure, Internet and cloud systems. These systems are making homes “medically smart” where patients are able to exchange the data and make changes to improve the user’s health and providing a support mechanism to live independently and manage their everyday activities [24,25,26,27].
Due to rapid development of new technologies and integrated networks, various healthcare monitoring applications have been designed to provide classification accuracies, scientifically assessment and computer-based classifications and analysis and for monitoring patient conditions. Healthcare sector is facing extraordinary issues and challenges due to the various different types of patterns of diseases, patient expectations and their financial matters, and rapidly increasing ageing population [28, 29]. There are various health conditions and factors distributed across the different levels and in subtle ways such as patient physical functions, anxiety, behaviour, social and environmental impacts and depression. The extraction of the required information is difficult due to various medical ontologies which have been adopted for data interpretation. A large amount of medical data brings tremendous issues and challenges. Various existing machine learning methods have been adopted for predictions in the healthcare sector, but still, many unaddressed challenges make this area in high dimensionality, temporal dependency, irregularity and sparsity [30,31,32,33]. Deep learning approaches have not been extensively reviewed in healthcare applications, especially for ambient assisted living. Deep learning methods are helpful for better and superior performance, integration, feature learning, handling complex and multi-modality data.
There is a need to conduct detail and systematic literature to highlight the impacts on patient’s treatment for better medical decisions. In this systematic literature review, we adopted the preferred reporting items for systematic reviews and meta-analyses (PRISMA) technique for research methodology. This review also helps to look into new and integrated information technologies to move the traditional systems towards the ambient assisted living environment. These new technologies will help to detect the diseases in earlier stages and reduce the dependence on caregivers.
This review is based on four main themes, main contributions of the paper, which are as follows:
-
Wearable technologies to self-monitor health for early detection of cardiovascular diseases.
-
CVDs in ageing population and the role of ambient assisted living (AAL).
-
Role of clinicians in providing treatments for patients who are digitally monitored.
-
Deep learning-based applications for biomedical data originated from wearable devices and other medical databases.
The rest of the paper is organized as follows: Sect. 2 presents the research methodology adopted for this systematic literature review and all possible questions and their answers to evaluate the state-of-the-art studies. Section 3 discusses the selected themes adopted to select the literature for further analysis. Section 4 illustrates the systematic literature review and technical aspects of all selected literature. Section 5 presents the discussion of this study. Section 6 presents the literature findings in positive and negative aspects. The last section concludes the paper with a future direction.
2 Research methodology
This systematic review is conducted and reported by adopting a PRISMA technique proposed by Moher et al. [34]. The next subsections present the detail of every step involved to achieve this research objective.
2.1 Information sources
The selection criteria of research articles are determined according to the population, intervention, comparison, outcomes and study design format. A comprehensive peer-reviewed literature search is conducted using the following databases: PubMed, Scopus, Springer, ScienceDirect, Medline (Ovid), Research Gate, Web of Science and ProQuest, to identify the most relevant published research from 2015 to 2019.
2.2 Literature selection criteria
Following the PRISMA statement, the following search strings are used for article extraction purposes, “ambient assisted living” OR “smart homes” OR “digital homes” OR “smart digital homes” AND “cardiovascular diseases” OR “heart disease” OR “heart attack” AND “self-management” OR “improved health” OR “reduced mortality” OR” reduced incidence of heart disease” AND “health monitoring” AND “deep learning for healthcare” AND “biomedical Informatics” AND “health-related outcomes” AND “quality of life” NOT “developing countries” NOT “poor countries”. Peer-reviewed, English-only articles from the past five years, with relevant titles, abstracts, objectives and conclusions, are initially selected. Further assessment of the quality of primary research is undertaken using the “QualSyst” quality assessment scoring system [35].
2.3 Literature selection results
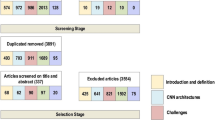
Figure 1 summarizes the assessment of evidence-based research articles at each stage. This initial search yielded 20,969 articles. Duplications are removed and reducing the articles to 17,866 where 10,000 are journal articles and 7866 articles are peer reviewed. The health informatics field is rapidly changing. Therefore, articles from the past five years are chosen; this reduced the search to 1877 articles. This is further reduced to 1775 articles when English-only articles are selected. A further review of the titles, abstracts and conclusions reduced the sample to 60 articles. A total of 40 articles are finalized using the QualSyst scoring system. Their review led to the identification of a set of four themes after being iteratively revised and hierarchically organized. The data are re-verified and checked in order to identify any missing information.

Assessment of evidence-based research articles
Individual scores for “yes”, “partial” and “no” are summed to create the Standard Quality Assessment Score (SQAS), which is given for each of the studies included in this review. The possible SQAS ranges from 0 to 20, with 0 indicating low quality and 20 indicating high quality. The main SQAS [34] is based on criteria which are as follows:
-
Question/objective sufficiently described.
-
Study design evident and appropriate.
-
Context for the study clear.
-
Connection to a theoretical framework/wider body of knowledge.
-
Sampling strategy described, relevant and justified.
-
Data collection methods clearly described and systematic.
-
Data analysis clearly described and systematic.
-
Use of verification procedure(s) to establish credibility.
-
Conclusions supported by the results.
-
Reflexivity of the account.
Inclusion and exclusion of the research articles criteria are presented in Table 1.
2.4 Data synthesis and analyses
A narrative synthesis is carried out based on the identified themes.
-
1.
Internet interventions and monitoring wearable devices/smartphones or personal digital assistant devices (PDAs) with software or applications for earlier detection, prevention and better self-management of cardiovascular diseases for an improved and healthier life.
-
2.
Role of ambient assisted living in aged populations with cardiovascular diseases.
-
3.
How the data generated by using these technologies can help the clinicians in treating patients with cardiovascular diseases.
-
4.
Use of deep learning for biomedical data originated from healthcare database (Fig. 2, Table 2).
Fig. 2 
Pie chart showing the percentage of occurrence of each theme in the selected articles
Table 2 Overall percentages of selected themes and selected literature

3 Selected themes and technologies
We divided the selected all literature on the basis of four main themes including self-monitoring devices and wearable technologies, ambient assisted the living, monitoring and clinician management and deep learning methods for cardiovascular diagnosis. We discussed these all themes for detail analysis.
3.1 Self-monitoring devices and wearable technologies
New technologies have altered the traditional healthcare services into new intelligent systems for self-monitoring. Small and wearable devices are used to share, monitor and collect the patient data for a healthy lifestyle [36]. Self-monitoring devices have Internet connections, sensors, GPS tracking systems, detectors, wireless technologies, small batteries, and a clock or display. These devices have gained popularity due to its portable lightweight structure and intelligent processes. Most popular self-monitoring devices are smartphones, wearable watches or wrist bands. These devices have well-designed applications and software to collect and monitor the data from patients by using patient vital signs. Mostly, the self-monitoring devices are portable, small in size, placeable, implantable and consumable. Various different types of sensors are placed in these devices enable with attachment mechanism with the body. These self-monitoring devices notified the patients to monitor instances. Placeable devices are another type of self-monitoring devices which are strategically located based on usage. These devices are also placed near patients and able to interact with other devices. These devices are not limited in size, battery power and processing capabilities [37, 38]. Self-monitoring devices have different services such as biometric systems, to proximate the person and sense patient body movements and functions such as heart rate, body temperature, pace, skin response and position tracking. The sportsman uses these devices for their fitness to collect and analyse the physical activities and collect calories intake, BMI (body mass index), blood pressure and other tracking activities. Some other devices are also designed for monitoring emotional status. Brain activities are also monitored but not so practice and applicable. Figure 1 shows the self-monitoring applications and their communication architecture (Fig. 3).

Self-monitoring applications and their communication architecture
3.2 Ambient assisted living
Ambient assisted living (AAL) refers to a solution for elderly people without any attendant where different types of management systems are used for preventing, curing and improving health and wellness conditions. These category tools and applications are used for medication management, notification of dosage, alerts and reminders to older people to control their health conditions. These applications provide safety and comfort by using mobile response systems, video surveillance and fall detection alerts. In addition, these systems are also helpful for daily activities by offering mobility capabilities. The systems also connect with elder’s attendants who are far away from elder people. These systems are based on smart and portable devices equipped with various sensor nodes such as gyroscope, accelerometer, GPS and detection and monitoring purposes. The new wearable sensor nodes are in the form of patches, body-worn devices and smart garments systems. The most popular ambient assisted living systems are used to monitor and sense blood pressure, glucose level and cardiac activity by using infrared sensing, oscillometric and optical sensing [39].
3.3 Monitoring and clinician management
With many benefits, the important factor is data delivery in time due to its seriousness and health-related information [40]. A number of wearable self-monitoring and AAL systems produced a huge amount of data that are stored in local databases or shifted to the cloud computing storage for further analysis. The data from homes and from other places are transferred to the medical centres and hospitals for further actions and processes. In-time data delivery is one of the major challenges due to complex and heterogeneous networks. Data handling and management is another challenge for medical centres. The emergency alerts need in time decisions for sending the immediate response to patients or to the ambulance, especially for cardiovascular patients. In-home monitoring systems, the accurate and in-time information should be delivered to clinics. Some applications are working on real-time information dissemination services such as hypertension patients to monitor their vital signs and provide immediate services. So there is a need to design more flexible patient care systems where the emergency messages management and handling require immediate medical attention. The main concern in these systems is how these types of patients alert handled by clinics or medical centres. In case, if some medical centre staff missed the information, then it has serious impacts on patient life.
3.4 Deep learning
Deep and machine learning has seen dramatic development and offered various methods and techniques to discover the complicated patterns from medical datasets. Deep learning has gained popularity due to its several analysis methods applied to complex and high-profile medical images and data. To recognize the objects from complex data is a difficult task for images, speech recognition, natural language processing and unstructured entities. Deep learning provides a wide range of techniques and is considered one of the well-known areas of research. In the healthcare sector, the data are captured in an enormous amount and then machine learning techniques are applied for further analysis and predictions. Various deep learning applications have been adopted for diagnosis, prediction, detection, discovery, operational efficiency and analysis of health records [41,42,43,44]. In the healthcare sector, machine learning has been adopted in general where deep learning is used particularly. Machine learning models are trained for feature extraction from raw data and then features learned by other machine learning models. On the other hand, in deep learning computers learn features and useful representations automatically by using direct raw data. This process is bypassing difficult and manual steps. The most popular deep learning methods are artificial neural networks. The only difference between machine and deep learning is manual and automatic features learning, and then, the discovered features are used to perform a task and improve the training process.
Deep learning methods are used for medical biomedical images and biomedical information such as medical records, medical images, signals and genomic sequences. Deep learning offers a variety of opportunities to handle a large amount of medical data for better decision-making. Deep learning methods have strong capabilities to determine the relationship between disease and its risk factors. A large amount of data have been collected all over the world but mostly the data do not consider any decision due to quality, inconsistency, instability, incompleteness, incongruence and multiple scale issues. Some other factors also make medical data more complex which are diversity or variety of multi-disciplinary fields such as signals, biology, computer science, math, instrumentation, medicine, pharmacy and physiology. One of the most popular projects initiated in 2015 was Medicine Initiative where they mapped the human genome of 1 million US citizens to extract the precise defects and primary cause of diseases at the genetic level and design new subset for molecular problems [45]. Deep learning and its related methods have a great role in medical and clinical research for decision management, low-cost solutions, control of diseases, in-time prediction and treatment and better efficiency. Deep learning architecture is based on several layers of neural networks where unsupervised deep learning is adopted to tune efficiency and extract deep structure for feature extraction. Figure 4 shows the deep learning architecture.

Deep learning architecture
4 Theme-wise systematic literature review of selected studies
This section presents the literature review on the selected studies which are divided into four main themes. The selected studied are evaluated in terms of different parameters as presented in tabular form in each theme subsection.
4.1 Wearable technologies to self-monitor health for early detection of cardiovascular diseases
Globally, CVD remains one of the most prevalent and costly public health issues. The E-health phenomenon has given rise to multi-domain, large-scale interventions, such as the app “Hello Heart” and “Healthy Ageing Through Internet Counselling in the Elderly” (HATICE) trial, providing coach-supported interactive platforms. The past five years have witnessed a significant increase in sensor-embedded, wearable technologies. In the digital era, health monitoring has been revolutionized by moving to self-powered wireless body computing technologies. The synchronization of all of these technologies and digital platforms create artificial intelligence to monitor and provide customized health predictions in an ambient assisted living environment to those who need care, “blurring the lines” between medicine and daily life. Undiagnosed atrial fibrillation (AF) costs the US government up to 3.1 billion dollars in 2014. Recent advances in telemonitoring, such as the smartphone-based monitoring apps, have reduced the relative risk of mortality caused by heart disease-related hospitalizations compared to the usual-care practices. Many patients with heart disease may have sleep apnoea or are unable to recognize the cause of their chest pain and may delay in seeking medical help.
This paper [46] explores how wearable context-aware ECG monitoring systems with kinematic sensors for continuous long-term monitoring are using a smartphone which can help to identify abnormalities in ECG and serve as a patient-friendly option to help and improve the data provided to clinicians for patients self-management. In another study [47], the authors discussed the wearable technologies and their vision and proposed wearable tracking technology. This wearable technology provides self-care and tracking capabilities with big data analytics. Big data analytics offers to navigate the consumers and provide better control related to their steps, sleep and other vital signs of health. Similarly, other self-monitoring devices in the ambient home environment have been developed for self-management, such as the direct cardiac rehabilitation wearable sensor, which informs heart patients about the level of exercise they would need to keep their heart rates in the target heart rate zone during exercise. Also, wearable activity trackers, such as Fitbit, Bodymedia, DirectLife, Jawbone Up or NikeFuel Band, can track multiple aspects and foster motivation, self-management for exercise and goal setting, which can serve crucial by filling in the blind spots and eliminating guesswork while collecting continuous data from patients of heart disease and providing information on exercise and activity in normal, free-living conditions.
Steinhubl et al. [48] focused on the use of wearable home-based monitoring devices for the earlier detection of cardiovascular episodes such as atrial fibrillation to provide opportunities for effective and economical screening for reduced associated mortalities and morbidities and better health outcomes. In this system, long-term, wearable, pulse-wave monitoring devices are connected via a smartphone app which is provided to participants in a trial to monitor continuously for any abnormalities in rhythm, which proved 100% effective in the detection of atrial fibrillation (AF), leading to early diagnosis, management and prevention of AF. Similarly, pacemakers and implantable cardioverter defibrillators with remote wireless Internet-based monitoring have markedly impacted time-to-event detection and decision-making from 22 to 4.6 days, reduced costs, mortality and morbidity and also safely reduced medical centre evaluations by 45%.
The study [49] presented the remote digital monitoring by the use of wireless body computing technologies such as implants, sensors and smartphones which are leading to the development of a more efficient virtual but continuous medical care system giving autonomy and power to the patient in managing his own health. This paper focuses on the integration of technologies to improve the overall patient experience by reducing costs and improving quality of care. In [50], the authors explored the positive impact on the quality of care, patient satisfaction and healthcare costs by using mobile health apps such as Hello Heart which supports patient engagement in self-measured blood pressure monitoring and provides the foundation for cardiovascular diseases. Applications such as Hello Heart provide platforms to enable patients to monitor and track self-recorded BP recordings with periodic reminders to measure BP, interactive educational modules and wireless connectivity with BP devices.
In [51], the authors discussed the benefits and different methods of monitoring, the recent changes and upgrades in home-based monitoring and its benefits for cardiovascular patients. Community-based ECG monitoring systems using smartphones, which collect personal physiological data and provide health-related information on self-monitoring and self-care especially for the elderly, are used for the cost-effective management and prevention of secondary CVD using technology from the comfort of their homes. It also utilizes the concept of gamification to drive user engagement with immediate personalized feedback, reward systems to maximize user interaction, positive reinforcement, progress reports, medication adherence and weight control promoting ownership of care. In [52], the authors discussed the importance of wearable devices in patient empowerment to ensure participation and decision-making in his health journey. Models with top-down approaches have been discussed to help achieve the objectives of a people-friendly cost-effective system.
Alharbi et al. [53] conducted a systematic literature review to assess the use of activity trackers as motivators of behaviour change for positive clinical outcomes in patients of heart failure. Another effort in [54] discussed cardiac monitoring to a higher and more reliable level using smartphone cameras to monitor heart rate by using images of fingertips. Other touchless methods based on optical sensors are also explored in this paper. The cameras as optical touchless sensors to detect the patient’s head motion and facial colour changes, due to blood pumping, are also being used to monitor the heart rate. Similarly, smartphone camera apps based on reflectance-mode photoplethysmography capture a fingertip placed on it, to determine the heart rate. In [55], the authors presented a wearable health device to monitor the vital signs monitoring of heart rate, blood pressure, blood glucose and electrocardiogram signals. Wearable devices are used for personal monitoring for single-parameter assessment and data transmission. This paper proposed a smart t-shirt for medical purposes which is a prototype solution for monitoring the cardiovascular signs. This system provides a low-cost solution after a detailed comparison of existing wearable devices.
In [56], the authors presented wearable devices for cardiac rhythm diagnosis and management. Wearable devices are discussed and analysed in the context of their performance of monitoring CVD signs and diagnose the sporadic arrhythmias. Limitations of wearable devices are also discussed where these technologies avoided inappropriate reliance for diagnosis purposes. In [57], the authors proposed a wrist-worn tracking device for monitoring CVD patients by using heart rate and energy expenditure. This watch helps patients for cardiac rehabilitation. This watch also helps to overestimate the energy expenditure in a group of patients. In [58], the authors discussed the existing and forthcoming devices for measuring the heart vital signs like heart rate, theoretic fluid and heart rhythm. The author also presented several frameworks for classification and a better understanding of wearable devices.
Contribution of smartphones and IT interventions using technologies such as user interface, real-time calculations and Bluetooth have transformed healthcare direction from being population-based to personalized medicine. Early detection of cardiac changes at a faster pace can help in providing patients with time medical help and also provide doctors with quality data due to continuous monitoring accurate diagnosis and better treatment options. Therefore, a reliable monitoring system can help by prompting the patient to seek medical care promptly, in case of an emergency. Table 3 presents wearable technologies with different parameters.
4.2 Role of ambient assisted living in aged populations with cardiovascular diseases
Ambient assisted living (AAL) is a cost-effective and personalized method by which the ageing populations, prone to chronic diseases, can spend healthier lives with no medical training in non-controlled environments such as their homes. Using sensors, accelerometers, glucometers, electrocardiography ECG and electroencephalography EEG (sensors), which are self-modular, cost-efficient, self-contained flexible and portable, is easily adapted to suit the needs of any person. In addition, home or self-monitoring can help reduce the inconvenience of visiting a doctor, at every problem a patient experiences. Systems such as the Health Buddy System connect patients with their physicians to reduce hospitalizations and Health@Home [60]. The project, a sensor-based wireless monitoring system for those affected by chronic heart failure, connects home-care systems with hospital information systems [23].
Adeluyi and Lee [61] discussed the role of various virtual instruments in ambient assisted living, especially in the aged populations for disease management, independent ageing and maintaining health and fitness. ECG sensors are interoperable and can be of various types such as galvanic skin response sensors (measuring the electric conductance of the skin), electromyography sensors (measure electrical activity in skeletal muscles), virtual sensors and smartphone-based sensors. The role of AAL is to provide an environment, especially for the high-risk ageing populations with CVD to age well and mitigate the high risk of mortality. In [62], the authors discussed the benefits of ambient assisted living to older individuals and their caregivers and also incorporated their point of views such as feeling more cared about and for with suggestions for change to make it more effective.
Richard et al. [63] focused on multiple internets based, at-home interventions for cardiovascular patients, customized to suit the needs of the individual for better self-management of cardiovascular diseases. This study shows that easy-to-use Internet platforms not only had greater acceptability among all age groups but also yielded positive long-term health impacts at reduced costs. In [64], the authors discussed the use of sensors in remote monitoring in ambient assisted living programs for patients with chronic conditions, especially aged patients to develop sustainable systems to provide pervasive health care. Effective frameworks comprise portable or wearable sensors to measure a patient’s physiological parameters and transmit them utilizing Bluetooth to a smartphone, which would analyse and forward the data to a medical centre and a health professional platform where it is reviewed by formal caregivers within the remote ambient assisted living system. This system would promote reactive services empowering patients for better self-management and proactive services initiated by the system reinforcing patient safety.
In [65], the authors presented solutions such as the use of robotics in rapidly ageing populations with age-related impairments that have been discussed in this paper. Smart-home environments, integrated sensors and assistive robotics are now used to help older people in improving their quality of life and live independently for longer. By the year 2020, the world will face an immense shortage of health and social care workers, around two million only in Europe. The growing integration of robotics can help monitor and alert persons with chronic conditions to facilitate effective disease management. In [66], the authors identified the perceptions of seniors when using smart homes. It was seen that even though they at times found discomfort and difficulty in using technology, their perceived benefit to achieve better health outweighed the challenges associates. This article gives us an insight into the user’s experiences with smart homes. Various research studies have shown that in-home health monitoring in CVD with zero-effort technology may result in better self-management, risk factor control, improved quality of life and reduced hospital stays, without any patient burden, error or failure.
In [67], the authors discussed the usefulness of warble devices for elderly people ambient assisted living. Elderly people need more care and assistance for monitoring their health and for early detection parameters. In [68], the authors investigated the personal care needs of elderly people to enhance support and medical therapy. This study discussed the need for care to determine the significant parameters of technologies and suggested the best specific technology for living assisted services. This is a questionnaire-based study, and results indicated that smartwatches and smartphones are more acceptable devices compared to cameras and smart TV. In [69], the authors presented the healthcare monitoring system based on wireless sneer networks to monitor the patients and hospitals’ elderly people living in an ambient assisted environment. This system assists the monitoring of chronic diseases such as heart attack, cardiovascular diseases by using wearable and implant devices. Table 4 presents the ambient assisted solutions with some important parameters.
4.3 How the data generated by using these technologies can help the clinicians in treating patients with cardiovascular diseases
Cloud computing has gained popularity globally with its capability of handling hardware and software efficiently, especially in patients with hypertension, which is also a leading risk factor for CVD. The concept is applied in the development of a hypertension patient control H-PC tool which transmits blood pressure readings to health centres, which allows clinicians to monitor their patients in real time and to take immediate actions when needed, thus offering high reliability and flexibility. Frameworks of pervasive patient care, based on sensing devices in the AAL for patients with chronic illnesses, can detect event severity according to its significance, activating alerts to the patient for self-management, or the health centre if the event is of a severe nature that requires immediate medical attention. Digital tracking products and applications can actively supplement the myopic vantage of real-time experiences, using sensor technology and big data to detect changes in the body, which could be missed by the eyes of a doctor in real time. With the advent of technology digital stethoscopes, miniature pocket-sized echocardiography machines with colour Doppler connected to smartphones, implantable and wireless sensors, patients can record, monitor and disseminate their diagnostic findings to their physicians. In AAL, devices monitor a patient’s vital signs to obtain their physiological information using smart bands, digital scales and blood pressure monitors. The system then analyses the data to decide whether the patient needs to see a clinician, or there is a need to modify behaviour and self-manage. Another important aspect of AAL is the empowerment of patients by involving them in their treatment and disease process, increasing the flexibility of the doctor–patient communication process and reducing face to face appointments and costs, while improving patient monitoring and overall health.
In [70], the authors discussed a hypertension patient control computer application that allows patients to send their readings through cloud computing to their clinicians helping in the management of patient/clinician time, reducing patient waiting times and providing continuous data to clinicians for treatment. In [71], the authors discussed the basic principles, accuracy, clinical applications and reproducibility of cardiovascular for better feature tracking and prognostic implications. In [72], the authors discussed the health technologies for cardiovascular disease for prevention and management. This study also discusses the current challenges and gaps and future aspects. The authors discussed that mostly monitoring management focused on activity tracking and blood pressure monitoring. The authors discussed that the existing management monitoring system has suffered from small sample size and limited follow-up, which is not as accurate as cardiovascular patients need.
In [73], the authors presented a cloud-based model for healthcare system data gatherings for further decision-making. This system reduces the response time and provides more efficient tracking and monitoring systems to collect the data. This smart system offers various advantages like data collection, processing by using PaaS and SaaS cloud models. In [74], the authors presented the wearable 2.0 healthcare system to collect patient data for clinical management. This system is based on one wearable 2.0 clothing instead of wearable 1.0 devices (smartwatches, wrist band, blood pressure monitor). Table 5 presents the monitoring and clinician management studies and their important parameters.
4.4 Deep learning methods for cardiovascular diagnosis
After monitoring the patient data and involvement of new technologies, another important factor is feature extraction from data and transforming into suitable representations classification. The traditional process is complex and time-consuming where the experts need prior knowledge. In recent years, deep learning has gained popularity for computer vision and imaging tasks.
The authors in [75] proposed a deep learning approach for phenotyping from the patient electronic health record. In this approach, the four-layer conventional neural network is used for extracting features and predictions. The first layer is based on electronic health record matrices, and the second layer is used to extract the phenotypes. The third layer has max pooling for sparsity on detected phenotypes, and the fourth layer is designed for prediction. Authors in [76] proposed a CNN-based system by using the nine-layer ID to identify the heartbeats. The heartbeat is categorized into different types including non-ectopic, ventricular ectopic, supraventricular ectopic, fusion and unknown beats. Different experiments are conducted on noise and original datasets from which the high-frequency noise is removed by using filters. Arrhythmia database is used based on ECG signals derived from the MIT-BIH.
The authors in [77] presented a deep learning approach for cardiac arrhythmia detection by using ECG signal analysis. The deep learning approach quickly classifies cardiac arrhythmias. Another feature of this proposed technique is end-to-end structure instead of handcrafted feature extraction. The authors in [78] proposed a detection technique for cardiovascular disease by using deep learning. This automated system provides detection and classification capabilities to estimate the mammogram’s risk markers for coronary artery disease. Deep learning has been applied to this system to analyse the proposed approach. However, the scope of this study is limited and needs proper assessment to detect closer clinical translation. The authors in [79] proposed a deep learning-based technique that learns own features to discover the knowledge from retinal images. This model predicts the cardiovascular risk factor by using different features including systolic blood pressure and adverse cardiac events. This model also predicts the optic disc and blood vessels for further analysis.
The authors in [80] proposed a deep learning-based deformable model to design a fully automatic segmentation for MRI datasets. This model automatically detects the shapes of the left ventricle. In [81], the authors discussed heart diseases and presented a wearable intelligent system for the diagnosis of cardiac disease. This system is an intelligent decision support system based on low energy, detection of cardiac abnormalities and advanced processing capabilities. The five methods are used for feature extraction from various ECG signal registers and evaluated with different classifiers. Support vector machines (SVM) and decision trees (DT) are used in this system. The authors in [82] proposed a smart healthcare framework for ambient assisted living by using new technologies for daily life activities. This system is based on wearable devices and communication technologies to deliver smart healthcare services. This system is used to monitor the physical activities of elderly people. Data are collected from multiple wearable devices including right- and left-hand ankle and chest. Data are collected and the MapReduce technique and multinominal Naïve Bayes classifier are adopted to check the performance of system. Results indicated the 97.1% accuracy and the best solution for monitoring the health conditions of elderly people. This paper [83] presented the HealthFog system based on deep learning for the automatic diagnosis of heart diseases. This system is based on fog and edge computing by bringing the resources and provides low latency and low power consumption system. Deep learning is also implemented for data analysis. The system performance was evaluated in terms of power consumption, latency, accuracy and execution time. Table 6 presents the deep learning-based solutions for ambient assisted living.
In [84], the authors proposed a method by using deep learning networks and multi-model signals. In addition, SVM is also adopted for this model where the signals are divided into time windows of equal duration. Then, the features are extracted and the concentrated features classified. In [85], the authors proposed a system based on IoT devices, artificial intelligence and wearable devices. The authors discussed the important cardiovascular signals and based on these inputs developed a mobile-based cardiac care solution. These cardiac signals constitute an intelligent and robust feature space for the detection of different cardiac abnormalities. In [86], the authors proposed a fog based IoT model for remote area cardiovascular patients. This system also used deep learning methods for disease prediction to classify the eight main cardiovascular classes ranging from hypertension signals to chronic heart failure. This model is used to diagnose cardiovascular disease and provide better physical and dietary advice. Multi-class classification is used for feature selection.
5 Discussion
The amalgamation of health data with the use of information technology has the potential to revolutionize health care. However, pathways to achieve a fully digitalized healthcare system are obscured by various challenges. Various trials and pilot projects are being conducted to test the synchronization of wearables, sensors, interactive health platforms, patient-provider communication platforms and smartphones, in order to bring together a single ambient assistive home environment. The journey to make it an everyday norm acceptable and accessible to all remains a huge task. Understanding the rapidly shifting population dynamics, especially in developed countries with the older generations living longer and drastically reduced fertility rates, it is undeniable that replacing manpower with information technology is the only viable solution to take care of a rapidly ageing population [9, 61]. The aged population with limited computer skills find it difficult to adapt to the rapidly changing technologies, which is another challenge [65]. Another unavoidable challenge is that it is difficult to ensure that the person is actually wearing the monitor continuously, because this could greatly impact the entire line of action of treatment and can be hazardous to the person in detecting and monitoring [48, 53]. Even though studies have concluded the use of wearable and monitoring technologies as a success, results may differ in long-term adherence with higher drop-offs when compared to short-term usage shown in experimental studies [63, 87, 88]. Also, the generalizability of these studies may be questionable when applied to the entire population [53, 87].
Health-related data are extremely sensitive in nature, needing highly credible systems to maintain its privacy, security, confidentiality and integrity because it can be exploited if it ends up with a stranger or a person with malicious intent [61]. As future interventions will use combinatorial innovations, maintaining the integrity, privacy multi-use concerns and security of health-related data being transmitted over multiple portals will be central to its success [53, 66, 70, 89]. Medical and health database breaches have been frequently reported, and medical data are a known target for fraudulent and illicit activities by cybercriminals and hackers [88]. In older generations, it was observed that their concern for maintaining the privacy of their personal dignity or financial information was much higher, resulting in a distrust of being constantly monitored in their homes [90].
Another challenge that was identified is the impact of tracking technologies leading to socioeconomic disadvantage and demotion. As the monitoring would become intense, it could lead to a coercive environment by stricter control enforced by employers or insurance companies to maintain fitness, where non-compliance could lead to consequences such as not being considered fit to work, reduced salaries or paying higher premiums to insurance companies [88]. Making monitoring technologies universally available and affordable in the commercial markets is yet another challenge, so they are not only available to those who are financially resilient, but available for all those who need it [66].
Technical barriers, especially of the body on sensors, including obstruction of signals due to motion artefacts, electromagnetic interferences, poor contact quality between sensor and skin, and baseline wander due to respiration can cause a deflection of the quality of the result [91]. Machine learning and artificial intelligence techniques working by converting raw data collected by sensors into actionable information were seen to be hampered by slow processing and time delays leading results with low accuracy, quality, limited scalability or reliability. Another important barrier is to shift the focus from using this technology for only data collecting purposes to a self-engaging and patient motivating system leading to user interaction acceptance and engagement. In some instances, the negative impacts of constant monitoring are known to cause stress as slight changes such as weight or BP fluctuations, which could trigger anxiety [66]. Calibration standardization practices of wearable activity trackers with clear cut methods to define intensity categories, monitoring periods and universally accepted definitions need to be developed, to bring them under the umbrella of universally accepted and adopted system [51, 53]. For a wider acceptance of the adoption of the wearable sensors, working on the simplicity, safety, aesthetics and customization of services is also a challenge to ensure its triumph with the people [53, 62].
Deep learning solutions have been implemented for feature extraction and disease prediction for CVD. With various benefits, these techniques still have suffered from several unsolved challenges. One of the significant challenges is handling big data volume, where deep learning-based highly intensive systems are fully connected. Different pieces of information and its extraction from a huge dataset are a fundamental issue. Various studies as discussed in the above themes section have utilized deep learning to link multiple data sources to make the joint knowledge for further analysis and prediction. However, existing methods of machine learning are not fully adopted, especially in ambient assisted living healthcare applications. The most common challenges are high-dimensionality, sparsity, irregularity and temporal dependency. These challenges are more complex when various medical ontologies are adopted to generalize the data.
6 Findings
After detailed discussion and checking all the parameters of the above-discussed themes, the main findings against each theme are as follows:
Theme-1: Wearable technologies to self-monitor health for early detection of cardiovascular diseases.
-
Existing wearable technologies have limited processing capabilities.
-
Faced difficulties to operate wearable devices and systems, especially in remote areas people.
-
Feeling discomfort with application interface and wearing devices.
-
Not so positive perceptions about wearable devices.
-
Patients are not mentally satisfied to wear these devices rather than visit the doctor physically.
-
Lack of trust in new technologies, especially old-age peoples, due to devices and technologies network pressure and fear.
-
Late decision to adopt wearable system due to financial factors.
Theme-2: CVDs in ageing population and the role of ambient assisted living (AAL).
-
Data privacy concerns due to open systems for data forwarding.
-
Malfunction concerns, where mostly patient discontinues the system due to maintenance and errors issues.
-
Multi-user concerns because the system is limited for one patient.
-
Affordability concerns due to the replacement of parts, batteries and nodes.
-
Adaptability issues, due to confusion about system results.
-
Awareness hurdles due to simple their knowledge and belief in new technologies.
-
Difficult to understand the application process and usage.
Theme-3: Monitoring and clinician management
-
Big data handling issues.
-
Updated information availability.
-
Independencies.
-
Risk mitigation that how to reduce negative effects on the data centre.
-
Security due to large systems placed openly in hospitals.
-
Expensive systems when using cloud services.
-
Real-time monitoring issues.
Theme-4: Deep learning-based applications for biomedical data originated from wearable devices and other medical databases.
-
Data overfitting issues.
-
Imbalanced dataset.
-
Data augmentation issues.
-
Choosing ideal hyper parameters.
-
Complex computational processing.
-
Power consumption.
-
Security and privacy.
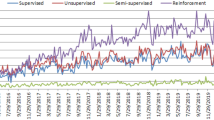
Although these all services and technologies have some limitations, these all systems are improving the accuracy and provision and prediction of cardiovascular diseases. The findings of this systematic literature review also concluded that these new wearable, smart-home, mHealth systems have gained popularity. Some wearable devices are popular in patients and will constantly increase their usage. According to the study [92], overall healthcare devices’ trend has increased as shown in Fig. 5.

Overall 3-year market trend analysis [92]
7 Conclusion
This century is marked with continuing and rapid progress in the field of healthcare and information technology transitioning with it to a new and dynamic era of digitization. Understanding that there is increasing pressure on the healthcare systems in the evolved countries due to increased ageing populations and health workforce shortages, expanding the role of digital technologies can help by the optimum allocation of existing resources, can promote more efficient patient monitoring and can also help in the early detection and prevention of various health conditions. It can also promote patient ownership in the management of his disease by enhanced engagement leading to improved patient health outcomes. The journey leading to a new and completely digitized world of health monitoring and management is on the horizon, which would revolutionize how health care is viewed.
Even though challenges and limitations exist to achieve a high level of digitization in our daily lives, technology advancement is gradually helping to overcome the limitations and make the impossible things into possible systems and achieve a world of endless possibilities. However, with various advantages, these new technology-based systems have suffered from some issues like adaptability, scalability, usage awareness, accuracy and data handling issues. This SLR will help the new researchers in the field of healthcare, especially for ambient living assisted applications and systems. The most available systems are using for cardiovascular disease all over the world. This paper discusses the wearable technologies role for early detection of cardiovascular diseases, the role of ambient assisted living (AAL), the role of clinicians in providing treatments for patients who are digitally monitored and, finally, deep learning-based applications for biomedical data originated from wearable devices and other medical databases.
References
Kenealy TW, Parsons MJG, Rouse APB, Doughty RN, Sheridan NF, Hindmarsh JKH, Masson SC, Rea HH (2015) Telecare for diabetes, CHF or COPD: effect on quality of life, hospital use and costs a randomised controlled trial and qualitative evaluation. PLoS ONE 10(3):e0116188
Lee H, Chung H, Ko H, Jeong C, Noh SE, Kim C, Lee J (2017) Dedicated cardiac rehabilitation wearable sensor and its clinical potential. PLoS ONE 12(10):e0187108
WHO (2019) Cardiovascular diseases (CVDs). http://www.who.int/mediacentre/factsheets/fs317/en/
Odden MCP, Coxson PGP, Moran AMDMPH, Lightwood JMP, Goldman LMDMPH, Bibbins-Domingo KPMD (2011) The impact of the aging population on coronary heart disease in the United States. Am J Med Ther 124(9):827–833.e5
Alanazi HO, Abdullah AH, Qureshi KN (2017) A critical review for developing accurate and dynamic predictive models using machine learning methods in medicine and health care. J Med Syst 41(4):69
Salisbury C, O’Cathain A, Thomas C, Edwards L, Gaunt D, Dixon P, Hollinghurst S, Nicholl J, Large S, Yardley L, Fahey T, Foster A, Garner K, Horspool K, Man MS, Rogers A, Pope C, Montgomery AA (2016) Telehealth for patients at high risk of cardiovascular disease: pragmatic randomised controlled trial. BMJ 353
Sarink D, Nedkoff L, Briffa T, Shaw JE, Magliano DJ, Stevenson C, Mannan H, Knuiman M, Peeters A (2016) Projected age- and sex-specific prevalence of cardiovascular diseases in Western Australian adults from 2005–2045. Eur J Prevent Cardiol 23(1):23–32
World Population Ageing 1950–2050 (2002) vol 17. Ringgold, Inc, Portland, p 69
Lin B-S, Wong AM, Tseng KC (2016) Community-based ECG monitoring system for patients with cardiovascular diseases. J Med Syst J 40(4):80
Ha NT, Hendrie D, Moorin R (2014) Impact of population ageing on the costs of hospitalisations for cardiovascular disease: a population-based data linkage study. BMC Health Serv Res 14(1):554
AIHW, “Australia`s Welfare 2017,” in “Australia`s welfare series no. 13,” AIHW, Canberra2017. https://www.aihw.gov.au/getmedia/088848dc-906d-4a8b-aa09-79df0f943984/aihw-aus-214-aw17.pdf.aspx?inline=true
Winefield H, O’Dwyer L, Taylor A (2016) Understanding baby boomer workers’ well-being in Australia. Aust J Ageing 35(3):E17–E21
Harris ML, Dolja-Gore X, Kendig H, Byles JE (2016) End of life hospitalisations differ for older Australian women according to death trajectory: a longitudinal data linkage study. BMC Health Serv Res 16(1):484
Milani RV, Bober RM, Lavie CJ (2016) The role of technology in chronic disease care. Progress Cardiovasc Dis 58(6):579–583
Anwar M, Abdullah AH, Altameem A, Qureshi KN, Masud F, Faheem M, Cao Y, Kharel R (2018) Green computing for wireless body area networks: energy efficient link aware medical data dissemination approach. Sensors 18(10):3237
Singh M, Stewart R, White H (2014) Importance of frailty in patients with cardiovascular disease. Eur Heart J 35(26):1726
AIHW (2017) Older Australia at a glance. https://www.aihw.gov.au/reports/older-people/older-australia-at-a-glance/contents/summary
Piwek L, Ellis DA, Andrews S, Joinson A (2016) The rise of consumer health wearables: promises and barriers. PLOS Med 13(2):e1001953
Chiauzzi E, Rodarte C, DasMahapatra P (2015) Patient-centered activity monitoring in the self-management of chronic health conditions. BMC Med 13(1):77
Vogel J, Auinger A, Riedl R, Kindermann H, Helfert M, Ocenasek H (2017) Digitally enhanced recovery: investigating the use of digital self-tracking for monitoring leisure time physical activity of cardiovascular disease (CVD) patients undergoing cardiac rehabilitation. PLoS ONE 12(10):e0186261
Car J, Tan WS, Huang Z, Sloot P, Franklin BD (2017) eHealth in the future of medications management: personalisation, monitoring and adherence. BMC Med 15:73
Miller AS, Cafazzo JA, Seto E (2016) A game plan: gamification design principles in mHealth applications for chronic disease management. Health Inf J 22(2):184–193
Hervás R, Fontecha J, Ausín D, Castanedo F, López-de-Ipiña D, Bravo J (2013) Mobile monitoring and reasoning methods to prevent cardiovascular diseases. Sensors (Switzerland) 13(5):6524–6541
Muse ED, Barrett PM, Steinhubl SR, Topol EJ (2017) Towards a smart medical home. Lancet 389(10067):358
Terry NP (2017) Will the Internet of things transform healthcare? Vanderbilt J Entertain Technol Law 19(2):327
Amiribesheli M, Benmansour A, Bouchachia A (2015) A review of smart homes in healthcare. J Ambient Intell Human Comput J 6(4):495–517
Aquino-Santos R, Martinez-Castro D, Edwards-Block A, Murillo-Piedrahita AF (2013) Wireless sensor networks for ambient assisted living. Sensors 13(12):16384–16405
Farhan W, Wang Z, Huang Y, Wang S, Wang F, Jiang XJJMI (2016) A predictive model for medical events based on contextual embedding of temporal sequences. JMIR Med Inf 4(4):39
Bengio Y, Lamblin P, Popovici D, Larochelle H (2007) Greedy layer-wise training of deep networks. In: Advances in neural information processing systems, pp 153–160
Litjens G, Kooi T, Bejnordi BE, Setio AAA, Ciompi F, Ghafoorian M, Van Der Laak JA, Van Ginneken B, Sánchez CIJMIA (2017) A survey on deep learning in medical image analysis. Med Image Anal 42:60–88
Lee J-G, Jun S, Cho Y-W, Lee H, Kim GB, Seo JB, Kim NJKJOR (2017) Deep learning in medical imaging: general overview. Korean J Radiol 18(4):570–584
Piccialli F, Di Somma V, Giampaolo F, Cuomo S, Fortino G (2021) A survey on deep learning in medicine: why, how and when? Inf Fusion 66:111–137
Piccialli F, Cuomo S, Crisci D, Prezioso E, Mei G (2020) A deep learning approach for facility patient attendance prediction based on medical booking data. Nat Sci Rep 10:14623. https://doi.org/10.1038/s41598-020-71613-7
Panic N, Leoncini E, de Belvis G, Ricciardi W, Boccia S (2013) Evaluation of the endorsement of the preferred reporting items for systematic reviews and meta-analysis (PRISMA) statement on the quality of published systematic review and meta-analyses. PLoS ONE 8(12):e83138
Leanne M, Kmet RCL, Cook LS (2004) Standard quality assessment criteria for evaluating primary research papers from a variety of fields. https://trove.nla.gov.au/version/227444865
Vinciguerra S, Vinciguerra M (2019) Smart devices and healthy aging. Nutr Healthy Aging 5(1):13–19
Qureshi KN, Bashir F, Abdullah AH (2018) An energy and link aware next node selection protocol for body area networks. In: 2018 International conference on information networking (ICOIN). IEEE, pp 721–726
Qureshi KN, Din S, Jeon G, Piccialli F (2020) Link quality and energy utilization based preferable next hop selection routing for wireless body area networks. Comput Commun 149:382–392
Rantz MJ, Skubic M, Koopman RJ, Phillips L, Alexander GL, Miller SJ, Guevara RD (2011) Using sensor networks to detect urinary tract infections in older adults. In: 2011 IEEE 13th international conference on e-health networking, applications and services. IEEE, pp 142–149
McGrath SP, Taenzer AH, Karon N, Blike G (2016) Surveillance monitoring management for general care units: strategy, design, and implementation. Joint Commiss J Qual Patient Saf 42(7):293–302
Shin H-C, Roth HR, Gao M, Lu L, Xu Z, Nogues I, Yao J, Mollura D, Summers RM (2016) Deep convolutional neural networks for computer-aided detection: CNN architectures, dataset characteristics and transfer learning. IEEE Trans Med Imaging 35(5):1285–1298
Kermany DS, Goldbaum M, Cai W, Valentim CC, Liang H, Baxter SL, McKeown A, Yang G, Wu X, Yan F (2018) Identifying medical diagnoses and treatable diseases by image-based deep learning. Cell 172(5):1122–1131
Katzman JL, Shaham U, Cloninger A, Bates J, Jiang T, Kluger Y (2018) DeepSurv: personalized treatment recommender system using a Cox proportional hazards deep neural network. BMC Med Res Methodol 18(1):24
Jiménez J, Skalic M, Martinez-Rosell G, De Fabritiis G (2018) K DEEP: protein–ligand absolute binding affinity prediction via 3D-convolutional neural networks. J Chem Inf Model 58(2):287–296
Terry SF (2015) Obama’s precision medicine initiative. Genetic Test Mol Biomark 19(3):113–114
Miao F, Cheng YY, He Y, He QY, Li Y (2015) A wearable context-aware ECG monitoring system integrated with built-in kinematic sensors of the smartphone. Sensors 15(5):11465–11484
Schull ND (2016) Data for life: wearable technology and the design of self-care. Biosocieties 11(3):317–333
Steinhubl SR, Mehta RR, Ebner GS, Ballesteros MM, Waalen J, Steinberg G, Van Crocker P, Felicione E, Carter CT, Edmonds S, Honcz JP, Miralles GD, Talantov D, Sarich TC, Topol EJ (2016) Rationale and design of a home-based trial using wearable sensors to detect asymptomatic atrial fibrillation in a targeted population: the mHealth screening to prevent strokes (mSToPS) trial. Am Heart J 175:77–85
Shinbane JS, Saxon LA (2016) Digital monitoring and care: virtual medicine. Trends Cardiovasc Med 26(8):722–730
Kaplan AL, Cohen ER, Zimlichman E (2017) Improving patient engagement in self-measured blood pressure monitoring using a mobile health technology. Health Inf Sci Syst 5(1):4
Michard F (2017) A sneak peek into digital innovations and wearable sensors for cardiac monitoring. J Clin Monit Comput 31(2):253–259
Ruiz-Fernandez D, Marcos-Jorquera D, Gilart-Iglesias V, Vives-Boix V, Ramirez-Navarro J (2017) Empowerment of patients with hypertension through BPM, IoT and remote sensing. Sensors 17(10):2273
Alharbi M, Straiton N, Gallagher R (2017) Harnessing the potential of wearable activity trackers for heart failure self-care. Curr Heart Fail Rep 14(1):23–29
Lomaliza J-P, Park H (2017) A highly efficient and reliable heart rate monitoring system using smartphone cameras. Multimed Tools Appl 76(20):21051–21071
Dias D, PauloSilvaCunha J (2018) Wearable health devices—vital sign monitoring, systems and technologies. Sensors 18(8):2414
Ip JE (2019) Wearable devices for cardiac rhythm diagnosis and management. JAMA 321(4):337–338
Falter M, Budts W, Goetschalckx K, Cornelissen V, Buys R (2019) Accuracy of apple watch measurements for heart rate and energy expenditure in patients with cardiovascular disease: cross-sectional study. JMIR mHealth uHealth 7(3):e11889
Pevnick JM, Birkeland K, Zimmer R, Elad Y, Kedan I (2018) Wearable technology for cardiology: an update and framework for the future. Trends Cardiovasc Med 28(2):144–150
Sohn K, Merchant FM, Sayadi O, Puppala D, Doddamani R, Sahani A, Singh JP, Heist EK, Isselbacher EM, Armoundas AA (2017) A novel point-of-care smartphone based system for monitoring the cardiac and respiratory systems. Sci Rep 7:44946
Sánchez-Tato I, Senciales JC, Salinas J, Fanucci L, Pardini G, Costalli F, Dalmiani S, de la Higuera JM, Vukovic Z, Cicigoj Z (2010) Health@ Home: a telecare system for patients with chronic heart failure. In: Fifth international conference on broadband and biomedical communications. IEEE, pp 1–5
Adeluyi O, Lee J-A (2015) Medical virtual instrumentation for ambient assisted living: part 1 concepts. Meas Control 48(6):167–177
Epstein I, Aligato A, Krimmel T, Mihailidis A (2016) Older adults’ and caregivers’ perspectives on in-home monitoring technology. J Gerontol Nurs 42(6):43–50
Richard E, Jongstra S, Soininen H, Brayne C, MollvanCharante EP, Meiller Y, Groep BVD, Beishuizen CR, Mangialasche F, Barbera M, Ngandu T, Coley N, Guillemont J, Savy S, Dijkgraaf MG, Peters RJ, Gool WAV, Kivipelto M, Anieu S, Stockholms U, Centrum för forskning om äldre och A, Samhällsvetenskapliga F (2016) Healthy ageing through internet counselling in the elderly: the HATICE randomised controlled trial for the prevention of cardiovascular disease and cognitive impairment. BMJ Open 6(6):010806
Triantafyllidis AK, Koutkias VG, Chouvarda I, Adami I, Kouroubali A, Maglaveras N (2016) Framework of sensor-based monitoring for pervasive patient care. Healthcare Technol Lett 3(3):153–158
Caleb-Solly P (2016) A brief introduction to … assistive robotics for independent living. Perspect Public Health 136(2):70–72
Grace SL, Taherzadeh G, Jae Chang IS, Boger J, Arcelus A, Mak S, Chessex C, Mihailidis A (2017) Perceptions of seniors with heart failure regarding autonomous zero-effort monitoring of physiological parameters in the smart-home environment. Heart Lung J Acute Crit Care 46(4):313–319
Kekade S, Hseieh C-H, Islam MM, Atique S, Khalfan AM, Li Y-C, Abdul SS (2018) The usefulness and actual use of wearable devices among the elderly population. Comput Methods Programs Biomed 153:137–159
Offermann-van Heek J, Schomakers E-M, Ziefle M (2019) Bare necessities? How the need for care modulates the acceptance of ambient assisted living technologies. Int J Med Inf 127:147–156
Buthelezi BE, Mphahlele M, Du Plessis D, Maswikaneng S, Mathonsi T (2019) ZigBee healthcare monitoring system for ambient assisted living environments. IJCNIS 11:1
Vilaplana J, Solsona F, Abella F, Cuadrado J, Teixidó I, Mateo J, Rius J (2015) H-PC: a cloud computing tool for supervising hypertensive patients. J Supercomput 71(2):591–612
Schuster A, Hor KN, Kowallick JT, Beerbaum P, Kutty S (2016) Cardiovascular magnetic resonance myocardial feature tracking: concepts and clinical applications. Circ Cardiovasc Imaging 9(4):e004077
Wongvibulsin S, Martin SS, Steinhubl SR, Muse ED (2019) Connected health technology for cardiovascular disease prevention and management. Curr Treat Options Cardiovasc Med 21(6):29
Yadav NS, Reddy BE, Srinivasa K (2018) Cloud-based healthcare monitoring system using Storm and Kafka. In: Towards extensible and adaptable methods in computing. Springer, pp 99–106
Chen M, Ma Y, Li Y, Wu D, Zhang Y, Youn C-H (2017) Wearable 2.0: enabling human-cloud integration in next generation healthcare systems. IEEE Commun Mag 55(1):54–61
Cheng Y, Wang F, Zhang P, Hu J (2016) Risk prediction with electronic health records: a deep learning approach. In: Proceedings of the 2016 SIAM international conference on data mining. SIAM, pp 432–440
Acharya UR, Oh SL, Hagiwara Y, Tan JH, Adam M, Gertych A, San Tan R (2017) A deep convolutional neural network model to classify heartbeats. Comput Biol Med 89:389–396
Yıldırım Ö, Pławiak P, Tan R-S, Acharya UR (2018) Arrhythmia detection using deep convolutional neural network with long duration ECG signals. Comput Biol Med 102:411–420
Wang J, Ding H, Bidgoli FA, Zhou B, Iribarren C, Molloi S, Baldi P (2017) Detecting cardiovascular disease from mammograms with deep learning. IEEE Trans Med Imaging 36(5):1172–1181
Poplin R, Varadarajan AV, Blumer K, Liu Y, McConnell MV, Corrado GS, Peng L, Webster DR (2018) Prediction of cardiovascular risk factors from retinal fundus photographs via deep learning. Nat Biomed Eng 2(3):158
Avendi M, Kheradvar A, Jafarkhani HJMIA (2016) A combined deep-learning and deformable-model approach to fully automatic segmentation of the left ventricle in cardiac MRI. Med Image Anal 30:108–119
Valenzuela O, Prieto B, Delgado-Marquez E, Pomares H, Rojas I (2018) Wearable intelligent system for the diagnosis of cardiac diseases working in real time and with low energy cost. Multidiscip Digit Publ Inst Proc 2(19):513
Syed L, Jabeen S, Manimala S, Alsaeedi A (2019) Smart healthcare framework for ambient assisted living using IoMT and big data analytics techniques. Future Gen Comput Syst
Tuli S, Basumatary N, Gill SS, Kahani M, Arya RC, Wander GS, Buyya R (2020) Healthfog: an ensemble deep learning based smart healthcare system for automatic diagnosis of heart diseases in integrated iot and fog computing environments. Future Gen Comput Syst 104:187–200
Hayashi T, Nishida M, Kitaoka N, Takeda K (2015) Daily activity recognition based on DNN using environmental sound and acceleration signals. In: 2015 23rd European signal processing conference (EUSIPCO). IEEE, pp 2306–2310
Ukil A, Bandyopadhyay S (2019) Automated cardiac health screening using smartphone and wearable sensors through anomaly analytics. In: Mobile solutions and their usefulness in everyday life. Springer, pp 145–172
Jabeen F, Maqsood M, Ghazanfar MA, Aadil D, Khan S, Khan MF, Mehmood I (2019) An IoT based efficient hybrid recommender system for cardiovascular disease. Peer-to-Peer Network Appl 1–14
Morawski K, Ghazinouri R, Icrumme A, McDonough J, Durfee E, Oley L, Mohta N, Juusola J, Choudhry NK (2017) Rationale and design of the medication adherence improvement support app for engagement blood pressure (MedISAFE-BP) trial. Am Heart J 186:40–47
Lupton D (2017) Self-tracking, health and medicine. Health Sociol Rev 26(1):1–5
Park LG, Beatty A, Stafford Z, Whooley MA (2016) Mobile phone interventions for the secondary prevention of cardiovascular disease. Progress Cardiovasc Dis 58(6):639–650
Lie MLS, Lindsay S, Brittain K (2016) Technology and trust: older people’s perspectives of a home monitoring system. Ageing Soc 36(7):1501–1525
Baig MM, GholamHosseini H, Moqeem AA, Mirza F, Lindén M (2017) A systematic review of wearable patient monitoring systems—current challenges and opportunities for clinical adoption. J Med Syst 41(7):115
Hayward J, Chansin G, Zervos H (2017) Wearable technology 2017–2027: markets, players, forecasts. IDTexEx report
Funding
Open Access funding provided by Università degli Studi di Napoli Federico II.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest statement.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Qureshi, M.A., Qureshi, K.N., Jeon, G. et al. Deep learning-based ambient assisted living for self-management of cardiovascular conditions. Neural Comput & Applic 34, 10449–10467 (2022). https://doi.org/10.1007/s00521-020-05678-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00521-020-05678-w