
Abstract
Background
This study was undertaken to analyze the characteristics of fever after cancer chemotherapy in order to reduce unnecessary medical care.
Methods
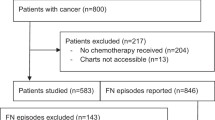
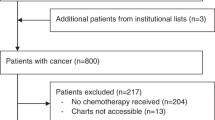
Retrospectively, 1016 consecutive cycles of cancer chemotherapy were analyzed. Fever was defined as a temperature of ≥37.5 °C lasting for 1 h. Age, sex, tumor histology, the treatment regimen, the timing of fever onset, the number of days for which the fever persisted, the cause of the fever, the presence or absence of radiotherapy, and the use of granulocyte colony-stimulating factor (G-CSF) were examined.
Results
The patients included 748 males and 268 females (median age = 68, range = 29–88), of whom 949, 52, and 15 were suffering from lung cancer, malignant pleural mesothelioma, and other diseases, respectively. Fever was observed in 367 cycles (36 %), including 280 cycles (37 %) involving males and 87 cycles (32 %) involving females. Fever occurred most commonly in the first cycles and was higher than later cycles (41 vs. 30 %, p < 0.001). Fever occurred most frequently on posttreatment days 4 (8 %), 3 (7 %), and 12 (7 %), and the distribution of fever episodes exhibited two peaks on posttreatment days 3 and 4 and 10–14. Fever on posttreatment days 3 and 4 was most commonly observed in patients treated with gemcitabine (20 %) or docetaxel (18 %). The causes of fever included infection (47 %; including febrile neutropenia [24 %]), adverse drug effects (24 %), unknown causes (19 %), and tumors (7 %). Radiotherapy led to a significant increase in the frequency of fever (46 vs. 34 %, p < 0.001). Thirty-three percent of patients received G-CSF, and the incidence ratios of fever in patients who received G-CSF were higher than those who did not receive G-CSF (44 vs. 31 %, p < 0.001).
Conclusion
The febrile episodes that occurred on posttreatment days 3 and 4 were considered to represent adverse drug reactions after cancer chemotherapy. Physicians should be aware of this feature of chemotherapy-associated fever and avoid unnecessary examination and treatments including prescribing antibiotics.


Similar content being viewed by others

References
Pizzo PA (1993) Management of fever in patients with cancer and treatment-induced neutropenia. N Engl J Med 328:1323–1332
Bennett CL, Djulbegovic B, Norris LB, Armitage JO (2013) Colony-stimulating factors for febrile neutropenia during cancer therapy. N Engl J Med 368:1131–1139
Kern WV, Marchetti O, Drgona L, Akan H, Aoun M, Akova M, de Bock R, Paesmans M, Viscoli C, Calandra T (2013) Oral antibiotics for fever in low-risk neutropenic patients with cancer: a double-blind, randomized, multicenter trial comparing single daily moxifloxacin with twice daily ciprofloxacin plus amoxicillin/clavulanic acid combination therapy—EORTC infectious diseases group trial XV. J Clin Oncol 31:1149–1156
Hong S, Tan M, Wang S, Luo S, Chen Y, Zhang L (2014) Efficacy and safety of angiogenesis inhibitors in advanced non-small cell lung cancer: a systematic review and meta-analysis. J Cancer Res Clin Oncol [Epub ahead of print]
Tabor PA (1986) Drug-induced fever. Drug Intell Clin Pharm 20:413–420
Mackowiak PA, LeMaistre CF (1987) Drug fever: a critical appraisal of conventional concepts. An analysis of 51 episodes in two Dallas hospitals and 97 episodes reported in the English literature. Ann Intern Med 106:728–733
Khurana A, Mitsis D, Kowlgi GN, Holle LM, Clement JM (2014) Atypical presentation of fever as hypersensitivity reaction to oxaliplatin. J Oncol Pharm Pract [Epub ahead of print]
Kimura H, Matsui Y, Ishikawa A, Nakajima T, Yoshino M, Sakairi Y (2015) Randomized controlled phase III trial of adjuvant chemo-immunotherapy with activated killer T cells and dendritic cells in patients with resected primary lung cancer. Cancer Immunol Immunother 64:51–59
Lortholary O, Lefort A, Tod M, Chomat AM, Darras-Joly C, Cordonnier C, Club de Reflexion sur les infections en Onco-Hematologie (2008) Pharmacodynamics and pharmacokinetics of antibacterial drugs in the management of febrile neutropenia. Lancet Infect Dis 8:612–620
Freifeld A, Marchigiani D, Walsh T, Chanock S, Lewis L, Hiemenz J, Hiemenz S, Hicks JE, Gill V, Steinberg SM, Pizzo PA (1999) A double-blind comparison of empirical oral and intravenous antibiotic therapy for low-risk febrile patients with neutropenia during cancer chemotherapy. N Engl J Med 341:305–311
Mayer K, Hahn-Ast C, Muckter S, Schmitz A, Krause S, Felder L, Bekeredjian-Ding I, Molitor E, Brossart P, von Lilienfeld-Toal M (2015) Comparison of antibiotic prophylaxis with cotrimoxazole/colistin (COT/COL) versus ciprofloxacin (CIP) in patients with acute myeloid leukemia. Support Care Cancer [Epub ahead of print]
Flowers CR, Seidenfeld J, Bow EJ, Karten C, Gleason C, Hawley DK, Kuderer NM, Landston AA, Marr KA, Rolston KV, Ramsey SD (2013) Antimicrobial prophylaxis and outpatient management of fever and neutropenia in adults treated for malignancy: American Society of Clinical Oncology clinical practice guideline. J Clin Oncol 31:794–810
Vanherik M (1965) Fever as a complication of radiation therapy for carcinoma of the cervix. Am J Roentgenol Radium Ther Nucl Med 93:104–109
Callen JP, Keskey K (1977) Fever as a complication of low dose irradiation. Br J Radiol 50:146–147
Finkelstein MS (1982) Unusual features of infections in the aging. Geriatrics 37:65–67
Keating 3rd HJ, Klimek JJ, Levine DS, Kiernan FJ (1984) Effect of aging on the clinical significance of fever in ambulatory adult patients. J Am Geriatr Soc 32:282–287
Norman DC, Grahn D, Yoshikawa TT (1985) Fever and aging. J Am Geriatr Soc 33:859–863
Adjogatse D, Thanopoulou E, Okines A, Thillai K, Tasker F, Johnston SR, Harper-Wynne C, Torrisi E, Ring A (2014) Febrile neutropaenia and chemotherapy discontinuation in women aged 70 years or older receiving adjuvant chemotherapy for early breast cancer. Clin Oncol 26:692–696
Conflict of interest
The authors declare that they have no competing interests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Ogawara, D., Fukuda, M., Ueno, S. et al. Drug fever after cancer chemotherapy is most commonly observed on posttreatment days 3 and 4. Support Care Cancer 24, 615–619 (2016). https://doi.org/10.1007/s00520-015-2820-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00520-015-2820-8